



There is not enough evidence in form of clinical studies regarding the behavior of the midfoot joints in dynamic situations such us walking or running. The present work aims to study the mechanical behavior of midfoot joints with a multisegmented foot model with special interest in joint moments and their clinical significance.
Subjects and methodsA computerized 3-dimensional gait study was performed on healthy male adult subjects with a neutral Foot Posture Index (FPI) (from 0 to +5) during walking. Joint angle and external moments were estimated with a multisegment foot model that considers three separate segments (forefoot, rearfoot and hallux) and graphs and values of midfoot joint (joint connecting forefoot to rearfoot) were analyzed for the right foot of all participants.
ResultsA total of 30 subjects (27.13±3.82 years) were included in the study. Highest external moments were observed in the sagittal plane in dorsiflexion direction which tend to collapse the longitudinal arch during the stance phase. Moments registered in frontal and transverse planes were much lower than those observed in the sagittal plane and seems to have lower clinical relevance.
DiscussionThe present study provides data about the mechanical behavior of midfoot joints in a healthy adult population with a neutral FPI. This work shows that plantar soft tissues are subjected to important tensional stress during the stance phase of walking.
No existe todavía suficiente evidencia en estudios clínicos respecto al comportamiento del mediopié en situaciones dinámicas como la marcha o la carrera. El presente estudio pretender analizar el comportamiento mecánico de las articulaciones del mediopié mediante un modelo multisegmental del pie con especial atención a los momentos articulares y sus repercusiones clínicas.
Sujetos y MétodosSe realizó un estudio computerizado de la marcha sobre 30 sujetos adultos sanos (27,13±3,82 años) con un Índice de Postura del Pie (FPI) neutro (entre 0 y +5). Se estimaron los ángulos y momentos articulares externos en 3 dimensiones mediante un modelo que considera 3 segmentos (antepié, retropié y hallux) y se analizó la evolución de dichas variables durante la marcha sobre la articulación del mediopié (articulación que conecta antepié y retropié) del pie derecho de todos los sujetos.
ResultadosLos mayores momentos articulares observados se dieron en el plano sagital en flexión dorsal produciendo una tendencia al colapso o aplanamiento del pie durante la fase de apoyo de la marcha. Los momentos articulares registrados en el plano frontal y transverso fueron de una magnitud mucho menor a la observada en el plano sagital y de menor relevancia clínica.
DiscusiónEl presente estudio aporta datos sobre el comportamiento mecánico de las articulaciones del mediopié en una muestra de 30 sujetos sanos con un FPI neutro. Este estudio muestra la importancia del estrés tensional al que se encuentran sometidas las estructuras blandas plantares durante la fase de apoyo de la marcha.
Nowadays, there is still controversy regarding normal and abnormal mechanical behavior of midfoot joints during dynamic situations such us walking or running. Although several theoretical models have been described for some midfoot joints such us those described for the midtarsal joint,1–3 there is not enough evidence in form of clinical studies about the mechanical behavior of these joints, including midtarsal joint.
In the last years, multisegmented foot models have gained popularity in the study of the mechanics of the foot during dynamic conditions. Those models divide the foot into different segments such us rearfoot or forefoot and allow a more precise study of the mechanical characteristics of different parts or segments of the foot and ankle. Presently, there exists several foot models4–7 that segment the foot in different ways and that has been used in different studies that explored the mechanical behavior of the foot and a better understanding of foot kinematics has been acquired in those studies.8,9 However, addition of kinetic variables (such us joint moments and powers) to these models has been much more limited by technical issues, mainly the location of forces in each segment and the estimation of joint centers.10–12 Recently, Bruening et al.13,14 developed a multisegment foot model that uses the leg as a rigid segment (tibia and fibula together) and also divides the foot in three different segments: rearfoot (calcaneus and talus), forefoot (navicular, cuboid, cuneiforms and metatarsals) and Hallux. This model, that used two force platforms and three measurements with different foot positions in the platforms, has been shown to be valid for the kinetic study of the foot in three joints: ankle joint, midfoot joint and first metatarsophalangeal joint.14
At the same time, most of the kinetic studies performed in “biomechanical laboratories” have been limited in their application to clinical practice. It seems to exists a disconnection between the results obtained in biomechanical studies that were accomplish on laboratories and their application to clinical world. This problem has been a constant in the history of biomechanics.15 Most of these problems lie in the difficult interpretation of the physical and mathematical languages in which laboratory results are usually expressed. These data are not intuitive for most health professionals and his immediate clinical application is usually delayed. Obviously, the lack of understanding between the biomechanical research and clinical practice has slowed down biomechanical progress and application of treatments to patients. For this reason, this paper tries to describe the mechanical behavior of midfoot joints from a clinical point of view (with special emphasis on kinetics) obtained in a sample of normal male subjects.
