







Investigation of deaths caused by the use of firearms, with their different homicidal, suicidal and accidental etiologies, is part of the medical-forensic expert's regular work. Mouth is usually chosen by the suicide using a gun. However, gunshot rarely occurs – or it is an exception, in homicidal or accidental deaths. In this paper we shall review the different variables which are useful in order to discriminate the different etiologies, such as the scene, the kind of weapon used, the number of injuries sustained and their location, or the direction of the bullet. Also, we shall particularly focus on the types of injuries caused. The way that lips, teeth and tongue are affected is of particular interest in this investigation. For this purpose, we have conducted a research in books and medical articles, including the PubMed, Dialnet and Academic Google bibliographic database.
El estudio de las muertes por arma de fuego, en sus distintas etiologías, forma parte de la práctica habitual medicoforense. En aquellas de origen suicida, la boca constituye un lugar preferente para el disparo, de forma contraria a los supuestos homicidas o accidentales. En el presente trabajo se revisan distintas variables de utilidad para la determinación medicoforense de la etiología, con especial referencia a los disparos intraorales. Entre ellas se analizan el lugar del suceso, tipo de arma empleada, el número y localización de las heridas, el trayecto seguido por el proyectil y las lesiones ocasionadas, siendo de especial interés la forma en que resultan afectados los labios, los dientes y la lengua. Para lo cual se ha realizado una búsqueda sistemática, incluyendo las bases de datos bibliográficas PubMed, Dialnet y Google Académico.
Firearm-related deaths constitute a major chapter in forensic medicine. The use of firearms in the settings of homicides, suicides and accidents affords them a special juridical and medical/legal significance. The habitual subjects of forensic examinations include measurements of the distance and direction of shots, wound characteristics or the possible survival of the victims, and as a preliminary and fundamental issue, differentiation between the causes of death by suicide and homicide, which will determine how the investigation develops.
The incidence of deaths of this type is indicative of its significance, although there are marked differences based on several factors, among which the ease of access to this type of weapon stands out, with the result of its prohibition a subject of study.1
The figures are very different and show the frequent use of firearms in countries where their availability is greater, such as Switzerland2 or the United States3; in the US they are involved in 68% of homicides and 51% of suicides. Similarly, in Argentina, they are involved in 28.2% of suicides and up to 70% of homicides.4
These figures differ considerable from those obtained in Asian countries. In Japan, where hanging is the preferred method of suicide, the use of firearms is found only in 0.2% of cases, in line with the fact that the population of Asians residing in the United States has the lowest rate of suicide by this method.5 Similarly, in Shanghai, China, the use of a firearm is recorded only in 0.5% of homicides and 0.7% of suicides, with hanging and deliberate jumping from heights being the main methods.6
With regard to Spain, in the Forensic Pathology Institute of Madrid, which performs the majority of autopsies in the autonomous community, firearms appear to be involved in 5% of suicides, where there is a preference for jumping, and 19% of homicides, where knives are predominately used.7 Likewise, a study on suicide in Seville found that firearms only in 7.5% of these deaths, a significantly lower percentage than those for hanging and jumping.8
Although the examination of the corpse and the site of the incident generally provide sufficient evidence to differentiate between suicide and homicide, there are cases where doubt remains, particularly those involving bodies in poor condition or after an insufficient examination during the autopsy, and which may, on occasion, be unsolvable. In these cases, in addition to basic studies—such as gunpowder residue and blood spatter analysis, the study of ridge patterns in prints on the firearm or the search for other signs of violence at the scene and on the body—of particular interest will be the number and location of wounds, the type of firearm used, the site of the event, the distance and the trajectory of the bullet, and the type of injury. This review analyses these latter factors. Although shootings are addressed according to their different causes, this review focuses on firearm-related mouth injuries, with the limitations entailed by frequency of homicides in these cases being low.
Discriminant function analysis of homicides and suicidesSex and ageAs is the case with violent deaths in general, the proportion of men who die from gunshot wounds is clearly higher than that of women, being even more pronounced in cases of suicide. For example, Verzeletti et al.9 reported a significant predominance of men (92.9%) among the suicides that comprise their study, a figure that drops to 72.9% when referring to homicide victims; Druid10 notes a figure of 98.59% of men in suicides and 59.2% in homicides; and Karger et al.11 reported figures of 89.4% and 73.3%, respectively.
If we refer specifically to the preference of each sex for this method of suicide, the results are striking12: in Argentina, the method was chosen by 37.6% of men, whereas for women the rate was 25.9%; in the US, the figures were 47.8% and 35.7%, respectively. In a similar way, in Venezuela, these figures were 23.3% and 12.2%; in Israel, 25.4% and 9.1%; in Japan, 0.2% and in no case among women; in France, 22.1% and 4.1%; in Germany, 10.3% and 1.4%; in Poland, 1.1% and 0.2%; in Sweden, 17.1% and 0.9%; in the United Kingdom, 3.5% and 0.6%; and in Spain, these figures amounted to 7.1% of men and 0.9% of women.
In relation to the mouth being the site of the gunshot, gender-based differences have also been noted. Among the suicides by shotgun registered in Istanbul, Asirdizer et al.13 found that men selected the mouth in 10.9% of the cases, with no case recorded in women, who opted for less visible areas such as the abdomen or, when it was to the head, the right temporal region. In contrast, in the extensive series of 1200 firearm-related suicides analysed by Stone,14 5.11% of the women chose the mouth, while men did so in 4.87% of the cases.
