




The high prevalence of forefoot pathology generates long surgical waiting lists (SWL). We have detected a considerable number of patients who withdraw surgery, which creates an important distortion in our activity and high expenditure of resources. Our objective is to study the factors related to these resignations, as well as, compare them with other pathologies of high prevalence and ambulatory surgical treatment: carpal tunnel syndrome (CTS) and internal meniscopathy (IM).
Material and methodsRetrospective study of the surgical cancellations on 2399 patients included in the SWL of the Foot and Ankle Unit of our centre for forefoot surgery, between January/2014 and March/2018, both included.
ResultsWe have found 389 renunciations, which represent 16.22% of the inclusions in SWL, with 84.83% of women. The pathologies with the highest rate of resignation have been Morton metatarsalgia (24%) and hallux rigidus (20.16%). The most frequent pathology, hallux valgus, records 15.96% of resignations that occur mostly between 6 and 9 months. In the CTS and IM, the resignation rate has been 17.42 and 8.92%, respectively, with higher resignation rates in the first 3 months.
ConclusionsThe withdrawal of a scheduled intervention on the forefoot registers a high frequency in our environment, which can be related to factors such as the type of pathology, its natural history, response to orthopedic interventions, time in LEQ, and other non-specific ones on which we must investigate, to rationalize and establish duties in our SWL.
La alta prevalencia de la patología del antepié genera largas listas de espera quirúrgica (LEQ). Hemos detectado un considerable número de pacientes que renuncian a la cirugía, lo que crea una importante distorsión en nuestra actividad y un elevado gasto de recursos. Nuestro objetivo es estudiar los factores relacionados con estas renuncias, así como comparar con otras patologías de alta prevalencia y tratamiento quirúrgico ambulatorio: síndrome del túnel carpiano (STC) y la meniscopatía interna (MI).
Material y métodosEstudio retrospectivo de las renuncias a la intervención sobre 2.399 pacientes incluidos en LEQ de la Unidad de Pie y Tobillo de nuestro centro para cirugía del antepié, entre enero/2014 y marzo/2018, ambos inclusive.
ResultadosHemos encontrado 389 renuncias, lo que supone un 16,22% de las inclusiones en LEQ, siendo un 84,83% mujeres. Las patologías con mayor tasa de renuncia han sido: metatarsalgia de Morton (24%) y hallux rígidus (20,16%). La patología mas frecuente, el hallux valgus, registra un 15,96% de renuncias que se producen mayoritariamente entre los 6 y 9 meses. En el STC y la MI, el índice de renuncias ha sido del 17,42 y del 8,92% respectivamente, con mayores tasas de renuncia en los 3 primeros meses.
