

The purpose of this study was to conduct a meta-analysis on the effects of neuropsychological rehabilitation procedures on the quality of life in non-Spanish-speaking individuals with some cognitive deficit. Sixteen studies published during the 2001–2012 period which yielded relevant information regarding the sample sizes used, the types of statistical contrasts, the evaluation instruments or pathologies among others, were analyzed. We carried out study following the usual estimation procedures, based on the definition of the effect size and the scrutiny of their relationship with relevant variables (e.g., sample sizes, type of population), or methodological variables (e.g., type of research or sampling design). The data analysis shows a statistically significant effect (r+=.38; p<.001) in all the variables associated with the characteristics of the intervention (duration, type of intervention, gender, year of publication and, more importantly, quality of life and neuropsychological outcomes). As a general conclusion, we were able to determine that Quality of Life (QoL) can improve, under certain conditions, through neuropsychological rehabilitation, but this change is not permanent.
El propósito de este estudio fue generar un meta-análisis sobre los efectos de la rehabilitación neuropsicológica en la dimensión Calidad de Vida en muestras de no hispano-hablantes, con algún déficit cognitivo. Se analizaron dieciséis estudios publicados durante el período 2001–2012, que mostraron información relevante con respecto a los tamaños de muestra utilizados, los tipos de contrastes estadísticos, los instrumentos de evaluación o diagnóstico, entre otros. Se realizó el estudio siguiendo los procedimientos de estimación habituales, sobre la base de la definición del tamaño del efecto y el análisis de su relación con las variables relevantes (tamaños de muestra, tipo de población, etc.), o variables metodológicas (tipo de investigación o diseño de la muestra, etc.) El análisis de los datos muestra un efecto estadísticamente significativo (r+=.38, p<.001) en todas las variables asociadas a las características de la intervención (duración, tipo de intervención, género, año de publicación y, más importante, la calidad de vida y los resultados neuropsicológicos). Como conclusión general, la dimensión calidad de vida (QoL) puede mejorar, bajo ciertas condiciones, a través de la rehabilitación neuropsicológica, pero este cambio no es permanente.
Health-Related Quality of Life (HRQoL) is a wide concept, but there exists consensus on it being a subjective measure of physical, emotional, and psychological conditions (Londos et al., 2008). Some studies define HRQoL as an assessment of how a disease and its treatment affect a person's capability to develop everyday activities and play valuable roles in their own life (Brissart, Leroy, & Debouverie, 2010; Fergusson et al., 2012). Neuropsychological diseases, like any other diseases, affect the quality of life (QoL) of those who suffer from it (Murell, 1999). In spite of that, the HRQoL of the persons suffering from neuropsychological alterations has not been widely studied, and it is often claimed that rehabilitating treatments in neuropsychological diseases improve the patients’ quality of life without actually measuring HRQoL (Londos et al., 2008). Other works (Cicerone, 2005; Wilde et al., 2010) have recommended using HRQoL measures as outcome measures in order to grade the efficacy of neuropsychological rehabilitation in traumatic brain injury (TBI). Few works have studied the possible impact of neuropsychological interventions on the QoL of patients with cognitive alterations. There exist works on patients with epilepsy, TBI, multiple sclerosis, cardiovascular events, mild cognitive impairment, Alzheimer's disease, and persons on chemotherapy. The methodology used in those works includes pre- and post-treatment observational studies (Cohen, Ylvisaker, Hamilton, Kemp, & Claiman, 2010; Londos et al., 2008; Rasquin et al., 2010), case and control studies (Svendsen &Teasdale, 2006), and several clinical trials (Brenk, Laun, & Haase, 2008; Clare et al., 2010; Davis, Massman, & Doody, 2001; Engelberts et al., 2002; Gehring et al., 2009; Hildebrand et al., 2007; Lincoln et al., 2002; Solari, Pucci, Forni, Mancardi, & Pozzilli, 2004; Voght et al., 2009). Those studies present controversial results: whereas some find a positive effect of neuropsychological rehabilitation on QoL (Brenk et al., 2008; Clare et al., 2010; Cohen et al., 2010; Engelberts et al., 2002; Glanz et al., 2010; Melchers, Maluck, Suhr, Scholten, & Lehmkuhl, 1999; Svendsen & Teasdale, 2006), others do not (Davis et al., 2001). This positive effect on the patients’ quality of life is observable immediately after rehabilitation but is not persistent in follow-up evaluations (Solan et al., 2004). Other works find a positive effect of cognitive rehabilitation on some, but not all, QoL measures (Seniow, Polanowska, Mandat, & Laudanski, 2003; Sitzer, Twamley, & Jeste, 2006). These are understandable controversies given that most works use small samples of patients with different diseases, have different designs, apply neuropsychological interventions of a different nature, duration, intensity, and use diverse instruments to measure HRQoL.