The different series consulted are consistent in terms of the higher age of those committing suicide compared with homicide victims, showing the following figures (mean age at suicide/homicide): 47/38, 49/30, 36/23, 39/34 and 51/34 years of age.9,15–18
Site of the incidentsSuicides are often committed, as might be expected by the voluntary and personal nature of the act, at home, considering as such the interior and surrounding property of the same. This is predominately true in the series of Karlsson,18 of Fedakar et al.,19 and of Thomsen et al.,20 (60.6%, 60.5% and in 72% of cases, respectively).
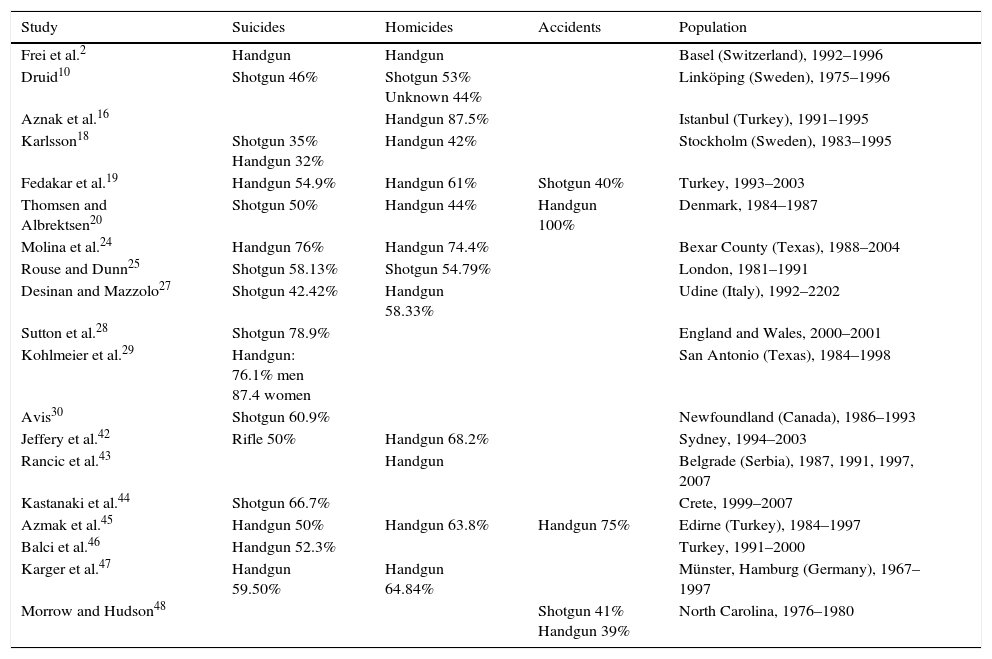
Type of firearmIf in firearm-related suicides there is a relative predominance of the use of long guns (shotguns) versus handguns (pistols or revolvers), the use of the latter stands out clearly in homicides (Table 1). In accidents, however, the data are limited. In an analysis of the latter by Thomsen,20 in the four cases referred to, a short gun was used, and all in the context of Russian roulette; although the ultimate motive (i.e., whether accidental or suicidal) of these cases is a source of debate.21,22
Gun preferentially used in the different aetiologies of firearm-related death.
| Study | Suicides | Homicides | Accidents | Population |
|---|---|---|---|---|
| Frei et al.2 | Handgun | Handgun | Basel (Switzerland), 1992–1996 | |
| Druid10 | Shotgun 46% | Shotgun 53% Unknown 44% | Linköping (Sweden), 1975–1996 | |
| Aznak et al.16 | Handgun 87.5% | Istanbul (Turkey), 1991–1995 | ||
| Karlsson18 | Shotgun 35% Handgun 32% | Handgun 42% | Stockholm (Sweden), 1983–1995 | |
| Fedakar et al.19 | Handgun 54.9% | Handgun 61% | Shotgun 40% | Turkey, 1993–2003 |
| Thomsen and Albrektsen20 | Shotgun 50% | Handgun 44% | Handgun 100% | Denmark, 1984–1987 |
| Molina et al.24 | Handgun 76% | Handgun 74.4% | Bexar County (Texas), 1988–2004 | |
| Rouse and Dunn25 | Shotgun 58.13% | Shotgun 54.79% | London, 1981–1991 | |
| Desinan and Mazzolo27 | Shotgun 42.42% | Handgun 58.33% | Udine (Italy), 1992–2202 | |
| Sutton et al.28 | Shotgun 78.9% | England and Wales, 2000–2001 | ||
| Kohlmeier et al.29 | Handgun: 76.1% men 87.4 women | San Antonio (Texas), 1984–1998 | ||
| Avis30 | Shotgun 60.9% | Newfoundland (Canada), 1986–1993 | ||
| Jeffery et al.42 | Rifle 50% | Handgun 68.2% | Sydney, 1994–2003 | |
| Rancic et al.43 | Handgun | Belgrade (Serbia), 1987, 1991, 1997, 2007 | ||
| Kastanaki et al.44 | Shotgun 66.7% | Crete, 1999–2007 | ||
| Azmak et al.45 | Handgun 50% | Handgun 63.8% | Handgun 75% | Edirne (Turkey), 1984–1997 |
| Balci et al.46 | Handgun 52.3% | Turkey, 1991–2000 | ||
| Karger et al.47 | Handgun 59.50% | Handgun 64.84% | Münster, Hamburg (Germany), 1967–1997 | |
| Morrow and Hudson48 | Shotgun 41% Handgun 39% | North Carolina, 1976–1980 |
In India, as in other developing countries, there is a prevalence of the use of illegally manufactured firearms (Kumar et al.23).