ConclusionesLa renuncia a una intervención programada sobre el antepié registra una alta frecuencia en nuestro medio, que puede relacionarse con factores como el tipo de patología, historia natural, respuesta a intervenciones ortopédicas, el tiempo en LEQ, y otros no determinados sobre los que debemos profundizar, para racionalizar y establecer prioridades en nuestras LEQ.
In health systems such as the Spanish one, in which coverage is practically complete and universal, with free access to all levels of medical care, the demand for diagnostic and therapeutic procedures usually exceeds system capacity, leading to waiting lists.1 The length of these lists depends on the incidence of the pathological processes in question as well as the nature of the diagnostic test or therapeutic procedure. It also depends on the healthcare catchment area and how it is managed, while factors such as age and comorbidities also have an influence.
Although waiting lists are neither the sole nor the best private or public healthcare system quality indicator, they directly affect public opinion, which sees them to reflect the response of the administration to the demand for care. They come to dominate the debate on healthcare and electoral programs, and they are at the core of the social and political life of the country. Orthopaedic surgery and traumatology is currently the speciality which generates the longest waiting lists for surgery (SWL) in the whole of the country.2 The causes which influence this are fundamentally3,4:
- •
The direct association of locomotor apparatus pathology with perceived quality of life.
- •
Increased life expectancy and active life duration in the population.
- •
The development of new more sophisticated surgical techniques with better results.
- •
Patients expect more and want to improve their functionality.
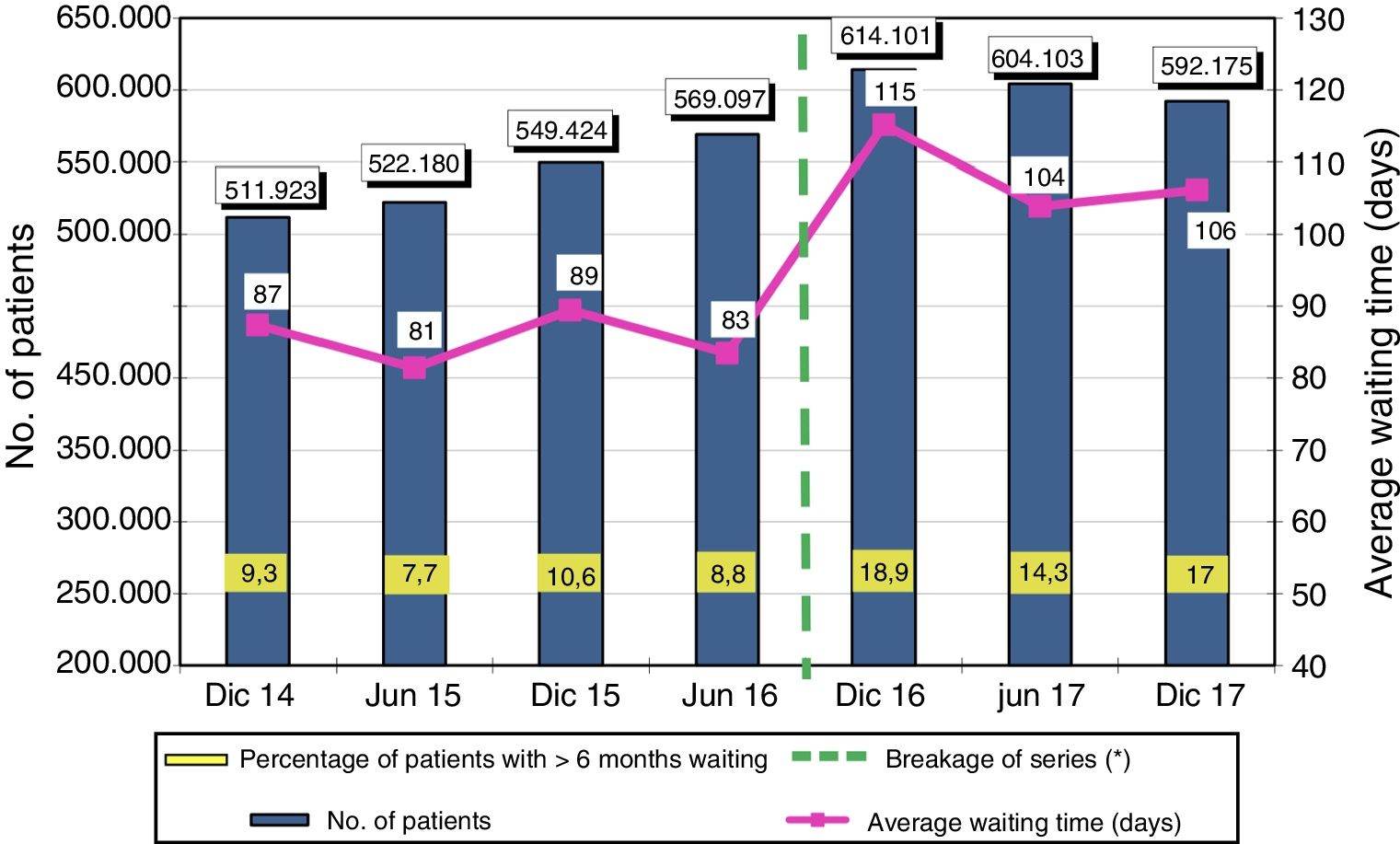
The growing demand for an increasingly broad range of services conflicts with management policy which aims to restrict spending. This leads to increasingly long SWL. Fig. 1 shows the total number of patients in planned waiting lists, the average time of waiting and the percentage of patients who waited for more than six months from 2014 to 2017, according to the SNS waiting list information system (SISLE-SNS).2

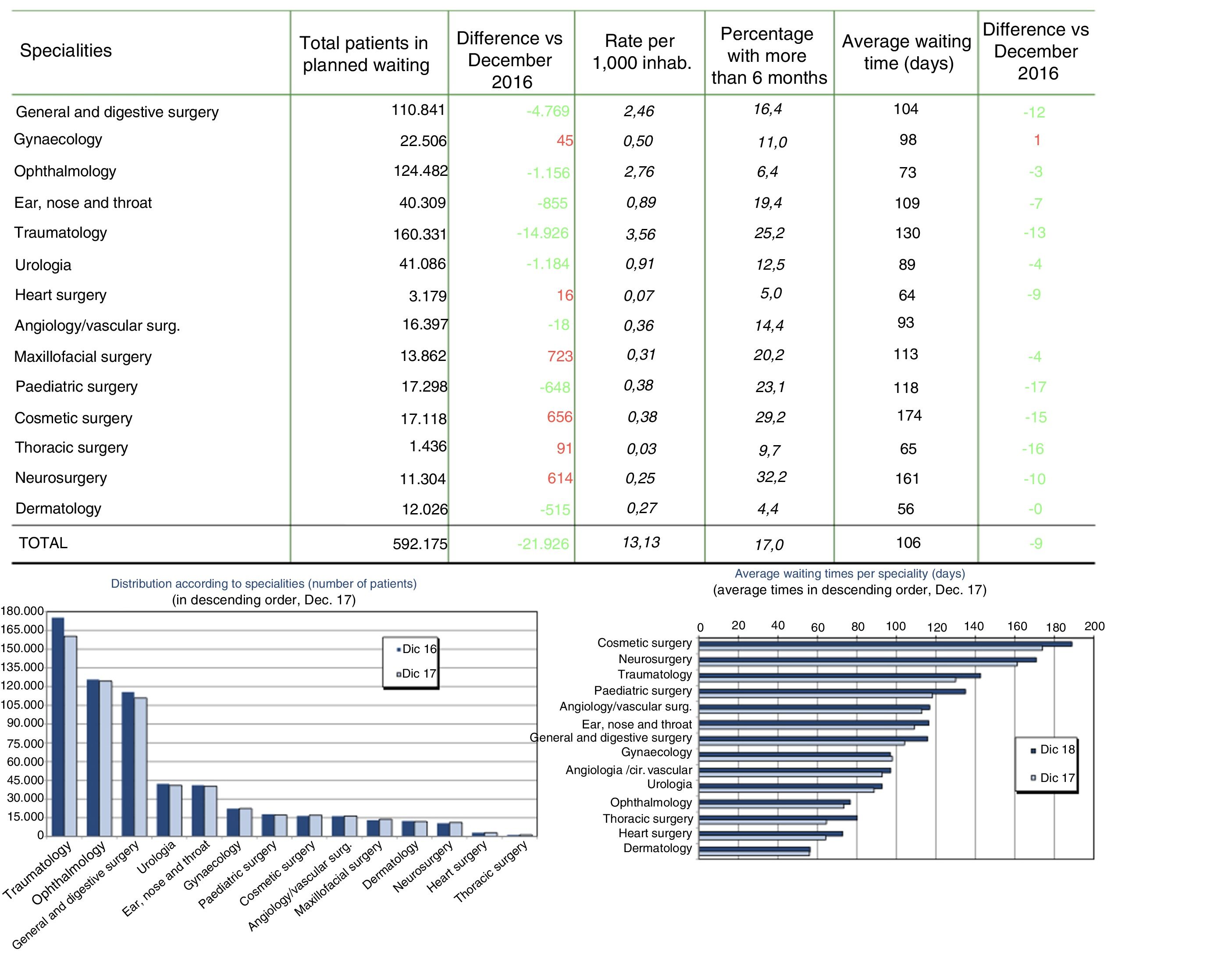
If we analyse the results according to speciality, it can be seen that the highest number of waiting patients corresponds to traumatology, with 160,331 patients. Their average waiting time amounted to 130 days, which was less than cosmetic surgery (174 days) and neurosurgery (161 days). The percentage of patients in a SWL for more than six months stands at 25.2% for traumatology, which is once again behind cosmetic surgery at 29.2% and neurosurgery at 32.2% (Fig. 2).