Patients and methodsA computerized gait analysis was performed in healthy normal subjects between January 2015 to March 2015. Subjects for the study were recruited as patients or partners of the first author of this paper (E.S.S.) or as students of Universidad Jaume I (Castellón, Spain). Inclusion criteria included subjects without history of neuromuscular problems, foot and ankle surgery or diabetes and whose Foot Posture Index (FPI) was between 0 and +516 to avoid excessively pronated or supinated cases. All of the participants provided written informed consent to participate in the study, which was approved by the ethical committee of the University Jaume I (Castellón, Spain).
Each subject was asked to walk barefoot at a self-selected speed along a 7m walkway. Before data collection, subjects were trained, walking on the walkway several times. The subjects faced forward while walking avoiding platform targeting, and they had to step with his right foot on a pressure platform located in the middle of the walkway. The activity was repeated as many times as required to have five valid trials from each subject, discarding those where the subject did not step on the platform with the right foot.
Gait evaluation included simultaneous recording of body kinematics and the normal component of ground reaction force with a pressure platform. The kinematics of the ankle, midfoot joints and first metatarsophalangeal joint were recorded using an adaptation of the model proposed by Bruening et al.13 The model considers the shank and the foot divided in three segments – rearfoot, forefoot, and hallux – connected by the ankle joint (which connects rearfoot segment to leg segment), midfoot joint (MT) (which connects forefoot segment to rearfoot segment), and metatarsophalangeal joint (MP) (which connects hallux segment to forefoot segment) (Fig. 1). The model uses 20 reflective markers attached to anatomical reference points of the leg and foot of the subjects of the study (Fig. 1). Three-dimensional (3-D) motions of the 20 markers were measured by an eight – infrared camera motion analysis system (Vicon® Motion Systems Ltd., Oxford, UK) operating at a 100Hz sampling rate. The 3D coordinates of the markers at each instant were used to obtain segment position and orientation.17 Finally, joint angles at each instant were calculated from the upright standing static reference posture, which was recorded to each subject at the beginning of the experiment. The joint angles were obtained using a Cardan rotation sequence between distal and proximal segments18: 1 – dorsiflexion/plantarflexion (DF/PF), 2 – abduction/adduction (AB/AD), 3 – inversion/eversion (IN/EV). All kinematical data were low-pass filtered using a 4th order Butterworth filter with a cut-off frequency of 10Hz.

To obtain the joint moments at the ankle, MT and MP joints, the contact pressure distribution was used along with the location of the joint centers obtained from the Bruening model. The contact pressures were recorded at a 100Hz sampling rate with a 0.40m×0.40m Podoprint® pressure platform (Namrol Group, Barcelona, Spain) which was synchronized with the infrared camera system. Pressure data was segmented by comparing the contact cell coordinates with the anteroposterior location of ankle, MT and MP joint centers. Then, the total normal ground reaction force was calculated at each segment along with its corresponding center of pressure (CoP). The 3D joint moments were calculated as the cross product of the ground reaction forces on distal segments (obtained by the pressure platform) and the 3D distances between the CoPs and the joint centers, thus neglecting the effect of the weight of the foot, as well as the effect of foot angular velocity and linear and angular accelerations.19–21 Joint moments were expressed relative to the orientation of the local frame of the proximal segment. All joint moment data were low-pass filtered using a 4th order Butterworth filter with a cut-off frequency of 50Hz, and, consistently with previous publications,19,20 the amplitudes were normalized to body weight. Joint moments were reported as external moments.