A previous work (Guàrdia, Jarne, Urzúa, & Gudayol, 2012) dealing with the impact of neuropsychological rehabilitation on QoL intended to approach this phenomenon by using meta-analysis techniques while bearing in mind their possible mediating effects in the analysis, as well as other substantive, methodological, and socio-demographic variables which may be affecting the results of the aforementioned works. That study yielded the following conclusions: the positive effect of the rehabilitating intervention is generally linked to an improvement in the patients’ quality of life. Likewise the use of retraining techniques (techniques intended to restore the lost cognitive function) seems to have a positive effect on HRQoL that is more intense than the effect of compensatory techniques (techniques designed to improve specific aspects of everyday life despite the specific cognitive loss experienced by the patient). That positive effect of cognitive rehabilitation on HRQoL tends to decrease as time goes by between the clinical intervention and the follow-up; and when analyzing the data as a whole, each study's sample size and design have a direct influence on the effect size of the QoL improvement. In fact, the above-mentioned work reanalyzes data from Spanish-speaking samples, and as the authors admit, most of the studies included in their study have a pre- post- simple design where the variable control mechanisms are minimal, and they tend to magnify the effect sizes of the phenomenon under study (Ahn, Myers, & Jin, 2012). Moreover the study purposefully excluded the works conducted with non-Spanish-speaking samples, and consequently, it involved relatively few works. On the date of its publication, there existed no other meta-analyses on the subject that allowed the authors to contrast their findings. Therefore their conclusions must be considered preliminary and they should be contrasted with results from non-Spanish-speaking samples, much more common in scientific literature.
Thus, the goal of the present study is to conduct a meta-analysis of the effects of neuropsychological rehabilitation on the QoL of patients with neuropsychological alterations by using non-Spanish-speaking samples, according to the phases proposed by Botella and Gambara (2006). In addition, we intend to compare our results to those of the individual works that approached this topic, and to the results of the meta-analysis by Guàrdia et al. (2012). The differences between, for example, the sample sizes in works with Spanish-speaking samples and those with non-Spanish-speaking samples are so large in most cases that it is impossible to carry out one integrated study with all the papers, with Spanish- or non-Spanish-speaking samples, apart from the fact that the conditions of assistance and neurorehabilitating intervention are not comparable, either.
MethodSearch of studiesTo be included in this meta-analysis, studies had to comply with the following inclusion criteria: a) they had to be original works focused on neuropsychological rehabilitation, that is, assessing the effect of a neurorehabilitation program; b) the studies had to have been published from 2001 to 2012 given that, prior to that period, there exist very few studies and they are much apart in time; c) they had to be indexed in Journal Citation Reports, PsycInfo, Pubmed, Scopus, SciELO, and Latindex; d) the papers had to include at least one psychometric standardized QoL measure; e) the study design had to be recognizable and undoubted in relation to the other variables set forth in this work; f) the studies had to be conducted on non-Spanish-speaking countries; g) the samples had to comprise adults only, samples of children and adolescents were excluded; and h) the studies had to include samples of subjects, case studies were excluded. We also excluded studies according to the following exclusion criteria: a) works where the concept of QoL was not operationalized empirically; and b) the methodological aspects were unclear, that is, neither the design type, nor the measures used, or the statistical contrasts were clearly identifiable. Complementing the above, we would like to specify that we conducted a search based on the Boolean criteria derived from the use of the following key words: Neuropsychological Neurorehabilitation, Clinical Trials, Estimation Clinical Effect Size, Quality of Life.