Forefoot pathology and more specifically hallux valgus (HV) is a very common cause of consultation in orthopaedic surgery and traumatology. Although its rate of prevalence in the general population is unknown,5 indications such as pain and deformity that hinders wearing normal footwear lead to long waiting lists. In our hospital, forefoot surgical operations usually take place under the major out-patient surgery regime.6
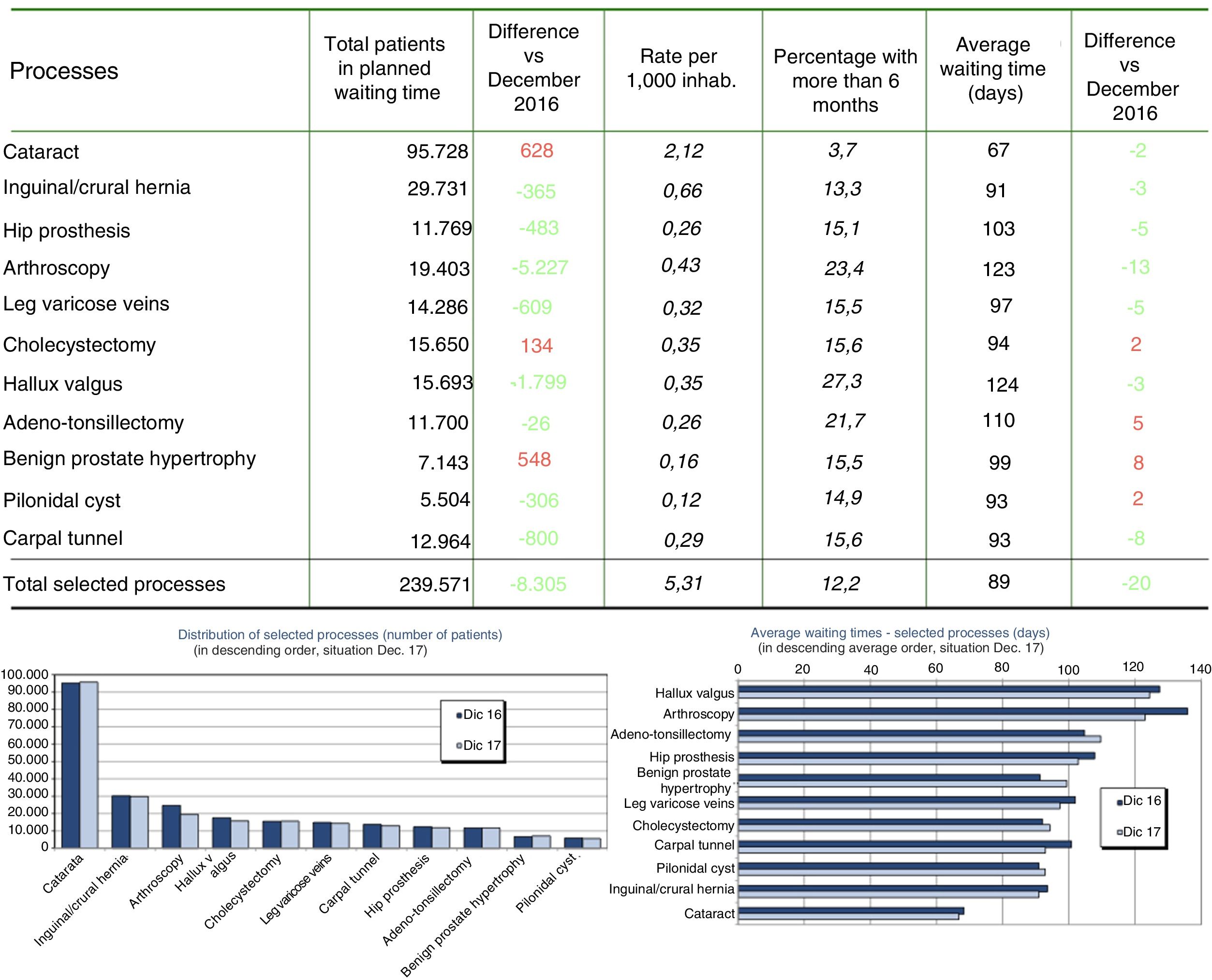
If we analyse the surgical waiting lists in the SNS on 31 December 2017 for selected processes, we find there are 15,693 patients in the planned waiting list for HV surgery. This amounts to a rate of 0.35 per thousand inhabitants, of which 27.3% waited for more than six months, while the average time to intervention was 124 days (Fig. 3).

Efficient management and use of human and material resources is essential to achieve the core objective of improving and maintaining the health of the population, as well as to guarantee the sustainability and quality of a universal healthcare system that is both public and free, such as the Spanish system.
We detected a considerable number of patients included in SWL who renounced surgery before it was programmed, or who failed to attend the appointment for the operation. This causes a substantial disturbance in our working as well as a fruitless consumption of resources. Cancelling the surgical procedures included in SWL involves wasting a large quantity of resources and producing direct and indirect costs. It has a direct negative effect on the quality of care, making medical services less accessible, creating morbidity and dissatisfaction in patients and raising doubts about the objectivity of this parameter as a care quality indicator.7,8
The objectives of this study are to investigate the reasons for this renunciation of forefoot surgery and its possible connections with factors such as the type of pathology, sex, waiting time or the doctor responsible for the indication. An additional aim is to compare these results with those for other common pathologies in orthopaedic surgery and traumatology, such as carpal tunnel syndrome (CTS) and internal meniscus pathology (IMP); all of these are major out-patient surgical procedures.
Material and methodsWe carried out an observational, descriptive and retrospective study of the renunciations of surgery by 2399 patients included in the foot and ankle unit SWL of our hospital for forefoot surgery in the period from 1 January 2014 and 31 March 2018, a total of 51 months.