A descriptive analysis of the midfoot joint angles and moments in DF/PF, AB/AD and IN/EV of the stance phase across subjects and trials were computed. Values observed were presented in form of a graph plotted versus time as a percentage of stance phase, along with the 95% confidence interval (CI). Each subject parameter was computed as the mean of the five valid trials recorded and that parameter was used as representative of each subject. Mean and standard deviation (SD) of these values across subjects were obtained as representative of the healthy adult population.22,23
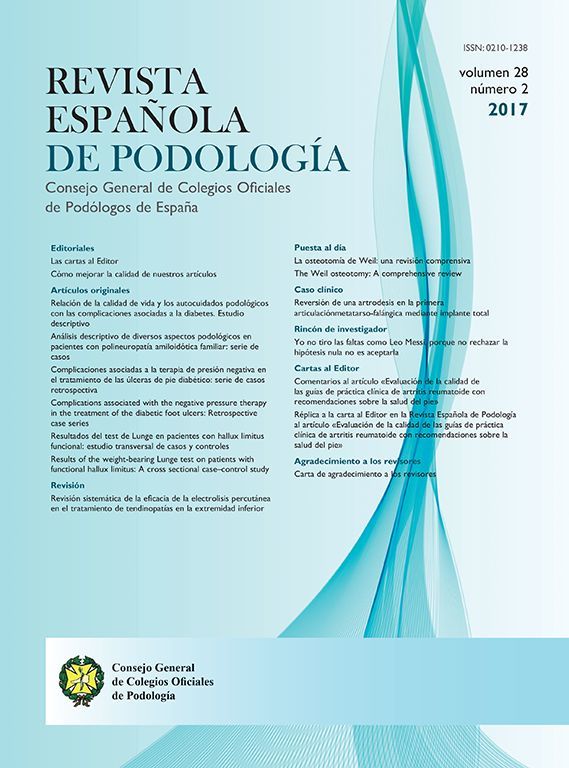
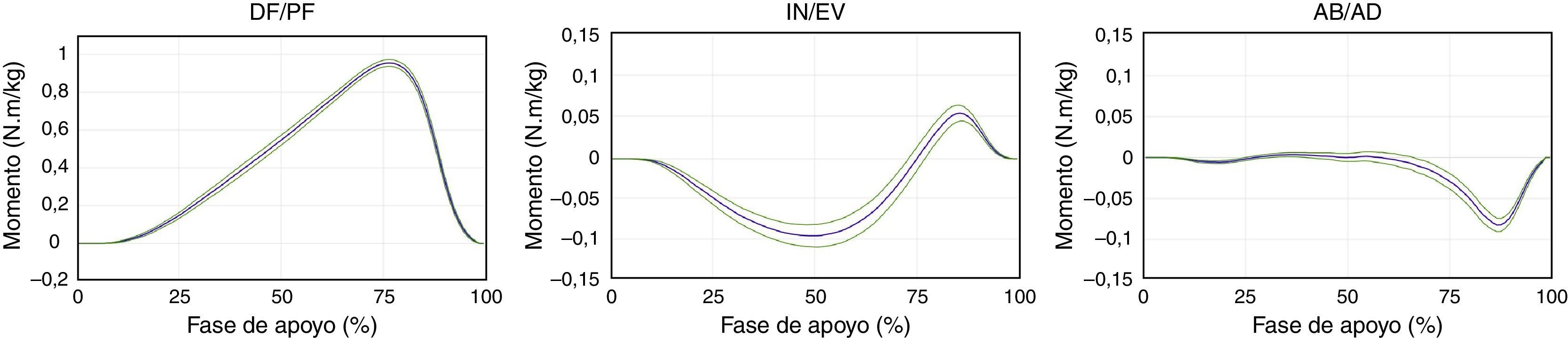
ResultsA total of 30 healthy normal subjects were included in the study. Table 1 shows descriptive data of the sample of study, including the FPI value. Figs. 2 and 3 show the graphs of moments and excursions of the midfoot joint in the three planes during the stance phase of walking corresponding to the right foot of all the subjects included in the study. Graphs show the mean of all the subjects of the study along with a 95% confidence interval throughout the whole stance phase.

Joint moments of the midfoot joint during the stance phase of walking. Moments are presented in the sagittal, frontal and transverse plane along with 95% confidence interval. Graph has been obtained as the mean of all trials across the 30 subjects of the study normalized by the body weight of each subject. Dorsiflexion, inversion and abduction are presented as positive values. Note that a bigger scale has been used to represent moments in transverse and frontal plane because of the differences in ranges with the sagittal plane.