Also, a manual search was conducted in some psychological or medical bibliographical sources (for example, reports by organizations of renowned prestige such as the World Health Organization or individual universities) hoping to find studies on the subject that had not been registered in the usual bibliographical databases. Studies listed in more than one of the aforementioned sources were not duplicated. This procedure yielded 71 studies within the period at hand. However, a detailed analysis of those led us to discard thirteen papers for using non-psychometric QoL measures, eighteen works for having sample sizes below 30 subjects, sixteen due to the impossibility to estimate the effect size for lack of some relevant data (e.g., sample sizes clearly identified or lack of a statistical contrast estimator), another three because, despite using psychometric registers, they did not use standardized criteria to evaluate QoL, yet four more because they were applied to samples of children or adolescents or were case studies (Seniow et al., 2003), and finally another one which was not obtained within the study period. Therefore, sixteen studies were eventually analyzed (marked with * in the reference section) with a combined total of 2,644 subjects. To validate the paper's selection process, the work was conducted by two independent researchers. The degree of fit was obtained with Cohen's kappa coefficient (k=.84), which, in accordance with Fleis’ criteria (1981), implies a very high agreement.
Coding of the variablesWe considered a series of variables relevant to the majority of studies selected according to the scheme used by Sánchez-Meca, Rosa and Olivares (1999). They were classified as substantive, methodological, or extrinsic characteristics.
We defined the following dependent variables in order to estimate the intervention's effect: a) mean effect size in QoL outcome measures; and b) mean effect size in neuropsychological outcome measures. Below is the list of substantive characteristics registered: a) disease etiology (samples exclusively from TBI, other etiologies (OE) such as Multiple Sclerosis or Alzheimer's Disease, or samples with mixed etiology (ME)); b) neuropsychological intervention (focused on retraining strategies or on compensatory techniques or mixed interventions); c) works with a treatment focused exclusively on neuropsychological interventions (% works); d) months between diagnosis of the illness and neuropsychological treatment; e) intensity of rehabilitation procedures (number of sessions); f) duration of the intervention (number of weeks); and g) ratio between number of sessions and duration in weeks. We selected the following socio-demographic characteristics: a) gender distribution through the studied samples (percentage of women); and b) mean age.
Below is the list for methodological characteristics registered: a) type of study design (clinical trials, one-group designs, or pre- and post-treatment designs); b) measurement procedures for QoL outcomes (psychometric approaches such as the SF-36 or other valid instruments); c) sample size; and d) number of measurement waves.
The extrinsic characteristics analyzed were exclusively the publishing year stratified in four-year periods between 2001 and 2012. In order to assess the reliability of the proposed coding, we studied it on the sixteen selected studies and obtained an interclass correlation coefficient indicating high reliability in the coding (r=.88; p<.001).
Some of the aforementioned variables required previously generating pertinent contingency tables from the original studies. In general, each variable's description was simple and the reconstruction of the table of observed frequencies involved manually calculating the application of a percentage to each sample size in order to obtain the observed frequency (e.g. the number of women treated versus placed in control groups in studies with group designs).
Calculating the effect sizeFirstly, we obtained the estimate of the difference between standardized means for comparison studies between groups or in relation to the baseline measure and the standard difference between the pre- and post-treatment change scores in this type of tests. In some cases, we also reported percentages of improved subjects that were likewise used to estimate the effects of the intervention. In the latter cases, the Odds Ratio estimation was used as described by Rücker, Schwarzer and Carpenter (2008). With all these results, we analyzed the 3×3 table generated by crossing the two main variables: the outcome measures in QoL (psychometric, qualitative, or mixed measures) and the type of treatment (retraining, compensation, or mixed). The data were then corresponded to each variable studied (effect size, sample size, years of diagnosis, etc.) for every possible combination. Therefore all the data tables from the studies were analyzed, and the odds ratio value was obtained for cases where the table presented a 2×2 order, later transformed to a correction value (r). For the remaining tables different from and larger than 3×3, the correlation values were estimated directly, which is usually the general indicator in meta-analysis works. All these analyses were conducted independently by two of the authors of the current paper, with completely matching estimates of the size effect and its corrections.
