



Functional hallux limitus (FHL) is a well-known multifactorial functional disruption defined as a clinical entity characterized by the difficulty of loading the metatarsal-phalangeal joint of the first finger to the dorsal flexion when weight-bearing. The objective of this study is to verify a possible relationship between a decrease in dorsiflexion of the talocrural joint with a limitation of the first phalangeal metatarsal joint.
Patients and methodsWeight-bearing Lunge test (WBLT) values of 26 participants were analyzed, 13 had FHL and 13 were controls. FHL test and WBLT were performed to the total of the sample. Three measurements were made for the WBLT to obtain its result as mean±standard deviation in order to relate it to the presence of HLF. The T-Student test was performed on independent samples comparing the WBLT results on the cases and controls groups. The left and the right limbs were analyzed for the sample and a distinction was made between genders.
ResultsStatistically significant differences were found between the cases group and the control group at the dorsal flexion range of motion for the right leg (30.84±2.820 vs 34.92±1.93; p<0.05) but not for the left leg (31.00±4.000 vs 34.30±2.56; p=0.19). In relation to the gender, the differences between cases–control were equally significant for the female and male genders on the right leg, but not on the left.
ConclusionsBased on the results obtained in the study, an association between HLF and a decrease in the range of motion of the talocrural joint has been found, although further studies are needed in order to correlate this biomechanical relation.
El hallux limitus funcional (HLF) es una alteración funcional de carácter multifactorial que se caracteriza por la dificultad que presenta a la flexión dorsal en carga, la primera articulación metatarsofalángica. El objetivo de este estudio es comprobar una posible relación entre una disminución de dorsiflexión de la articulación talocrural con una limitación de la articulación metatarsofalángica.
Pacientes y métodosSe analizaron los valores del Weight-Bearing Lunge Test (WBLT) de 26 participantes, de los cuales 13 presentaban HLF y 13 controles. Se realizaron los test de HLF en descarga y WBLT en carga al total de la muestra, realizándose 3 mediciones para el WBLT para obtener su resultado como media±desviación estándar con el objetivo de relacionarlo con la presencia de HLF. Se realizó la prueba de la t de Student para muestras independientes comparando el resultado del WBLT en los grupos de casos y controles. Se analizaron los miembros derecho e izquierdo en toda la muestra y diferenciado también por sexos.
ResultadosSe encontraron diferencias estadísticamente significativas entre el grupo de casos y controles en el rango de flexión dorsal en la pierna derecha (30,84±2,820 vs. 34,92±1,93; p<0,05) pero no en la pierna izquierda (31,00±4,000 vs. 34,30±2,56; p=0,19). En relación con el género, las diferencias entre casos y controles fueron igualmente significativas para el sexo femenino y el masculino en la pierna derecha, pero no en la izquierda.
ConclusionesSobre la base de los resultados obtenidos en el presente estudio, se ha encontrado asociación entre la presencia de HLF y la disminución del rango de movilidad de la articulación talocrural, aunque son necesarios más estudios que evidencien esta relación biomecánica.
Functional hallux limitus is known as a functional disruption characterized as a difficulty in the dorsiflexion movement of the first metatarsophalangeal joint of the first ray when weight bearing. The condition is considered to be multifactorial.1,2
On the first stages, FHL is characterized for not getting, in closed kinetic chain, 20° dorsiflexion, while in opened kinetic chain the first metatarsophalangeal joint maintains the 65°–75° dorsiflexion.3 As the condition progresses, a degeneration of the articulation occurs and in non-weight bearing the first metatarsophalangeal joint does not get the 65°–75° dorsiflexion, the condition is then known as Hallux Limitus (HL). Clinical manifestations for HL are an intermittent pain at the level of the joint and a marginally deviation of the sesamoids bones. The progression of this functional disruption is known as Hallux Rigidus and it is characterized by a limitation in the metatarsophalangeal joint to less than 10° dorsiflexion. At this stage, the articulation loses its space and osteophytes and a deformity of the sesamoid bones can be seen.1,2
Those functional disruptions are, together with Hallux Valgus, the main first ray conditions. Furthermore, the first metatarsophalangeal joint is the most prevalent site of arthrosis after the knee joint.4,5
From a biomechanic point of view, a good range of motion of the first metatarsophalangic joint articulation in the sagittal plane is essential during gait. Therefore, 65°–75° hallux dorsiflexion are needed in order to keep an effective progression of the center of mass in the phase of propulsion during gait.6
For an optimal performance of the joint, many factors have to be taken under consideration such as the action of the Flexor Hallucis Brevis muscle, the hallucal sesamoid complex, joint capsule and the plantar fascia.7,8