Our hospital is a third level teaching hospital with a high number of annual out-patient surgical operations. There were an average of 2,434.2 out-patient operations per year from 1999 to 2018, according to data obtained from the admissions department and the clinical documentation of our hospital. There were a total of 48,684 procedures in the past 10 years.
Patients are firstly assessed in the out-patient surgeries of the foot and ankle unit, after referral from primary care, general traumatology services or other units in the department, the emergency department or other specialities. The clinical history is commenced in the said speciality surgeries, a directed physical examination takes place and, if necessary, it is complemented with imaging tests to decide how best to manage the pathology in question.
Patients with an indication for surgery are given an explanation of the characteristics of their pathology and the recommendation for surgery. The expected results are described, together with the risks and complications, and the patient signs the informed consent document. The surgical acceptance document is then filled out, indicating the type of intervention (major out-patient surgery, minor surgery, surgery with admission and diagnostic procedures), the priority of the intervention, the need for pre-anaesthesia evaluation and preoperative tests. This document is completed with the signature and identification of the doctor who indicates surgery. The patient is also given instructions for the day of the operation and immediate postoperative period. The patient is responsible for giving this document to the secretaries who plan preoperative appointments and including them in the SWL. Patients remain in the SWL until the surgical operation or the moment they leave it.
Interventions are generally planned by the head of the unit, following the order and priority of the SWL. In general the duration of the validity of complementary tests and pre-anaesthesia is taken to last for 6 months, according to the stipulations of Order 804/2016, of 30 August, of the Board of Health, which approved the instructions for the registration of patients in Madrid Health Service surgical waiting list (BOCM of 5 September 2016),9 on condition that the clinical conditions of the patient have not varied considerably. Complementary tests and the pre-anaesthesia evaluation would have to be repeated after this period of time so that the patient can be operated.
Once surgery has been programmed the patient has a variable margin of time in which to arrive on the morning or afternoon when the operation is to take place, in a suitable condition of fasting and having suspended any medication and with the requisite of being accompanied by a family member so that they can be discharged on the same day after the surgical operation.
The data gathered from the internal records of the hospital include patient sex, their diagnosis and type of intervention, their preoperative state, time in the SWL, the administrative reason for renunciation and the doctor who indicated surgery. All of the patients who entered the SWL but then for different personal reasons renounced surgery have been considered to be “renunciations of surgery”: voluntary renunciation, patients who could not be located, repeated delays or failure to arrive. Cancellations or suspensions due to logistical or administrative problems in the hospital were not included, together with problems in connection with medical professionals or medical problems of the patient.
The data were analysed using version 16.25 of the Microsoft Excel 2019 spreadsheet (Microsoft Corporation, Washington, U.S.A.). Qualitative descriptive data are shown as absolute numbers and percentages, while quantitative data are shown as an average and standard deviation. The graphs were produced using the same program.
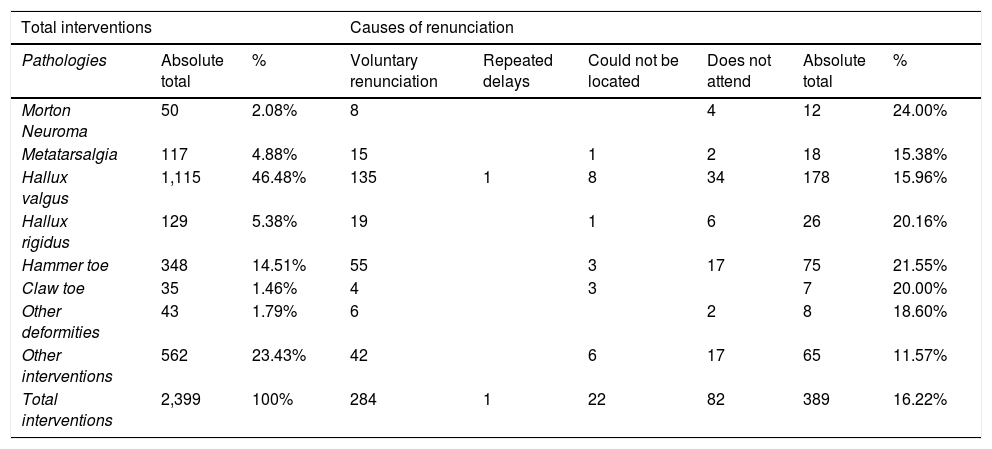
Results389 renunciations were recorded, amounting to 16.22% of the patients included in SWL for forefoot surgery. The pathologies affected the most often by this were: Morton’s neuroma with 24% of renunciations and hallux rigidus with 20.16%. HV was the most frequent pathology and recorded 15.96% of renunciations in this series. Table 1 shows the data on the total number and percentage of operations together with the total number and percentage of renunciations, as well as the causes of renunciation according to type of forefoot pathology.
Absolute number and percentage of interventions according to type of forefoot pathology, reason for renunciation, absolute No. and percentage of renunciations according to type of forefoot pathology.