Data analysisFirstly, r values were corrected by means of their variance to weigh them according to their sample sizes, since the p value related to the effect size is not independent from the sample size where it is estimated. This procedure was repeated following the scheme used by Redondo, Sánchez-Meca and Garrido (2002), with the exception that, in that work, a fixed-effect model was used, and, in our case, we eventually opted for a random-effect model, given the high variability of the observed distributions of the effect sizes. All the analyses were conducted with the IBM-SPSS software, version 21.0, and some of the R software routines (R Development Core Team, 2011), more specifically, the Meta library (Schwarzer, 2013).
ResultsDescription of the resultsFor the sixteen studies analyzed, the mean sample size was 165.25 (SD=11.08) and when combined, the studies yielded a mean age of 56.26 years (SD=9.13). The average time between the diagnosis of the disease and the onset of the cognitive rehabilitation program was 4.12 months (SD=1.11). The average number of sessions was 25 (SD=3.11) (range between 18 and 35). The average duration of the intervention from the onset of the program was 14 weeks (SD=1.94).
Eleven (68.75%) of the studies used a clinical trial methodological strategy, two (12.5%) used case control, and the rest (3 studies) used a simple pre- and post-treatment design with repeated measures. In regard to measurement procedures, fifteen (93.75%) used strategies strictly based on psychometric-base questionnaires and/or scales (SF-36, WHOL, QoFS, etc.) to evaluate the outcome in QoL. No studies used qualitative evaluations by means of semi-structured interviews, and only one (6.25%) used both strategies. As for the publishing year, three studies were published between 2001 and 2003, three between 2004 and 2006, seven between 2007 and 2009, and three between 2010 and 2012. Two studies (12.5%) involved subjects with TBI (strokes caused by traffic and work accidents); eleven focused on individuals with other neuropsychological conditions, such as Multiple Sclerosis, Alzheimer's Disease, and Mild Cognitive Impairment, among others (68.65%). The rest of the studies (3) used subjects suffering from several pathologies. Finally, seven studies (43.75%) focused on retraining strategies, whereas two (12.5%) directed the treatment at compensation systems, and seven (43.75%) set forth mixed rehabilitation procedures (both retraining and compensation mechanisms).
Finally, we would like to point out that the assessment of statistical and methodological quality (scale 1 to 7, 1 for a low evaluation, and 7 for and excellent evaluation)—conducted by four independent experts (coefficient of concordance of .94)—of the selected works yielded a mean of 5.77 (SD=0.91), which would indicate a not especially high methodological and statistical test in the complexity of the designs and statistical treatments set forth. These types of estimations are of little relevance, but they offer an approximate idea of the complexity of the strategies used and are frequent in studies on meta-analyses.
Mean effect sizeAfter obtaining the effect sizes based on correlation, the observed global mean was r+=.38, which points at a highly significant effect (p<.001). These results are important because the obtained signification shows a high effect size. In order to establish better these results, the Binomial Effect Size Display (BESD) was applied (Rosenthal & Rubin, 1982; Valera-Espín & Sánchez-Meca, 1997). The BESD estimated values obtained for the treatment groups were of 60.28% and obviously of 39.72% for the failure. This high percentage warrants the significance of the results in the statistical and clinical domain. The analysis of the contingency tables indeed shows a clear tendency toward the use of intervention systems based on retraining by means of simple designs of pre- and post-test repeated measures. That is consistent with the data of previous meta-analyses conducted with English-speaking samples. As stated by Sitzer et al. (2006), this would be expected in clinical trials applied in hospitals and is consistent with works similar to the present one, such as Cicerone (2005).