The consequences of FHL include the variation of the pressure center, an increase of pressure under the first metatarsal head, an increase of pronation in the midfoot joints, the appearance of an abductory twist, lack of knee extension during gait and an early heel strike at the initial contact.9
The clinical tests used to determinate the absence or presence of FHL were described by Payne and Dananberg.10
On the other hand, the ankle joint, also known as talocrural joint, is one of the most important and complexes articulations of the foot. The dorsiflexion (DF) movement of the talocrural joint allows the movement of plantar flexion and dorsiflexion. A good range of DF is necessary for daily life activities such as walking, running, going up the stairs, stand up from a chair and bend down.11 Therefore, a limitation of the DF movement is originating an abnormal function of the foot and consequently, a functional dysfunction of the foot.12,13 The evaluation of the DF range of motion of the talocrural joint is essential in order to identify the risk factors of many lower limb injuries.13
The Lunge test or WBLT is a clinical exploration protocol scientifically validated. Frequently used in the scientific literature in order to quantify the deficiency of range of motion in the talocrural joint during DF.14,15 Due to the importance of the DF movement during gait, the WBLT is a recurrent clinical test used by those practitioners that deal with lower limb pathologies. Furthermore, the WBLT is also used to detect deficiency of range of motion in those subjects with history of traumatic pathologies, knee instability and control the progress during the rehabilitation process.16,17 Prospective studies have shown that the WBLT can also be used as a predictor of injuries.18,19
The presence of the limitation of movement in the first metatarsophalangeal joint in dynamic can cause an inadequate activation of the Windlass mechanism that could lead to an excess of stress placed on the plantar fascia.8 Due to the believe that the body works in muscle chains,20 the tension would be then transmitted through the Achilles-calcaneus-plantar system to the triceps surae, leading to a shortening at this level.21,22 All those theories encouraged us to find a possible biomechanical correlation between the functional imbalance FHL and a shortening of the gastrocnemius and soleus group.
The hypothesis of this study establishes the existence of significant differences in the result of the WBLT between a group of subjects that suffer FHL and a group of healthy subjects. The main objective of this study is to prove the possible co-relation between a limitation of the ankle dorsiflexion measured with the WBLT and the presence of FHL in a group of young and healthy subjects.
Patients and methodsStudy populationThe data of the study belongs to a sample composed by men and women that attended Podoactiva's central podiatry and biomechanics clinic in Huesca (Spain), to realize a preventive biomechanical study, some of them were then diagnosed with a HLF on both feet. The study was approved by the Research Ethics Committee of the Autonomous Community of Aragon (Spain). In addition, an informed consent of all the volunteer participants was required in order to authorize the realization of the study.
Demographic data from the subjects included in the study was registered, including sex, age, height, weight and Body Mass Index (BMI). In addition, Foot Posture Index (FPI) was registered following the protocol established by Redmond.23 In order to be eligible for the study, subjects had to meet the following inclusion criteria: at least 18 years of age and not older than 50 years old, signed written informed consent and a normal BMI. None of the enrolled subjects was undergoing rehabilitation treatment at the moment of the study or underwent lower limb surgery. Patients who, at the start of the treatment, did not meet any of the inclusion criteria were not eligible for the study. Patients were admitted to the study in order of arrival to the podiatry clinic and then classified into the cases group, if HLF, and into the control group if the subject did not present with a HLF.
Measurement of variablesAll the data collection took place in March 2017 by the same podiatrist specialized in biomechanics and with 8 years of experience. The FHL test was performed non-weight bearing and the WBLT was done weight-bearing to all the participants. Both tests have been validated.11,21,22 Patients were placed bipedal, with one of their feet set back into a comfortable position. Secondly, instructions were given in order to obtain ankle DF on the advanced feet. Range of motion was measured in degrees using the Tiltmeter (IntegraSoftHN – Carlos E. Hernández Pérez) mobile application locating the phone on the posterior side of the tibia (Achilles tendon path) (Fig. 1).26 Afterwards, the same procedure was then used for the other limb.

In order to test the FHL, subjects were asked to lie down on a supine position on a clinical couch. Instructions were given to avoid any kind of voluntary contraction, and DF of the first metatarsophalangeal joint, repeating the same procedure three times in each foot. The clinician assessed the congruence, degrees of articular movement and the condition of the mechanism (Fig. 2).6,10

In total, three measurements of the WBLT were performed in order to obtain the result as a median±standard deviation (SD), with the aim to relate the result with the presence of FHL.