| Total interventions | Causes of renunciation | |||||||
|---|---|---|---|---|---|---|---|---|
| Pathologies | Absolute total | % | Voluntary renunciation | Repeated delays | Could not be located | Does not attend | Absolute total | % |
| Morton Neuroma | 50 | 2.08% | 8 | 4 | 12 | 24.00% | ||
| Metatarsalgia | 117 | 4.88% | 15 | 1 | 2 | 18 | 15.38% | |
| Hallux valgus | 1,115 | 46.48% | 135 | 1 | 8 | 34 | 178 | 15.96% |
| Hallux rigidus | 129 | 5.38% | 19 | 1 | 6 | 26 | 20.16% | |
| Hammer toe | 348 | 14.51% | 55 | 3 | 17 | 75 | 21.55% | |
| Claw toe | 35 | 1.46% | 4 | 3 | 7 | 20.00% | ||
| Other deformities | 43 | 1.79% | 6 | 2 | 8 | 18.60% | ||
| Other interventions | 562 | 23.43% | 42 | 6 | 17 | 65 | 11.57% | |
| Total interventions | 2,399 | 100% | 284 | 1 | 22 | 82 | 389 | 16.22% |
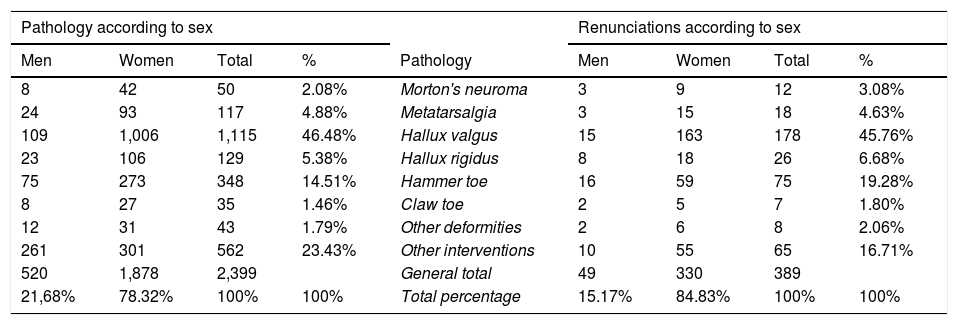
According to sex the renunciation rate was 15.12% of men vs 84.88% women. The corresponding data for HV are 8.43% (15 cases) of renunciations by men and 91.57% (163 cases) women. Table 2 shows the number of cases per sex and forefoot pathology, as well as the number of renunciations according to sex and pathology, and the percentage of these over the total number of renunciations. In the comparative study with other highly prevalent pathologies with out-patient treatment, such as CTS and IMP, the renunciation rate was 17.42 and 8.92% respectively, with a distribution according to sex of 77.4% and 22.6% of renunciations by women and men in cases of CTS and 36.08% and 63.92% of renunciations by women and men in cases of IMP, respectively.
Number of cases according to sex and forefoot pathology, as well as number of renunciations per sex and pathology, and the percentage of the same over the total number of renunciations.
| Pathology according to sex | Renunciations according to sex | |||||||
|---|---|---|---|---|---|---|---|---|
| Men | Women | Total | % | Pathology | Men | Women | Total | % |
| 8 | 42 | 50 | 2.08% | Morton's neuroma | 3 | 9 | 12 | 3.08% |
| 24 | 93 | 117 | 4.88% | Metatarsalgia | 3 | 15 | 18 | 4.63% |
| 109 | 1,006 | 1,115 | 46.48% | Hallux valgus | 15 | 163 | 178 | 45.76% |
| 23 | 106 | 129 | 5.38% | Hallux rigidus | 8 | 18 | 26 | 6.68% |
| 75 | 273 | 348 | 14.51% | Hammer toe | 16 | 59 | 75 | 19.28% |
| 8 | 27 | 35 | 1.46% | Claw toe | 2 | 5 | 7 | 1.80% |
| 12 | 31 | 43 | 1.79% | Other deformities | 2 | 6 | 8 | 2.06% |
| 261 | 301 | 562 | 23.43% | Other interventions | 10 | 55 | 65 | 16.71% |
| 520 | 1,878 | 2,399 | General total | 49 | 330 | 389 | ||
| 21,68% | 78.32% | 100% | 100% | Total percentage | 15.17% | 84.83% | 100% | 100% |
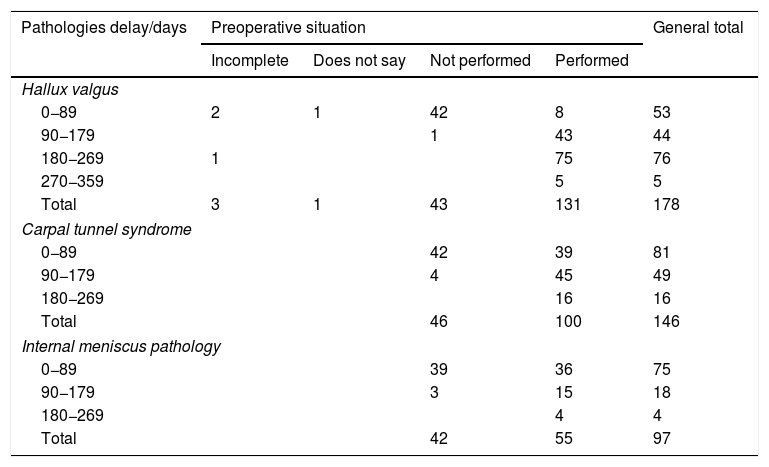
Respecting the preoperative situation, we found that except in the renunciations which occurred closest to the planned date of surgery, in the majority of cases the renunciation occurred after the preoperative preparation (Table 3). The most frequent reason for cancellation due to the patient in cases of HV is voluntary renunciation (75.84%), followed by failure to arrive (19.10%), the impossibility of locating the patient (4.49%) and repeated postponements (0.56%). Table 4 shows the comparison with CTS and IMP, which can be seen to have similar percentages.
Renunciations according to preoperative situation, pathology and waiting time.
| Pathologies delay/days | Preoperative situation | General total | |||
|---|---|---|---|---|---|
| Incomplete | Does not say | Not performed | Performed | ||
| Hallux valgus | |||||
| 0−89 | 2 | 1 | 42 | 8 | 53 |
| 90−179 | 1 | 43 | 44 | ||
| 180−269 | 1 | 75 | 76 | ||
| 270−359 | 5 | 5 | |||
| Total | 3 | 1 | 43 | 131 | 178 |
| Carpal tunnel syndrome | |||||
| 0−89 | 42 | 39 | 81 | ||
| 90−179 | 4 | 45 | 49 | ||
| 180−269 | 16 | 16 | |||
| Total | 46 | 100 | 146 | ||
| Internal meniscus pathology | |||||
| 0−89 | 39 | 36 | 75 | ||
| 90−179 | 3 | 15 | 18 | ||
| 180−269 | 4 | 4 | |||
| Total | 42 | 55 | 97 | ||
Reason for renunciation according to pathology.
