




Información del artículo
Resumen
Texto completo
Bibliografía
Descargar PDF
Estadísticas
Figuras (3)
Mostrar másMostrar menos
Tablas (1)
Tabla 1. DIAGNÓSTICO DIFERENCIAL DEL HIPERTIROIDISMO POR AMIODARONA
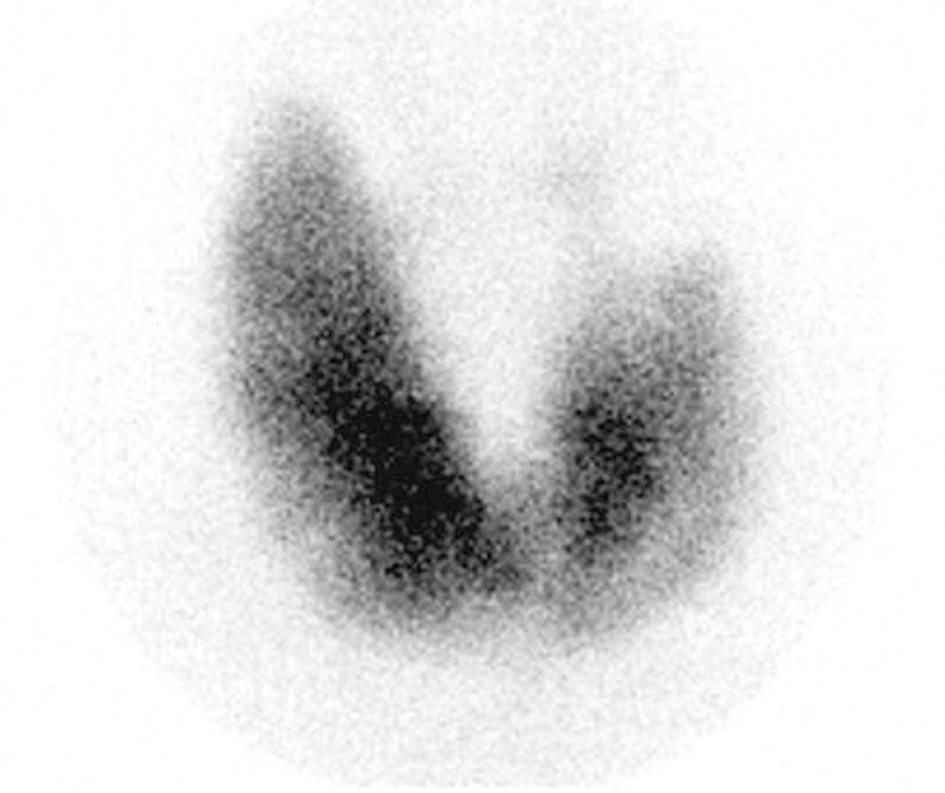
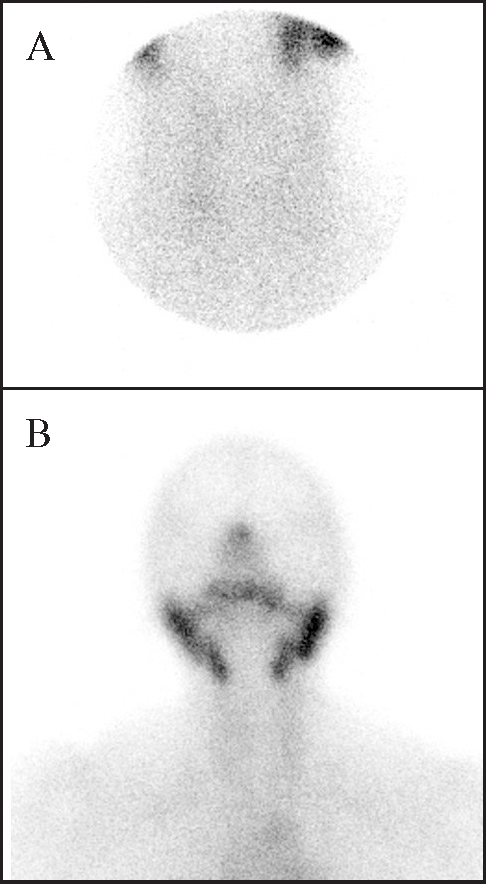
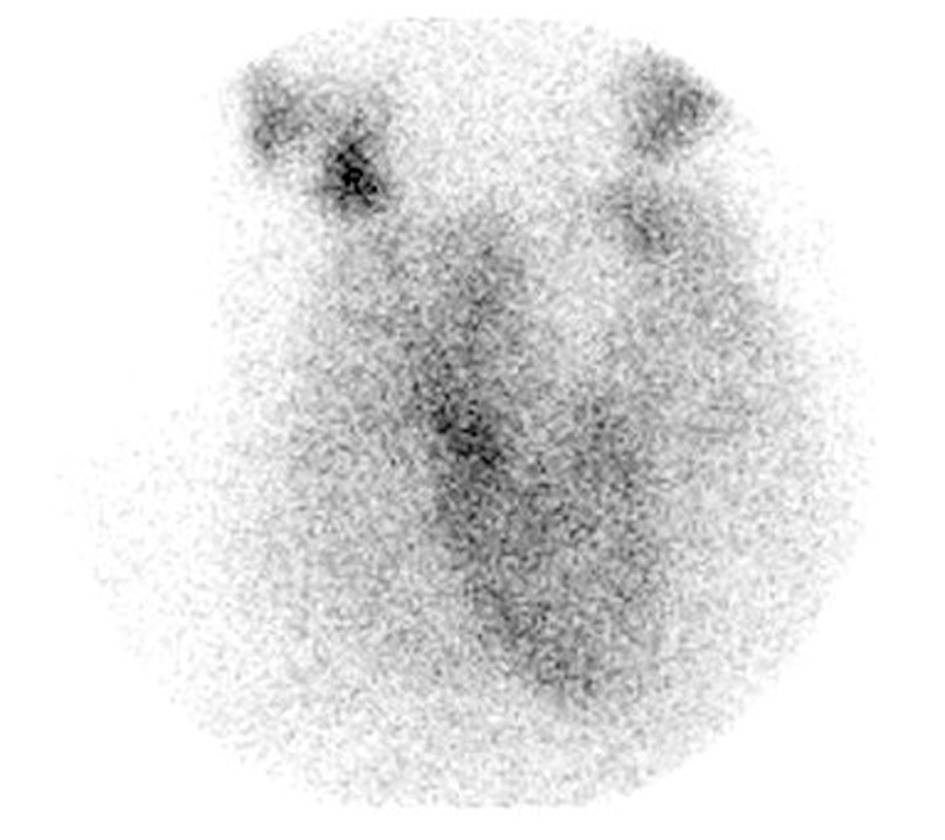
Amiodarone-induced hyperthyroidism is relatively common in iodine-deficient regions. Two types have been described: type I, caused by increased synthesis and release of thyroid hormone in individuals with underlying thyroid disease, can be treated with antithyroid drugs or radioiodine; and type II, a destructive thyroiditis responsive to corticoid therapy but not to antithyroid drugs. It can be difficult to distinguish between the two types, and cases of mixed types have been reported. Objective. to assess the usefulness of thyroid scintigraphy in amiodarone-induced hyperthyroidism. Materials and methods. 27 consecutive patients (13 females) with amiodarone-induced hyperthyroidism. Mean age was 65 years (range: 39-89). All patients underwent 99mTc-pertechnectate thyroid scintigraphy and were classified according to the qualitative estimation of radiotracer uptake: type I (increased / normal uptake): 9 patients, all of whom responded to antithyroid drugs or radioiodine, except one patient with sub-clinical hyperthyroidism who received no therapy; type II (very low or undetectable uptake): 13 patients, 11 of whom responded to discontinuation of amiodarone or prednisone therapy (2 patients). Hyperthyroidism was resistant