Data analysisRelating to the statistical analysis, firstly, exploratory analysis of the data was carried out. The quantitative variable was expressed as a median±SD. In order to assume or not equal variances (p<0.05), the Levene test for the equality of variances was performed. The median comparison between the two study groups was made by the T-Student test for independent samples. The Shapiro–Wilk tests did not show alteration on the data of the sample.
The data analysis was carried away with the statistic pack SPSS 22.0 for Windows (SPSS Ibérica, Madrid, Spain). Statistical significance was set at a p-level below 0.05.
ResultsThe sample of this study is composed of 26 young individuals between 21 and 27 years old (mean 24.23±1.96 years), without gender discrimination (15 male and 11 women). The group was classified in 13 subjects (cases) diagnosed with FHL and 13 healthy subjects (controls) without FHL.
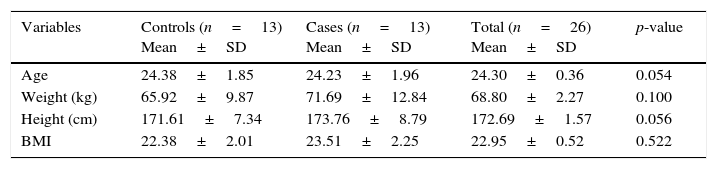
The analysis on the distribution of the data, using the Shapiro–Wilk test, shows a normal behavior for all the variables. Table 1 shows the results of the analysis of the demographics that form the sample of the study.
Analysis of the differences in demographic data using T-Student.
| Variables | Controls (n=13) Mean±SD | Cases (n=13) Mean±SD | Total (n=26) Mean±SD | p-value |
|---|---|---|---|---|
| Age | 24.38±1.85 | 24.23±1.96 | 24.30±0.36 | 0.054 |
| Weight (kg) | 65.92±9.87 | 71.69±12.84 | 68.80±2.27 | 0.100 |
| Height (cm) | 171.61±7.34 | 173.76±8.79 | 172.69±1.57 | 0.056 |
| BMI | 22.38±2.01 | 23.51±2.25 | 22.95±0.52 | 0.522 |
BMI: Body Mass Index.
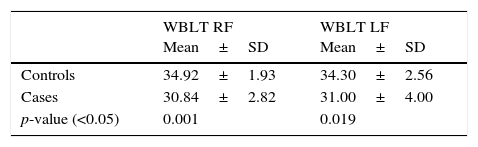
Analysis on the distribution of the WBLT data also shows a normal behavior for the control group and cases. Of the total of 13 subjects measured with the FHL is observed how the range of DF on the ankle on the left foot has an average of 31.00°±4.00° while on the right foot, the average is 30.84°±2.82°. As for the control group we observed that the average on the left foot is 34.30°±2.56° and 34.92°±1.93° in the right foot (Table 2).
Mean and standard deviation of the left foot and right foot of the control group and cases for the WBLT variable. T-Student value (p<0.05).
| WBLT RF Mean±SD | WBLT LF Mean±SD | |
|---|---|---|
| Controls | 34.92±1.93 | 34.30±2.56 |
| Cases | 30.84±2.82 | 31.00±4.00 |
| p-value (<0.05) | 0.001 | 0.019 |
RF: right foot; LF: left foot.
T-Student test.
The mean of the values obtained in the cases group on the right foot is 30.84°±2.82°, while on the left foot is 31.00°±4.00°, being greater than the result obtained in the group of the controls on the right foot 34.92°±1.93° and 34.30°±2.56° on the left foot; showing a statistically significant difference with a p-value=0.001 for the right foot and a p-value=0.19 in the left foot.
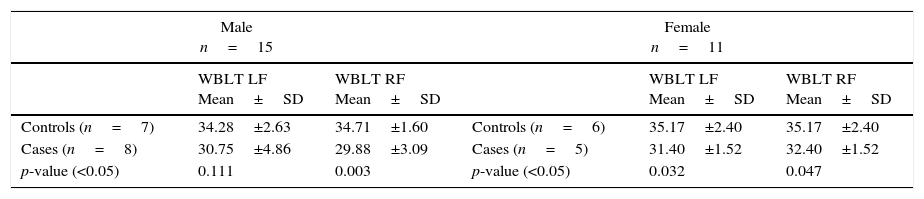
Comparison of data between the case–control groups according to gender can be seen in Table 3.