Moderating variablesThe initial analysis with the direct effect sizes show clear statistical significance (QT(15) = 97.42; p<.001), so we can assume the heterogeneity of the effect sizes derived from the different studies. Therefore, the need arises to evaluate the role of the different moderating variables identified in this study in order to search for reasonable explanations for that difference both in the boarding system and in the mechanisms of intervention. The mean effect size is good complementary information. Accordingly, the meta-analytical approach here presented may provide us with more thorough data than merely checking the published works, which is the usual methodology in scientific literature reviews.
Therefore, the descriptive effect in favor of retraining strategies versus compensation strategies—discussed in the next section—must be clarified according to the role of the moderating variables we have determined, since it is reasonable that some of them may provide relevant information regarding the differences we found. The tables below show the statistical significance found for qualitative variables (Table 1) and for quantitative variables (Table 2).
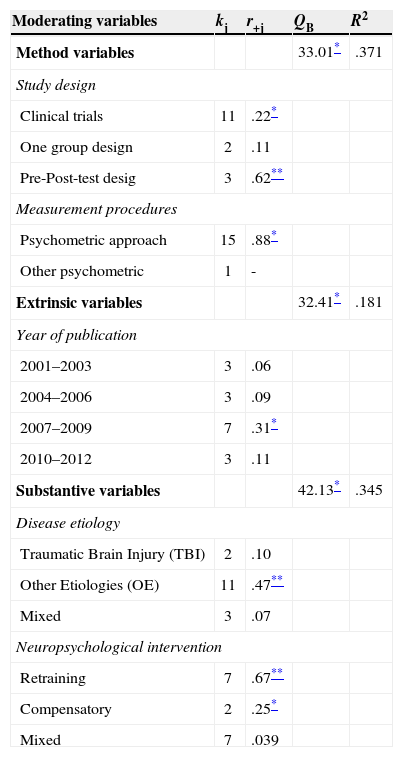
Results of the variance analyses for the qualitative moderating variables.
| Moderating variables | kj | r+j | QB | R2 |
|---|---|---|---|---|
| Method variables | 33.01* | .371 | ||
| Study design | ||||
| Clinical trials | 11 | .22* | ||
| One group design | 2 | .11 | ||
| Pre-Post-test desig | 3 | .62** | ||
| Measurement procedures | ||||
| Psychometric approach | 15 | .88* | ||
| Other psychometric | 1 | - | ||
| Extrinsic variables | 32.41* | .181 | ||
| Year of publication | ||||
| 2001–2003 | 3 | .06 | ||
| 2004–2006 | 3 | .09 | ||
| 2007–2009 | 7 | .31* | ||
| 2010–2012 | 3 | .11 | ||
| Substantive variables | 42.13* | .345 | ||
| Disease etiology | ||||
| Traumatic Brain Injury (TBI) | 2 | .10 | ||
| Other Etiologies (OE) | 11 | .47** | ||
| Mixed | 3 | .07 | ||
| Neuropsychological intervention | ||||
| Retraining | 7 | .67** | ||
| Compensatory | 2 | .25* | ||
| Mixed | 7 | .039 | ||
Note. k = Numberof studies for each category; r+j = mean of the correlation coefficient; Qb = statistical signification test; R2 determination coefficient.
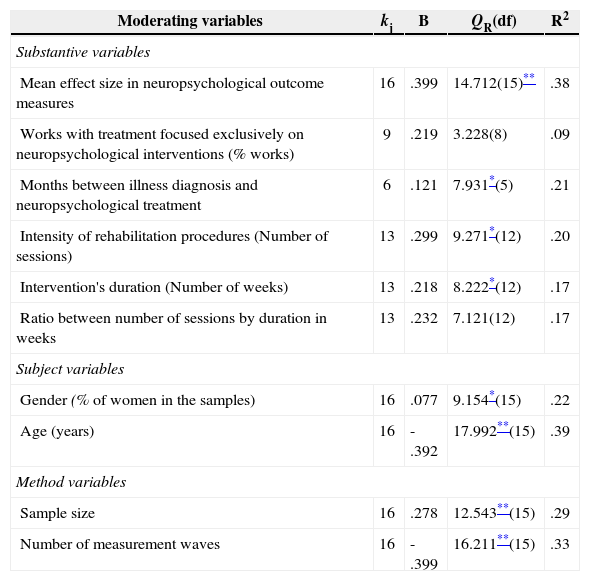
Results of the weighted simple regression analyses for the quantitative moderating variables.