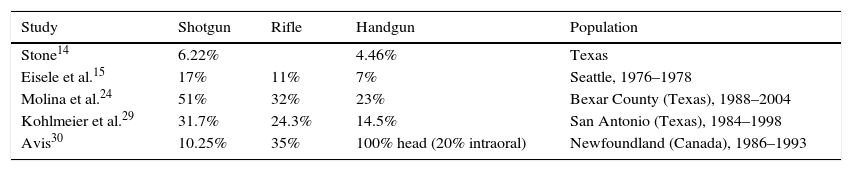
The ways in which the type of firearm used may influence the choice of mouth for suicide have been highlighted by several authors (Table 2), with the use of shotguns being more frequent. With regard to homicides, in the study by Molina et al.,24 2% of gunshot wounds to the head were intraoral when the firearm used was a pistol, and 5% when it was a shotgun, with no case recorded with the use of rifle.
Intraoral option by type of gun.
| Study | Shotgun | Rifle | Handgun | Population |
|---|---|---|---|---|
| Stone14 | 6.22% | 4.46% | Texas | |
| Eisele et al.15 | 17% | 11% | 7% | Seattle, 1976–1978 |
| Molina et al.24 | 51% | 32% | 23% | Bexar County (Texas), 1988–2004 |
| Kohlmeier et al.29 | 31.7% | 24.3% | 14.5% | San Antonio (Texas), 1984–1998 |
| Avis30 | 10.25% | 35% | 100% head (20% intraoral) | Newfoundland (Canada), 1986–1993 |
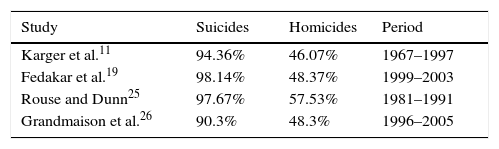
In suicides, the number of shots fired is almost always one, with more cases of intraoral wounds due to their immediate and devastating effects.
This has been shown in different series on suicides,11,19,25,26 with a single shot in more than 90% of cases in all of them, which only happens between 48% and 58% of the time in homicides. While studying 120 deaths by this method, Cina17 found no multiple gunshot wounds in suicides or accidental deaths, compared with 33% among those in homicides.
In the following table (Table 3), the single-shot frequency is recorded in the context of a medical/legal etiology.
Entry woundsThe mouth is known to be one of the main sites of suicide-related gunshot wounds, generally the head11,17,20,24–32 and more specifically the forehead, mouth, submental triangle and fundamentally the right temple. Conversely, in deaths by homicide, the wounds are often multiple,33,34 with atypicality in the areas concerned indicated as being characteristic.33
In an analysis of firearm-related deaths in Bangkok, Suwanjutha32 points out that, although suicide-related gunshot wounds are located inside the mouth, in homicides they are found on the lips.
In general, in suicides the gun is placed in the mouth (intraoral gunshot) intentionally, to ensure a fatal outcome. In homicides, the shooting usually occurs at a distance greater than the point of contact35 (perioral gunshot) due to the victim's evasive reaction, unless the victim is asleep or unconscious (possible intraoral). The case mentioned by Polson et al.,33 in which a girl asked her friend to close her eyes and open her mouth, is illustrative here as a moment where a sure shot was taken. In addition, it must be considered that a mouth injury may merely be a further incidental one, as a result of multiple shots.
Accidental intraoral shots would be found almost exclusively in known cases of Russian roulette, referred to above.
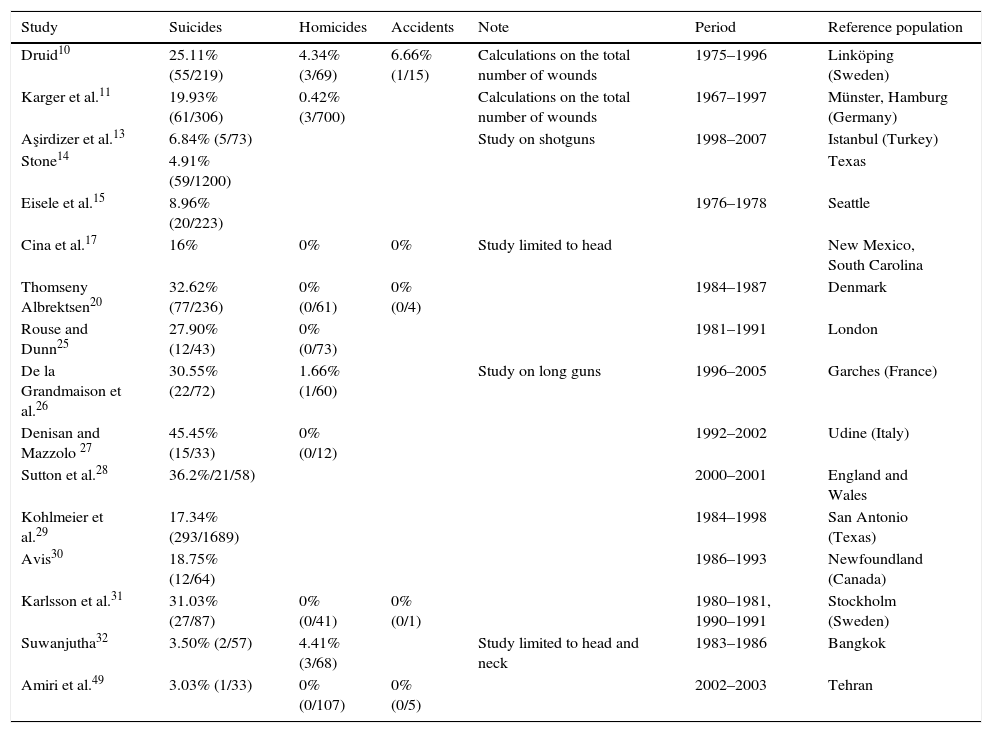
Many studies record gunshots to the mouth depending on the different medical/legal aetiologies (Table 4), although it should be noted that their results are not homogeneous, as some are limited to one type of firearm or a specific anatomical location (head, neck), and the estimates are made on the total number of wounds, often multiple in cases of homicide. All of this must be evaluated when comparing the results.