| Voluntary renunciation | Repeated delays | Could not be located | Failure to attend | % renunciations | |
|---|---|---|---|---|---|
| Hallux valgus | 75.84% | 0.56% | 4.49% | 19.10% | 15.96% |
| Carpal tunnel syndrome | 71.92% | 3.42% | 24.66% | 17.42%% | |
| Internal meniscus pathology | 67.01% | 2.06% | 30.93% | 8.92% |
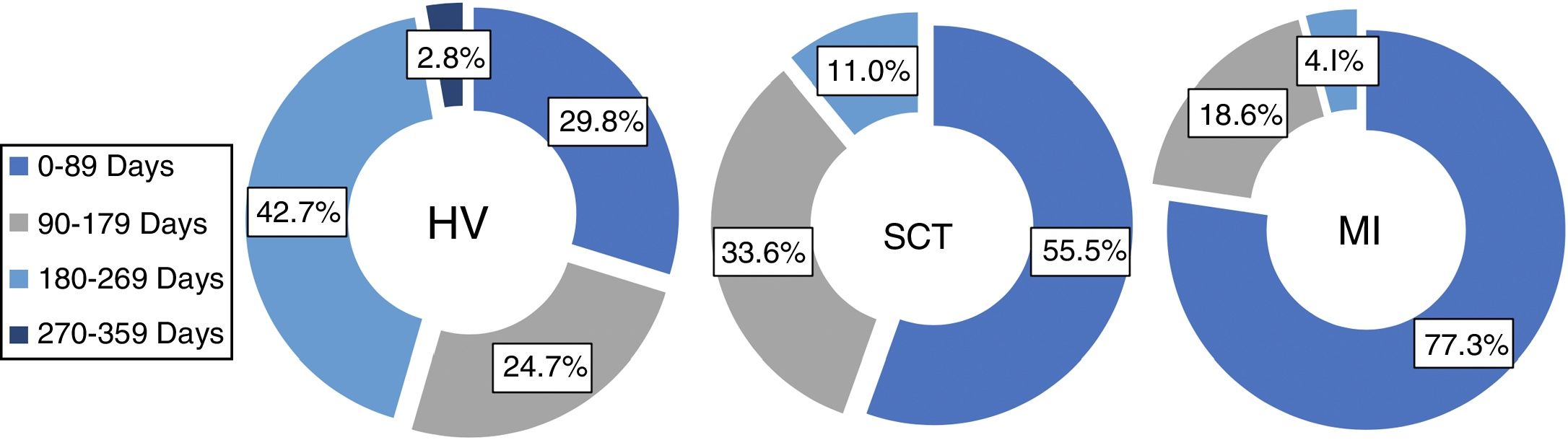
To evaluate the association between the time patients remain in the SWL and the renunciation rate, we set regular three-monthly intervals for each pathology relative to the moment at whicjh patients renounced surgery (Fig. 4). Thus for HV the highest percentage (42.7%) of pacientes who renounced surgery did so in the period from six to nine months, while 24.7% did so from three to six months and 29.8% did so from zero to three months; for CTS and IMP the highest percentage of patients who renounced surgery did so in the period from zero to three months, at 55.5% and 77.3%, respectively.
, carpal tunnel syndrome (CTS) and internal meniscus pathology (IMP) showing the percentage of renunciations of surgery according to time spent in the SWL.")
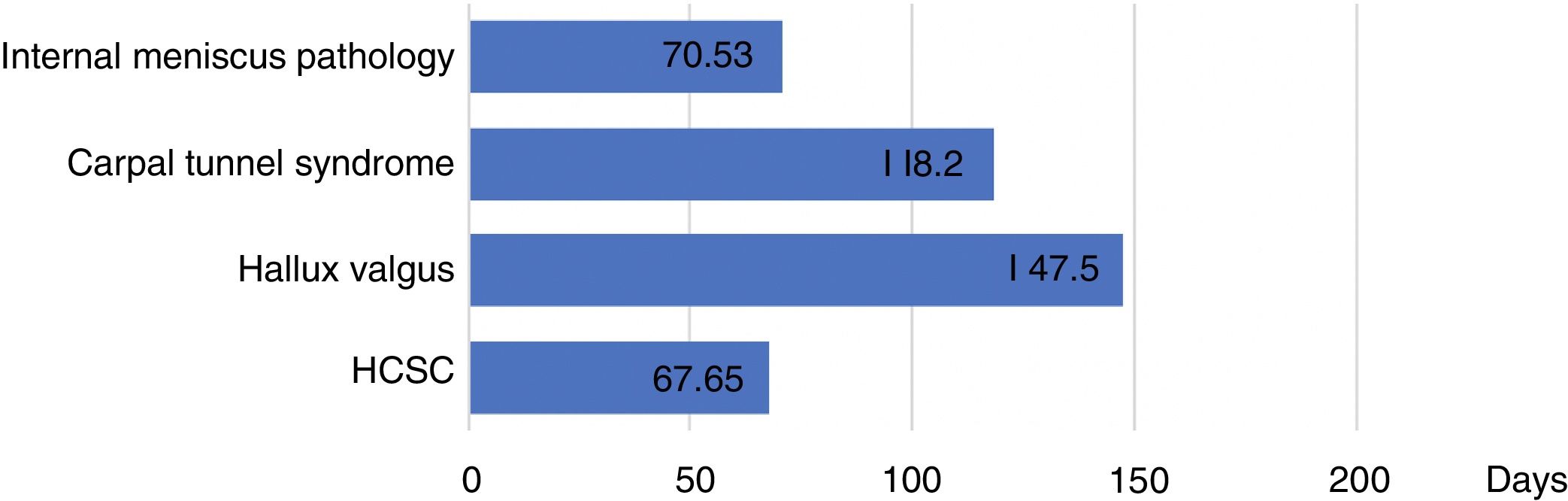
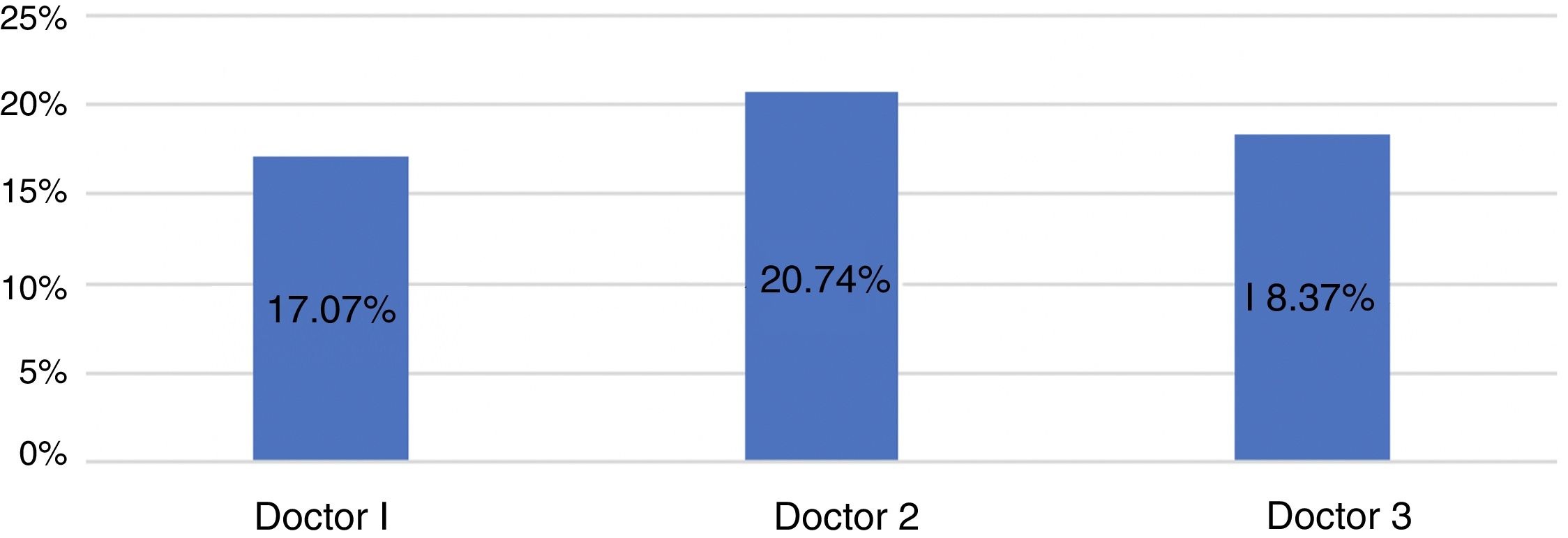
Fig. 5 shows the average number of days during which patients remained in the SWL until they left it. The patients who renounced HV and CTS surgery had spent an average number of days in the SWL before doing so that was quite a lot higher than the hospital average and for meniscus pathology. Regarding renunciations of forefoot surgery according to the indicting doctor, it can be seen in Fig. 6 that the differences here are not statistically significant.


Although cancellations due to the renunciation of surgery by the patient are a challenge for the healthcare system, there is no consensus among professionals regarding acceptable rates of the same.10 Greater knowledge of the causes which lead a patient to renounce surgery may help us to better understand the patients and anticipate future problems that would allow us to detect areas in medical care that could be improved.
Several publications in the literature cover the subject of SWLs and cancellations of surgery as a problem in health systems, leading to an increase in medical costs.11,12 Nevertheless, to date we are unaware of any publication that specifically covers patient renunciations of surgery, and more specifically of foot surgery.
Talking in general, several authors state that cancellations of planned surgical operations may be due to problems associated with medical professionals, logistic or administrative problems in hospitals10,13–15 or ones associated with the patients themselves. The latter may include medical problems, incomplete preoperative preparation or renunciation by the patients due to personal, social or professional reasons.16
We have concentrated on the particular group of cancellations which are due to the patients themselves and their personal, social or professional reasons. We have termed these reasons “renunciation of surgery”, and this excludes cancellations or suspensions due to medical reasons or ones in association with logistical problems in the hospital or ones in connection with medical staff. An initial analysis of the results obtained in our study confirms the first impression that the surgery renunciation rate of patients in the SWL for out-patient forefoot surgery in our area is high, at 16.22% for our field of work.