Joint movement of the midfoot joint during the stance phase of walking. Angles and movements are presented in the sagittal, frontal and transverse plane along with 95% confidence interval. Graph has been obtained as the mean of all trials across the 30 subjects of the study. Dorsiflexion, inversion and abduction are presented as positive values. Note that a bigger scale has been used to represent moments in transverse and frontal plane because of the differences in ranges with the sagittal plane.
Of the moments reported in the three planes, sagittal plane moments were those of the biggest magnitude compared with the other two planes (8 times bigger than the transverse and frontal plane). The moment presented in the sagittal plane tend to dorsiflex midfoot joints during the stance phase. It starts approximately at 10–15% of stance phase and increase gradually till the middle of the propulsive phase when the heel has been taking off the ground. At that point it slowed down quickly. Movement registered of the midfoot joint was also into dorsiflexion during the first 75–80% of the stance phase (maximum peak of 7.60°±1.81). Finally, midfoot joint plantarflexed during the last part of the propulsive phase.
In the frontal plane, joint moments of the MT showed an external eversion moment during the first 75% of the stance phase. The graph also shows a gradual increase that reaches its maximum peak at approximately the 50% of the stance phase. After reaching its maximum value, external pronation moments decreased progressively till null and then became supinator in the propulsive phase. Magnitude of these moments are much lower than those observed in the sagittal plane. Movement of the MT in the frontal plane was in eversion from heel strike to full forefoot load. Once this eversion movement occurred during the contact period, the MT was stable without movement during the whole midstance of the stance phase till propulsive phase in which supination movement of the midfoot joint occur (maximum peak pronation of 2.20°±1.77).
In the transverse plane, obtained moments were basically null during most of the stance phase. However, an abductor external moment peak of low magnitude appeared in the propulsive period. Movement of the midfoot joint in the transverse plane was into abduction between heel strike and full forefoot load (maximum abduction peak of 2.43°±1.02). As the same as in the frontal plane, the movement in the transverse plane after full forefoot load was stable in a slightly abducted position without movement during most of the midstance period till the foot entered the propulsive phase in which a small abduction movement occurred.
DiscussionThe term kinetics is used in biomechanics to describe the relationship between the forces and the movement produced in a joint. Connections between bones (joints) are not completely rigid and allow different types of movements. Those movements are produced by both internal forces (derived mainly from muscular activity, capsuloligamentous restrictions and forces derived from osseous contact) and external forces (derived mainly from body weight or ground reaction forces). Kinetic studies try to relate joint angles and movements during dynamic situations to joint moments. Modern systems for gait analysis use the kinematic data registered (joint movement) and kinetic data (mainly from ground reaction) to calculate net joint moments about a particular joint. Net joint moments are the final result of all forces (internal and external) acting on a particular joint. From a mathematical point of view, it can be defined as the product of the final force multiplied by the minimum perpendicular distance to joint axis. Clinically, it can be interpreted as the “tendency” to rotation that the sum of all forces generate over a particular joint. The present study has tried to described three-dimensional moments of a midfoot joint that connects forefoot to rearfoot in the multisegment model described by Bruening et al.13 in a healthy adult sample. Till date, authors do not have knowledge of previous reports that have studied these variables in an adult sample with a neutral position of the foot under the criteria of the FPI. Data of the joint moments obtained in the present study are quite similar to those reported by Bruening et al.14 in a sample of 17 pediatric patients.
Data obtained has shown that bigger moments in the midfoot joint are produced in the sagittal plane into dorsiflexion being the magnitude of that moment eight times bigger that those reported in the frontal and transverse planes. The graph displayed shows a dorsiflexion moment similar to that reported for ankle joint in other studies24–26 excepting for the external plantarflexion moment at the contact period of the stance phase. These findings show that midfoot joints would be subject to dorsiflexion moments during most of the stance phase of walking with a maximum peak just after heel off. This finding can be appreciated clinically as the tendency to flattening or collapse of the longitudinal arch of the foot during midstance and propulsion (from full forefoot load to heel off) being that collapse bigger just after heel off. From a clinical perspective, it is important to understand that those dorsiflexion moments should be controlled by tensional forces generated by muscle contraction and plantar soft tissue tension (including plantar fascia) opposing the dorsiflexion moments. Those plantar structures slowed down the external dorsiflexion moments of the midfoot joints creating a plantarflexion moment of the forefoot to avoid arch collapse. The bigger the external dorsiflexion moments acting on the midfoot joints, the bigger the contractile and tensional forces of the musculo-ligamentous structures of the plantar foot will be. It is possible that this data could be implicated in the genesis of some disorders such us plantar fasciitis, abductor hallucis muscle miositis or any other type of intrinsic muscular disorder. It would be interesting to look at the external midfoot joint dorsiflexion moments in the genesis of particular plantar disorders in future prospective studies.