in 2 patients and required antithyroid drugs or potassium perchlorate; mixed type (low uptake but with underlying thyroid pathology): 5 patients, with variable evolution; all needed antithyroid drugs, one required subtotal thyroidectomy, and another radioiodine treatment. Conclusion. thyroid scintigraphy can establish the correct therapeutic approach in most cases of amiodarone-induced hyperthyroidism, making it essential in the clinical management of these patients.
Keywords:
hyperthyroidism, thyroid dysfunction, amiodarone, thyroid scintigraphy, thyroiditis
Artículo
Opciones para acceder a los textos completos de la publicación Revista Española de Medicina Nuclear e Imagen Molecular
Socio
Si es usted socio de la Sociedad Española de Medicina Nuclear e Imagen Molecular (SEMNIM) puede acceder al texto completo de los contenidos de la Revista Española de Medicina Nuclear e Imagen Molecular desde los enlaces a la revista publicados en la web de la SEMNIN (enlace a https://semnim.es/iniciar-sesion/), previo inicio de sesión como socio. Si tiene problemas de acceso puede contactar con la Secretaría Técnica de la SEMNIM en el correo electrónico secretaria.tecnica@semnim.es o en el teléfono: + 34 619 594 780
Suscriptor
Suscribirse

Comprar
Comprar acceso al artículo
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora
Contactar
Teléfono para suscripciones e incidencias
De lunes a viernes de 9h a 18h (GMT+1) excepto los meses de julio y agosto que será de 9 a 15h
Llamadas desde España
932 415 960
Llamadas desde fuera de España
+34 932 415 960
E-mail