Due to its high rate of prevalence and direct association with perceived quality of life, the debate on waiting lists as care and management quality indicators could centre on forefoot pathology. This would cover, amongst other factors, the major differences observed between autonomous communities within the same public healthcare system.2 As a whole, the renunciations of surgery by patients in SWL give rise to problems in how they are managed and function. Given the combined importance of the specific weight of these pathologies and the full impact that surgical renunciations have on the health system, the work of examining our data is worthwhile.
Firstly, the frequency with which forefoot surgery is renounced according to each pathology will offer us an indication of its possible causes. Morton’s neuroma, for which almost a quarter of the patients in the SWL renounce surgery, is followed very closely for this by hallux rigidus: these pathologies essentially cause mechanical pain that is often remittent and recurring, with periods of time when symptoms reduce or even disappear, and they hardly affect the external morphology of the foot. This may partially explain why their rates of renunciation are higher than those corresponding to HV, which is the most frequent and limiting in terms of pain and footwear, with the highest number of patients in SWLs. The fact that some pathologies are more common in women partially justifies the overall difference between the sexes here, which is not so marked after correction in percentage terms.
Comparison with other very common orthopaedic pathologies treated on an out-patient basis obtains data that seems to share some of the above-mentioned reasons: in the case of compressive nerve neuropathy at carpal tunnel level the rate of renunciation is relatively high. This may be associated with its inflammatory nature together with occasional hormonal influence on the establishment and maintenance of symptoms. This would explain why it is more frequent in women as well as its eventual spontaneous improvement following modification of activity or the use of orthopaedic devices such as nocturnal splints.17 In the case of internal meniscus pathology treated by arthroscopic meniscal regularisation, this has a less asymmetrical distribution between the sexes, and the symptoms of pain, instability, blockage or repeated discharges usually cause more functional deterioration and restriction of everyday activities, and this may explain its lower rates of renunciation.18
Regarding the timing of renunciation, analysis of this according to period found that, apart from the group of patients who leave the SWL before the preoperative period, the largest number of renunciations in forefoot pathologies occurred in the group that waited for six to nine months, followed by those who waited from three to six months. This supports the hypothesis that there is an association between longer waiting times for forefoot surgery and the risk of abandoning the SWL. Some authors indicate that a long waiting time in the SWL seems to affect the health of patients as well as the results and degree of satisfaction with interventions,19–21 although the recent systematic review by Morris in 2018 showed no clear evidence for the impact of time spent in a SWL on health.22 Likewise, when we analyse the other two comparative pathologies these periods can also be seen to be influenced by the natural history of the diseases studied and the results of orthopaedic treatments: the complete improvement in CTS with the use of a splint in terms of loss of strength and nocturnal pain usually takes longer to achieve, while the influence of rehabilitation on IMP is faster and more sustained than is the case for orthoprosthetic measures applied to the forefoot, so more patients leave the SWL during the first three months in the case of this pathology.