Movement of the midfoot joints in the present study has been shown to be very stable during midstance (from full forefoot load to heel off) in the frontal and transverse planes. In fact, movement graphs in these planes show that the MT moves into abduction and eversion during heel contact period. Afterwards, once full forefoot load has completed, movement of the MT in transverse and frontal plane is stable in a fixed position that is maintained during the whole midstance period till heel takes off the ground. At that time, movement of the midfoot joint appears again. It is not clear which is the exact mechanical reason of this finding, but it seems that tension generated of plantar soft tissues created by body weight could act as fixation system of the midfoot joints, especially in the transverse and frontal planes. However, this process does not happen in the sagittal plane in which midfoot joint deforms gradually till reach a maximal a dorsiflexion peak of 7.60°±1.81. As has been mention, magnitudes of joint moments are much more bigger in the sagittal than in the other two planes.
Another relevant point of the present study is that kinematic and kinetic results of the sample have shown a narrow confidence interval compared to other reports. Nester et al. have pointed great interindividual variation in the movement of foot and ankle joints when normal healthy subjects are subjected to study.8,27 These authors have hypothesized that normal healthy subjects (asymptomatic) can have different and very diverse kinematic patterns that could be considered normal. The present study analyzed walking kinematics and kinetics of 30 healthy male subjects (no pain in foot of lower extremity) with a very similar FPI between them (between 0 and +5). The 95% confidence interval in the kinematic value seems to be narrower than those reported in other studies that did not take the FPI factor into account. It would be interesting to analyzed this factor in future studies to investigate if different foot postures could have some influence in the kinematic patterns of the subjects during walking or if there are other more predominant factors (such us neuromuscular activation) that could drive the kinematic pattern of subjects.
This study has some limitations and its results should be taken cautiously. First, sample obtained was not randomized because it was obtained from patients and relatives of the first author of the paper (E.S.S.), so some kind of bias could have affected the selection of the sample. Second, like all foot multisegment models, the model join together several bones depicting one rigid segment. Obviously, kinematic and kinetic descriptions represent the mechanical behavior of different joints together (i.e. rearfoot segment combines the movement of ankle and subtalar joint together). This aspect is especially important in this study of midfoot joints as errors can be introduced describing the movement of the segment forefoot to the segment rearfoot in which several joint are mixed together in the “midfoot joint”.7 In the present study, forefoot segment combines midtarsal, naviculocuneiforms and Lisfranc joints in one rigid segment, and MT behavior described represents the sum of all those joints together. Third, for joint moments calculation a pressure platform was used. This system allows for the calculation of the normal component of the ground reaction forces but not the friction component. So, basically pressure platforms allow registration of ground reaction forces in the sagittal plane and calculation of joint moments in the frontal and transverse planes are subjected to limitations. However, Hunt et al. found no differences comparing ankle joint moments with and without considering frictional forces concluding that joint moments at the ankle were not significantly different when frictional forces were considered.28 At the same time, for the calculation of joint moment data relative to acceleration and velocity of foot segment were obviated. This aspect could be a limitation of the study although it would be much more important in the study of swing phase moments and not in stance phase moments in which foot acceleration and velocity are less important.
In conclusion, the present study gives kinematic and kinetic data of the midfoot joint during walking using a multisegment foot model based in that described by Bruening et al.13 from an adult male healthy sample of 30 subjects and with and neutral FPI. Dosiflexion moments in the sagittal plane were much more higher than in any other plane generating a tendency to collapse o flattening of the longitudinal arch with the subsequent stress that those moments create in plantar soft tissues. Joint moments in the frontal plane had much lower magnitude than those observed in the sagittal plane and tend to move the foot into eversion during midstance period. Transverse plane moments were basically null during most of stance phase showing some low activity in propulsion. Transverse and frontal plane moments seems to have a lower clinical significance than those produced in the sagittal plane in the MT joint.
Financial disclosureNot present.
Conflicts of interestThe authors declare no conflict of interest.