Intraoral shooting by etiology (percentage and number of cases compared with the total).
| Study | Suicides | Homicides | Accidents | Note | Period | Reference population |
|---|---|---|---|---|---|---|
| Druid10 | 25.11% (55/219) | 4.34% (3/69) | 6.66% (1/15) | Calculations on the total number of wounds | 1975–1996 | Linköping (Sweden) |
| Karger et al.11 | 19.93% (61/306) | 0.42% (3/700) | Calculations on the total number of wounds | 1967–1997 | Münster, Hamburg (Germany) | |
| Aşirdizer et al.13 | 6.84% (5/73) | Study on shotguns | 1998–2007 | Istanbul (Turkey) | ||
| Stone14 | 4.91% (59/1200) | Texas | ||||
| Eisele et al.15 | 8.96% (20/223) | 1976–1978 | Seattle | |||
| Cina et al.17 | 16% | 0% | 0% | Study limited to head | New Mexico, South Carolina | |
| Thomseny Albrektsen20 | 32.62% (77/236) | 0% (0/61) | 0% (0/4) | 1984–1987 | Denmark | |
| Rouse and Dunn25 | 27.90% (12/43) | 0% (0/73) | 1981–1991 | London | ||
| De la Grandmaison et al.26 | 30.55% (22/72) | 1.66% (1/60) | Study on long guns | 1996–2005 | Garches (France) | |
| Denisan and Mazzolo 27 | 45.45% (15/33) | 0% (0/12) | 1992–2002 | Udine (Italy) | ||
| Sutton et al.28 | 36.2%/21/58) | 2000–2001 | England and Wales | |||
| Kohlmeier et al.29 | 17.34% (293/1689) | 1984–1998 | San Antonio (Texas) | |||
| Avis30 | 18.75% (12/64) | 1986–1993 | Newfoundland (Canada) | |||
| Karlsson et al.31 | 31.03% (27/87) | 0% (0/41) | 0% (0/1) | 1980–1981, 1990–1991 | Stockholm (Sweden) | |
| Suwanjutha32 | 3.50% (2/57) | 4.41% (3/68) | Study limited to head and neck | 1983–1986 | Bangkok | |
| Amiri et al.49 | 3.03% (1/33) | 0% (0/107) | 0% (0/5) | 2002–2003 | Tehran |
In an autopsy, the importance of determining a bullet's trajectory in the mouth has been emphasised. Classic in this regard are the papers by Fatteh34,36 describing how in suicides the firearm is pointed upward towards the hard palate or pharynx, unlike in homicides, where the trajectory is horizontal.
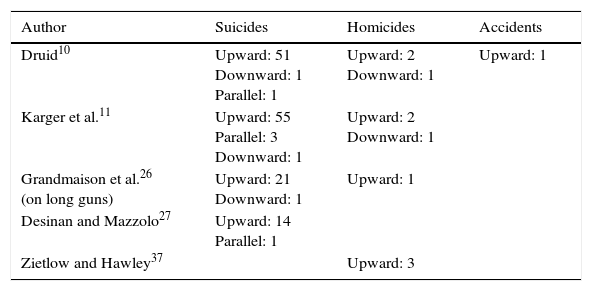
In several studies, the statistics consulted match this upward, anteroposterior trajectory in suicides, such as the study by Denisan and Mazzolo,27 where 14 of 15 intraoral gunshot wounds were consistent with this, as well as in 21 of the 22 of those recorded by Grandmaison et al.,26 55 of 59 of those recorded by Karger et al.,11 and 51 of 53 of those recorded by Druid.10
With regard to homicides, the most common references available are those with an upward intraoral direction, although the cases reported are few and thus lack significance. In the study by Grandmaison et al.,26 the only homicide recorded with a mouth gunshot wound showed an upward trajectory, as was the case in 2 of the 3 homicides described by Karger et al.11 or by Druid,10 or in the 3 cases analysed by Zietlow and Hawley.37 It must be taken into account that this trajectory is unique to intraoral gunshot wounds, unlike perioral ones, which are executed from a greater distance.
The table shows the direction of the bullet in relation to the different aetiologies (Table 5).
Bullet trajectory in the different aetiologies.
| Author | Suicides | Homicides | Accidents |
|---|---|---|---|
| Druid10 | Upward: 51 Downward: 1 Parallel: 1 | Upward: 2 Downward: 1 | Upward: 1 |
| Karger et al.11 | Upward: 55 Parallel: 3 Downward: 1 | Upward: 2 Downward: 1 | |
| Grandmaison et al.26 (on long guns) | Upward: 21 Downward: 1 | Upward: 1 | |
| Desinan and Mazzolo27 | Upward: 14 Parallel: 1 | ||
| Zietlow and Hawley37 | Upward: 3 |
An important aspect of an autopsy is to differentiate between the injuries caused directly by the bullet in its trajectory and those attributable to combustible gases or even the sudden movement of the barrel in the mouth, in the case of lip contusions due to the sight of the firearm in its recoil.33
The study of wounds requires a careful examination of the oral cavity, which is sometimes technically complicated by rigour mortis and an obscure view of the area caused by the injuries themselves and even the lack of a suitable lighting system in the autopsy room. To make a careful examination, access to the mouth has been advocated through the neck33; the use of complementary techniques is also recommended, such as CT38 for charred corpses, or a normal X-ray34,39 with an added indication when the ammunition used was slugs or buckshot.