It may be also deduced from the above considerations that a certain percentage of patients may renounce surgery because their symptoms have improved or even been “cured”, making it unnecessary. This may lead us to think, as other works hypothesise, that more information, attention and patience when indicating surgery may reduce the number of circumstances under which it ceases to be necessary.23–25
The different reasons for renunciation in the different pathologies that were compared are distributed in a very similar way. The patients who could not be located form the smallest group, and in all cases a majority of patients voluntarily communicate their renunciation of surgery. The highest proportion of those who so had HV, followed by CTS and then IMP; the percentage of patients who neither arrive nor communicate is in the inverse order. A probable reason for this may be age distribution: patients with HV have a higher average age, and associated cultural and educational factors may lead them to be more likely to inform the health administration of changes in their situation in the SWL. Patients with the other pathologies and IMP above all tend to be younger and in work, with more changeable professional and family circumstances. They are more likely to come up against unforeseen circumstances and are therefore at greater risk of not arriving for the operation or even forgetting to inform the administration that they will not do so.
As well as pointing out which factors influence the cancellation of planned surgery, the works in the literature suggest that many cancellations are avoidable,26,27 and they propose ways of reducing them. Improving preoperative instructions and information about operations using a multidisciplinary approach28,29 may help to improve cancellation rates and involve patients more in the procedure they are to undergo.30–33 It would seem in fact that patients would even like to know where they stand in the SWL,34 so that they can organise themselves socially, in their family and in their work as they approach the date of their operation, and it is probable that this would help to reduce cancellations. Moreover, communicating the estimated date for surgery26 sufficiently early and sending out a reminder have been shown to reduce the number of last-minute cancellations and the number of patients who fail to arrive for an operation.28,35 Other authors propose informing patients and making them aware of the importance of promising to arrive for an operation once they have been included in a SWL, as well as doing the preparative tests and other steps, while also informing them of the costs which arise if they do renounce their surgery.8,36 Other recommendations which we consider to be useful consist of offering patients an accessible means of cancelling operations, as well as verifying their personal data, contact details and address. Furthermore, according to some studies, allowing patients to take part in planning the date of their operation has been associated with better results, as it allows them to adapt surgery to their individual circumstances.37
The limitations of our study include, among others, the fact that as it is a highly specific work that centres on a specific pathology the results cannot be extrapolated. Nevertheless, we found that it was possible to draw reasonable conclusions when we compared it with other orthopaedic pathologies with similar rates of prevalence. In this point the importance of individualising results can be underlined, analysing not only numerical values in isolation but also within the complex understanding of each pathology. Another limitation of our study is that we were unable to more precisely know the specific reasons why each patient renounced surgery, as this would have allowed us to extract firmer conclusions.
We therefore see that renouncing a surgical forefoot operation often occurs, and it may be based on multiple causes. However, the data obtained show tendencies that can explain these causes: the lack of a relationship with the doctor who indicates surgery or the possible influence of the time patients spend in the SWL. Nevertheless, above all it depends on the intrinsic characteristics of each pathology and their natural history during the waiting time and its response to conservative treatments. Thus those pathologies which respond more or faster to orthoprosthetic or rehabilitation therapies lead patients to renounce treatment earlier than those which do not respond so well or which cause an evident morphological alteration. It also depends on the repercussions of the pathology on everyday life activities, as is made plain by the low rate of surgical renunciation in IMP patients.
ConclusionsPlanned forefoot surgery is often renounced in our field, amounting to 16.22% of the patients included in SWL in our series. The forefoot pathologies subject to the highest rates of renunciation are metatarsalgia, Morton’s neuroma and hallux rigidus. Somewhat lower figures were recorded for one of the pathologies that is treated surgically the most often, HV. This may be because it causes more pain and difficulties with footwear than the other conditions.
The number of renunciations of surgery in HV is comparable to those observed in CTS surgery, while the percentage found for IMP amounts to half those of the other two conditions, which is probably due to its greater affect on everyday life activities. According to sex, renunciation of HV and CTS surgery is more common in women, while this is so for IMP in men, which agrees with the distribution and prevalence of each pathology.
Although no clear evidence emerges when studying the three pathologies that were compared, in HV it is feasible that there is a relationship between the time spent in a SWL and the percentage of renunciations. However, for CTS and IMP this datum may be affected more by the nature, evolution and response to conservative treatment of the pathology itself. We found no statistically significant differences between percentages of renunciations and the doctor who indicated surgery.
To improve the management of our waiting lists and to reduce the number of renunciations, we have to improve communication with the patients on their pathology and the surgery they will receive. The patients have to be more involved in the process, making them aware of the importance of visiting at the time of their appointment, creating systems to facilitate the notification of cancellation and informing them of the date of surgery sufficiently beforehand, as well as creating reminders. We should also explain the natural history of their pathologies to patients and the options of altering some of them using non-surgical techniques that are able to delay or even replace surgery. We believe that these improvements, together with an understanding the nature of each pathology, would help to reduce the number of renunciations and contribute to optimising our SWL and therefore surgical treatment too and the quality of care.
FinancingThis research received no specific supports from public, commercial or not-for-profit bodies.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Llanos S, Galán-Olleros M, Manrique E, Celada R, Galeote JE, Marco F. Renuncias en cirugía del antepié. Análisis crítico de las listas de espera. Rev Esp Cir Ortop Traumatol. 2021;65:75–84.