| Moderating variables | kj | B | QR(df) | R2 |
|---|---|---|---|---|
| Substantive variables | ||||
| Mean effect size in neuropsychological outcome measures | 16 | .399 | 14.712(15)** | .38 |
| Works with treatment focused exclusively on neuropsychological interventions (% works) | 9 | .219 | 3.228(8) | .09 |
| Months between illness diagnosis and neuropsychological treatment | 6 | .121 | 7.931*(5) | .21 |
| Intensity of rehabilitation procedures (Number of sessions) | 13 | .299 | 9.271*(12) | .20 |
| Intervention's duration (Number of weeks) | 13 | .218 | 8.222*(12) | .17 |
| Ratio between number of sessions by duration in weeks | 13 | .232 | 7.121(12) | .17 |
| Subject variables | ||||
| Gender (% of women in the samples) | 16 | .077 | 9.154*(15) | .22 |
| Age (years) | 16 | -.392 | 17.992**(15) | .39 |
| Method variables | ||||
| Sample size | 16 | .278 | 12.543**(15) | .29 |
| Number of measurement waves | 16 | -.399 | 16.211**(15) | .33 |
Note. k = number of studies; B = is the non-standardized regression coefficient; Qr = statistical signification test for each regression coefficient; R2 = the determination coefficient.
Statistically significant data in both tables present a relatively clear scenario. First, regarding Table 1, we see that (QB(2)= 33.01; p<.05), so we can infer that this type of works use pre- and post-test designs with repeated measures without much of a doubt about that effect (r+=.62), as compared to those using clinical trials (r+=.22) or case control strategies (r+=11). In relation to the measurement procedures, the use of scales is the only significant source (r+=.88) and it allows us to infer that the scientific community widely agrees on this point and that both effects are important, given that R2=.371 (37.1% of explained variance), which should not be discarded. In fact, the effect of using psychometric scales for both pre- and post-test evaluations is decisive.
Likewise, the papers published within the 2007–2009 period (r+=.31) show a tendency toward a somewhat higher average effect size (QB(3) = 32.41; p<.05), so it would be reasonable to think that over time the number of studies has increased, and the studies have become clearer with more significant effect sizes (18.1% of explained variance). In other words, in two years there has not only been a clear breakthrough in the number of studies published with non-Spanish-speaking samples.
We would like to point out that the estimated effect is distributed asymmetrically among the studies using samples of patients with external or internal pathologies according to the definition above. External pathologies (r+=.10) were not statistically significant, but internal pathologies (r+=.47) were clearly significant instead (p<.01). The effect of samples with both pathologies has been discarded due to non-significance (r+=.07). Finally, the combined effect derived from retraining interventions was highly statistically significant (r+=.67; p<.01), as was the effect associated to the compensatory intervention (r+=.25; p<.05). Despite being statistically significant, they are far from the effect obtained by retraining interventions. Probably, that effect is partly due to the different tradition in the clinical studies applied to the one we discussed above, which focused on retraining as a choice of intervention in relatively simple designs. No associated effect to the mixed strategy was noted (r+=.039). In general, the explained variance was high (R2=.345 or 34.5% of the total) and statistically significant (QB(2) = 42.13; p<.05).
If we focus on Table 2, regression models show some effects to be highlighted. The percentage of works focusing solely on neuropsychological interventions (QR(8) = 3.228) was not significant. Instead, the months gone by from the diagnosis to the onset of the intervention (QR(5) = 7.931; p<.05), and the number of sessions (QR(12) = 9.271; p<.05) applied were significant. The duration of the intervention program was statistically significant (QR(12) = 8.222; p<.05), therefore it seems that longer rehabilitation programs bring more effect to the therapy results. Likewise, although there was no clear statistical significance (QR(12) = 7.121), a tendency can be established toward ratio significance between weekly sessions and the number of weeks of the program. This adds to the notion that a greater effect is obtained in programs involving more sessions during a longer period of time.