Other authors, in order to circumvent rigour mortis in the area, have proposed gaining access to the mouth through bilateral incisions made in the retromandibular region.40
In intraoral suicides, the victim lowers the tongue to be able to fit the barrel deep into the mouth, owing to which the bullet does not pass through it, although it may be affected by the effect of the gases or the flame, with tears and burns, as well as bruises on the lips, being common.
Conversely, in homicides the victim will instinctively put the tongue up, and so the bullet pierces it, in addition to damaging the lips and teeth when the shot comes from outside the mouth, which does not occur in suicides. This is evidenced in a homicide noted by Fatteh36 in which the bullet clearly pierced the tongue; or in 6 of the 8 cases described by Azmak et al.,16 where the bullet penetrated a higher plane in the other 2 cases.
There is therefore a need to closely examine the lips, teeth and tongue in deaths of this type.
In addition, mouth injuries are generally highly destructive, in relation to the type of firearm and ammunition used. In intraoral gunshot wounds, which make up the majority of cases, the bullet's direct impact combines with the effects of cavitation and combustible gases that act on a closed cavity, with severe effects on the base of the skull and other craniofacial structures such as the jaw being habitual. In relation to the exit wound, occipital or parietal fractures are common, depending on the bullet's trajectory, usually anteroposterior, following the midline, or with a slight leftward deviation in right-handed subjects. The hard palate may show the wound confirming the bullet's trajectory.
If the shot was horizontal or with a downward trajectory, the cervical vertebrae may be injured directly, without affecting the palate. In this regard, Fatteh36 points out that death in suicides is due to direct brain damage, whereas in homicides, with the bullet's cervical exit, death can be related to blood invading the respiratory tract.
Sometimes the bullet does not exit the head (absence of exit wound), while losing part of its energy after passing through the bony structures,33 but always in relation to the type of firearm and ammunition used. In practice, it is common to observe, in suicide-related gunshot wounds with buckshot, severe destruction in the anterior cranial-facial plane, with no exit hole.
On other occasions during the autopsy, the bullet is located under the scalp, which it was not able to pass through, even with numerous fractures in the cranial vault. This has been reported precisely as a difference between the use of 12- or 20-gauge ammunition, which with the former the bullet perforates the scalp; this is assumed to occur in less than 10% of cases with the use of the lower gauge.41
Case reportsBelow, 6 cases are presented, selected from medical/forensic archives, corresponding to different aetiologies and types of firearm, which illustrate some of the characteristics mentioned.
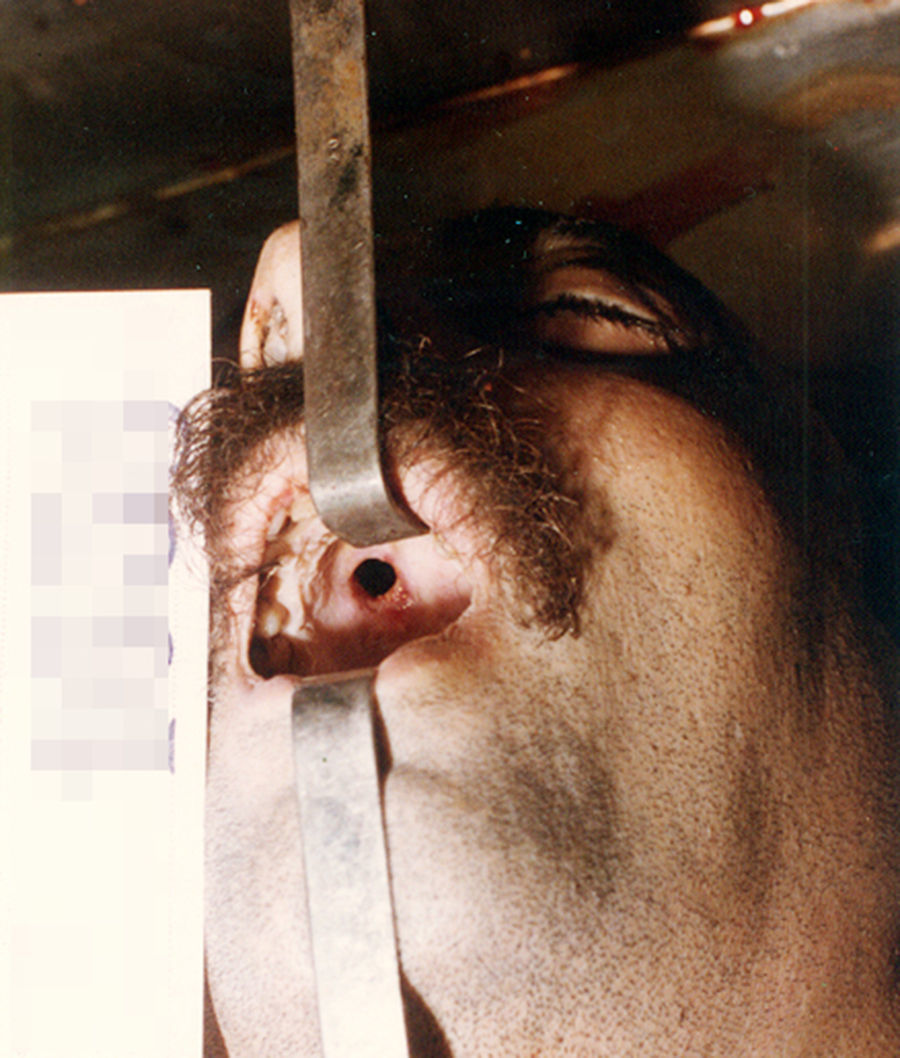
Case 1Distance: intraoral. Direction: markedly caudocranial and slightly anteroposterior. Exit: anterior interparietal. Etiology: suicide. Type of firearm: presumably handgun (not listed).