Gender case–control WBLT comparison.
| Male n=15 | Female n=11 | ||||
|---|---|---|---|---|---|
| WBLT LF Mean±SD | WBLT RF Mean±SD | WBLT LF Mean±SD | WBLT RF Mean±SD | ||
| Controls (n=7) | 34.28±2.63 | 34.71±1.60 | Controls (n=6) | 35.17±2.40 | 35.17±2.40 |
| Cases (n=8) | 30.75±4.86 | 29.88±3.09 | Cases (n=5) | 31.40±1.52 | 32.40±1.52 |
| p-value (<0.05) | 0.111 | 0.003 | p-value (<0.05) | 0.032 | 0.047 |
RF: right foot; LF: left foot.
T-Student test.
In the case of the male subjects, equal variances were assumed and it was obtained that for the right leg the difference of degrees in the WBLT was significant, not for the left one. As for the female sex, for the left leg no equal variances (p<0.05) were assumed, according to the Levene test, but not for the right lower limb. The difference between the case–control groups was significant for this gender.
DiscussionIn the present study we have evaluated whether there are significant differences when comparing the range of motion of the talocrural joint in healthy patients with a normal metatarso-phalangeal range of motion and patients with FHL. The results obtained in this study showed a significant association on the right limb but not on the left one between FHL and the decrease of ankle joint dorsiflexion.
We have managed to demonstrate one of the specific objectives of this study due to the fact that significant differences have been found between patients with HLF and healthy individuals in the range of motion of the talocrural joint, being higher the range of motion of this joint in healthy subjects.
In relation to an explanation that substantiates the results of the exposed hypothesis, there are many factors predisposing to the emergence of HLF. These include the contracture of the first ray flexor musculature, the existence of a metatarsus primus elevatus, a hypermobile first ray or a degenerative process such as osteoarthritis.3,24
The biomechanical explanation of the relationship between these two clinical entities is based on Dananberg's theory of the sagittal plane,6 due to the fact that a decrease or a difficulty to dorsiflexion of the metatarso-phalangeal joint of the first ray causes a difficulty to activate the Windlass mechanism.27 An increase in the tension of muscles and elements that compose it, during the digital takeoff or third rocker because the dorsiflexion of the metatarso-phalangeal, causes an activation of the plantar fascia, shortening its course. As a result, an increase of the muscular tension on the Achilles-calcaneus-plantar system occurs, following through soleous and gastrocnemius, causing a contraction and retraction of the same.28,29 The retraction of muscles on the posterior chain and the plantar foot muscles, cause a limitation on the plantarflexion and specially the dorsiflexion of the talo-crural joint.25,26
Another determinant factor on the difficulty to dorsiflex the ankle is an overpronation at any of the phases of the gait cycle, generating stress on the plantar facia.30 The stress on the plantar fascia can preclude the correct performance of the Windlass mechanism.31 The tension can be transmitted to the posterior back chain through the soleus and gastrocnemius muscles, leading to a difficulty of dorsiflexion on the talocrural joint.31 At the same time, an overpronation during the terminal stance or toe-off results in a overuse of the first metatarsophalangeal joint (MPJ), this arising in a deterioration of the first MPJ and an appearance of a FHL.32
Bennell et al.33,34 demonstrate no difference in the angle of DF of the talocrural joint in groups of young ballerinas, when compared to a control group of young individuals that do not dance ballet. This fact correlates to our hypothesis, linking a FHL with a decrease of DF of the ankle and worsening its prognosis.
According to gender comparison, for female the difference between cases and controls was significant in both legs. However, for the group of males this was only been fulfilled for the lower right limb but not for the left, which is strange after having performed the general comparisons, with no difference of sex between case and control groups, where differences in WBLT grades were significant in both limbs. It should be clarified that this study did not take into account the bilateralism of the subjects, which may have influenced these results, a concept advocated by some authors,35 but refuted by others, who assure that there are no differences in shortening – stretching of the muscular fibers between dominant and non-dominant limbs.36
As a concluding remark, and according to the preceding biomechanical explanation and the results obtained in this study, we can appreciate an association between FHL and the diminution of the range of movement of the talocrural joint. According to the results obtained in this study, there are statistically significant differences between degrees of DF of the talocrural joint in healthy young subjects with FHL when compared with subjects without FHL. These findings may be of great interest in clinical practice since FHL is one of the most frequent functional disruptions in podiatry and biomechanical consultations, so that in the face of a limitation on the WBLT, the presence of a FHL should be tested.
After this first observational study correlating cases and controls, further studies would be needed in order to demonstrate the biomechanical relationship between the FHL with the limitation of DF of the talocrural joint in more extensive and heterogeneous samples.
Conflict of interestsThe authors declare that they have no conflict of interest.