30-Year-old man, transferred to a hospital, dying of complications due to infection. There was a pronounced upward and slightly posterior trajectory, following the midline with a slight deviation to the right. There was a clear wound in the palate (Fig. 1), crossing the right anterior cerebral fossa.
Case 2.")
Distance: intraoral. Direction: caudocranial and anteroposterior, with slight deviation to the left. Exit: posterior interparietal, slightly to the left. Etiology: suicide. Type of firearm: 38-calibre handgun.
68-Year-old man with serious money problems shot himself on a public road. The gun remained alongside the body. The autopsy showed a single shot, with lip wounds and burns on the tongue and palate. The bullet passed through the latter in its posterior half and the sella turcica at its midline.
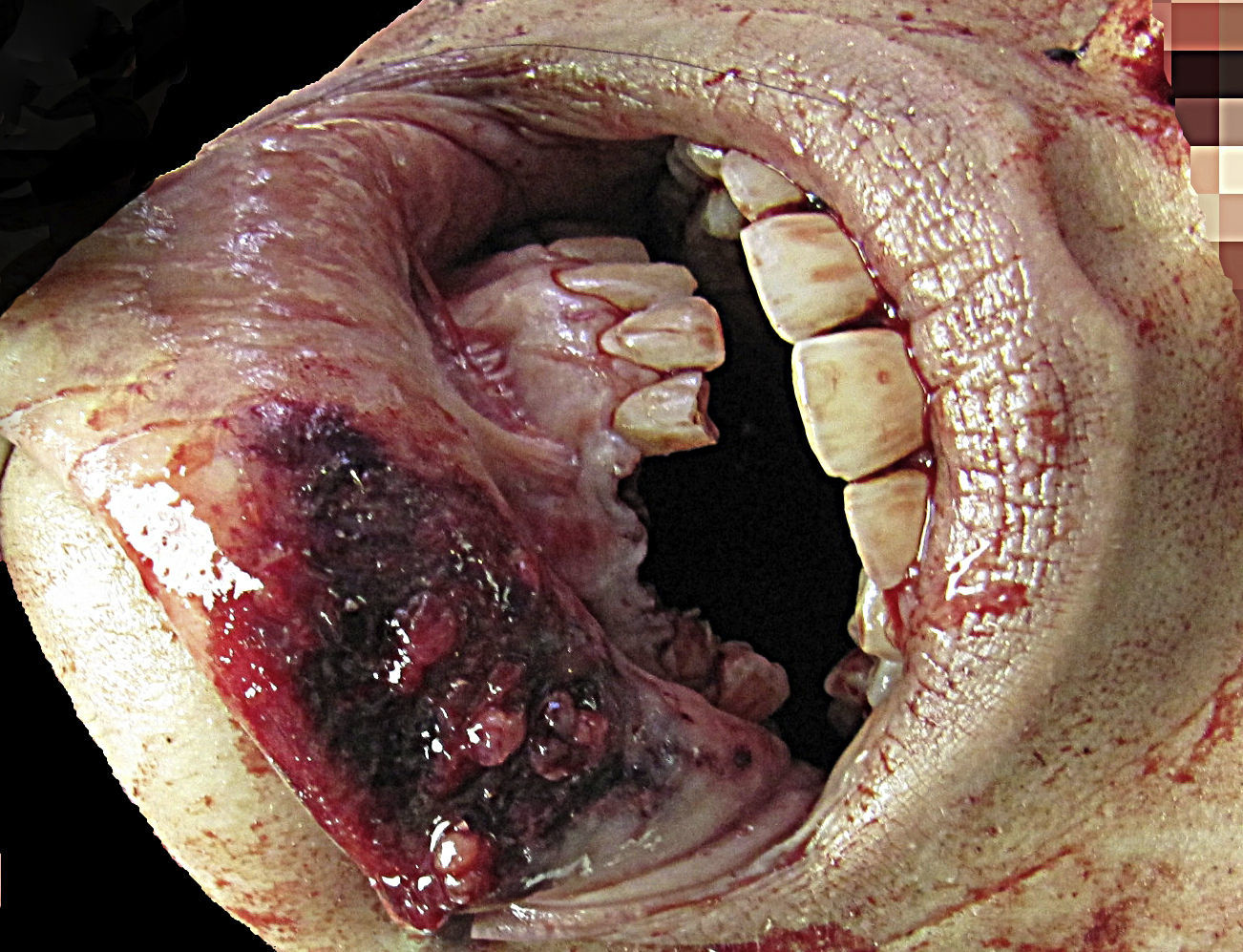
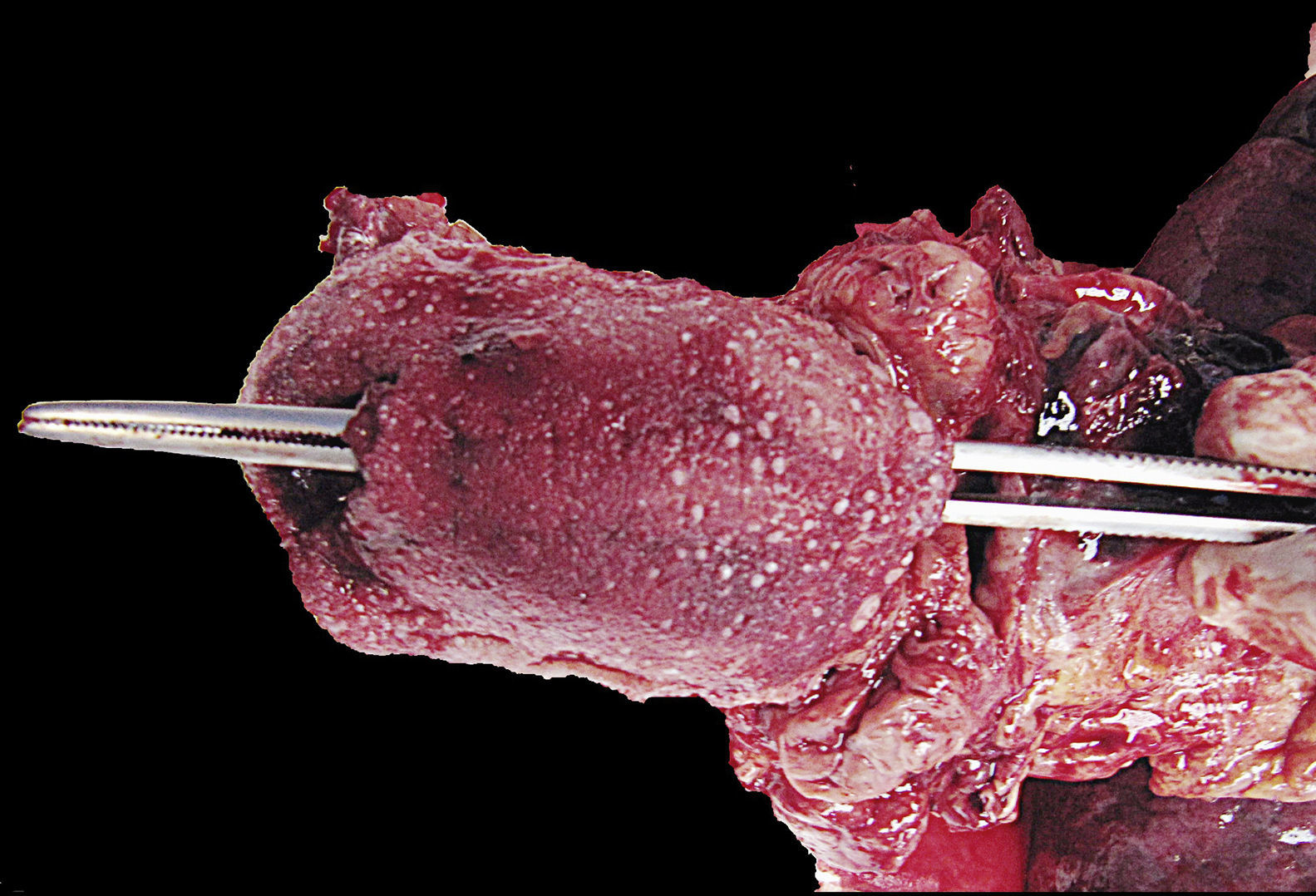
Case 3Distance: short distance (perioral). Direction: anteroposterior, slightly caudocranial and to the right. Exit: right posterior cervical. Etiology: homicide. Type of firearm: handgun.
25-Year-old woman. No information about the site of the incident. Single shot in the mouth with large wound on the lower lip, avulsion of lower teeth and tongue traversed longitudinally by the bullet (Figs. 2 and 3). Fracture of transverse processes of vertebrae C3 and C4 with exit wound 14×12mm in size split in two by a small cutaneous effraction (Fig. 4). Death due to vertebral artery injury with bronchoaspiration and spinal cord injury.
Case 4.")

.")
Distance: intraoral. Direction: anteroposterior, following the midline in a horizontal trajectory. Exit: cervical. Etiology: suicide. Type of firearm: handgun (9mm).
52-Year-old man on antidepressants. Suicide at the workplace. The body remained in a seated position, leaning forward, with the firearm on the floor. Anterior extrusion of the upper incisors. The bullet passed under the posterior edge of the foramen magnum, fracturing the posterior arch of the atlas (Fig. 5).
Case 5.")
Distance: intraoral. Direction: markedly caudocranial and slightly anteroposterior. Exit: no exit wound. Etiology: suicide. Type of firearm: shotgun (buckshot).
Man with no relevant history, with single shot in a fenced enclosure (plot). The shotgun was placed between the legs, with the barrel gripped in one hand. The examination showed an intraoral gunshot wound, with panfacial fracture, damage to the anterior and middle cranial fossa, destruction of the palate and an irregularly sectioned tongue. In the endocranium, there were marks caused by the impact of the buckshot (Fig. 6).
Case 6.")
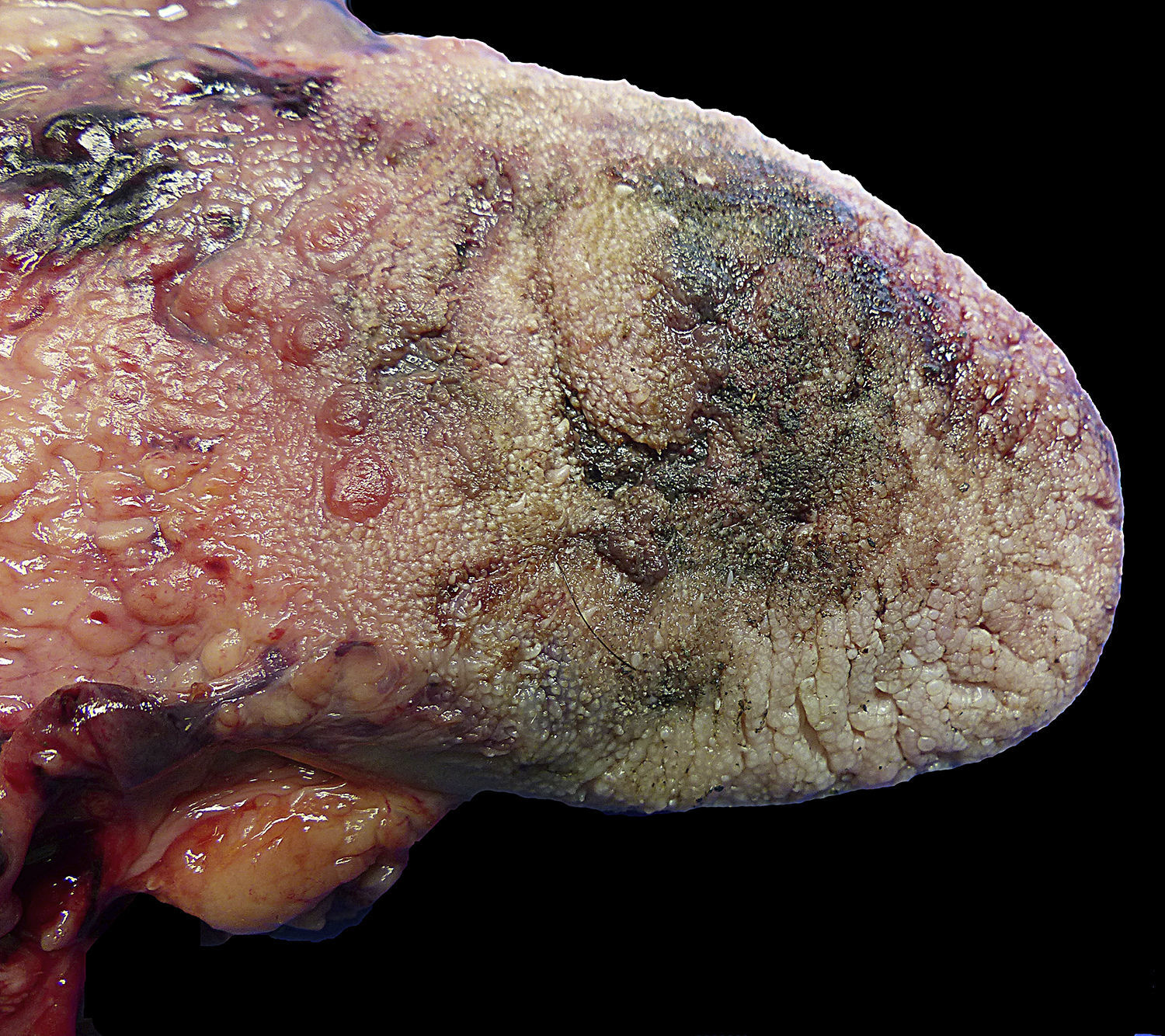
Distance: intraoral. Direction: anteroposterior, very slightly caudocranial and to the left. Exit: left occipitoparietal. Etiology: suicide. Type of firearm: shotgun (single bullet).
40-Year-old man, found at his home with the firearm next to his body. History of depression. The autopsy showed injuries caused by single shot, with contusions on the lips (Fig. 7), tears in the lingual posterior third and burns on the pharynx, larynx and tongue, more severe on the left side (Fig. 8). Palate crossed at the posterior third, with extensive facial fractures and cranial fracture.
Conclusions.")
.")
Several variables have been suggested for differentiating the causes of firearm-related deaths by homicide and suicide, some referring specifically to mouth injuries.
The victim's being male, the home as the site of the incident, the use of a long gun and a single shot fired are characteristic features of suicide with a firearm. In intraoral wounds, the bullet usually follows an anteroposterior and bottom-to-top (caudocranial) trajectory, passing through the palate, without directly damaging the teeth, lips and tongue, although they are damaged by other elements of the gunshot wound.
In homicides, by contrast, these results are more variable, with the use of handguns and multiple shots being common. In rare intraoral cases, the bullet may directly injure the lips and teeth, passing through the tongue in its trajectory.
Conflicts of interestThe authors declare that there are no conflicts of interest.
We would like to thank the Pathology Department at the Legal Medicine Institute of Alicante. Dr Sandostatin García and Dr Miguel Ángel Castillo.
Please cite this article as: Dorado-Fernández E, Andreu-Tena E, Magaña-Loarte C, Ruiz-Tagle Fernández E, Cáceres-Monllor D, Souto López-Mosquera JL, et al. Muertes por arma de fuego y disparo intraoral: etiología medicolegal. Rev Esp Med Legal. 2017;43:70–78.