The crucial data in Table 2 are the results obtained with the data derived from the outcome in neuropsychological performance. The result is highly significant (QR(15) = 14.712; p<.01) for neuropsychological measures, exclusively. Thus, we can interpret that the studies analyzed show that cognitive rehabilitation programs are effective with an effect size that may be responsible for up to 38% of the explained variation, and, even more importantly, that effect is more intense when they are estimated by comparing the pre- and post- levels of these patients’ perceived QoL, up to 39% of the explained variation. There are no differences between one choice and the other, but it is important to highlight a certain tendency to improve neuropsychological values over strictly QoL measures.
These comments need to be clarified, partially, by the role of the subject and the methodological variables included in Table 2. There is, indeed, an evident bias in favor of women and younger patients. In the case of women, the effect is clear (QR(15) = 9.154; p<.05), and even more conclusive in the mean age of the groups treated (QR(15) = 17.992; p<.01). It should all be interpreted in the sense that the favorable effect in post-evaluations is more pronounced in the case of women and younger subjects (the coefficient of regression is negative, (β = −.392). Likewise, the effect attributed to the study of sample sizes and the number of measurements is also crucial. As regards the sample size, the results we obtained (QR(15) = 12.543; p<.01) show that the effect size is higher and clearer with large samples. It is also important to note that the effect of the duration of the follow-ups (measurement waves) is also clearly significant (QR(15) = 16.211; p<.01). The negative value of the coefficient of regression (β = −.399) would show that, as the follow-up duration increases, the effect size decreases. The reduction of post- effects is clear, as they seem to dilute over time. Both variables are essential given the variation percentages they explain: 29% and 33% respectively. Finally, in order to evaluate the possible bias of publication, we estimated the Egger test (Egger, Smith, Schneider, & Minder, 1997), which was non-significant (p=.86). Therefore it was unnecessary to include information of the Funnel plot.
DiscussionThe results allow us to draw several conclusions. Firstly, it is important to highlight that the number of papers with non-Spanish-speaking samples analyzed (16) was lower than the number of papers with Spanish-speaking samples (21) reported on Guàrdia et al. (2012), since the publications in non-Spanish-speaking countries vastly outnumber any others. The reason may lie in the fact that this type of works commonly use clinical samples, and intervention times are glaringly longer in Spanish-speaking healthcares than in non-Spanish-speaking ones. Additionally, in the Spanish-speaking world, it is somewhat more common to use Quality of Life measurements as indicators of effect associated to the neurorehabilitation program. The tradition in the Spanish-speaking neuropsychological approach is somewhat longer than in the non-Spanish-speaking one.
Furthermore, we must note the existence of a positive effect of neuropsychological rehabilitation techniques on QoL. We can thus state that the different neuropsychological intervention therapies improve the patients’ quality of life, with a moderate effect size. However, that effect tends to decrease over time. As time goes by after the neuropsychological intervention applied, the patient's quality of life tends to diminish, which suggests that the therapy's positive effect on the variable is not permanent. In addition, the rehabilitation's effect on QoL is very much influenced by several moderating variables, both quantitative and qualitative. As for the effect of the substantive variables, we must note that the type of therapy applied seems to influence the phenomenon under study, so that those works where the neuropsychological intervention was based on the use of retraining techniques are the ones showing the greatest improvements in their patients’ quality of life, whereas those using compensatory treatment strategies yield more modest results. However, that fact can be due, at least partly, to the slightly higher number of participants in that sub-sample than in other intervention groups, which is hardly surprising when we consider that those techniques have a greater tradition in neuropsychological intervention. For that reason, this fact could be biasing the results, thus yielding a greater effect size than other interventions. Other substantive variables interfering with the neuropsychological rehabilitation's effect on QoL are all those related to the intensity and the duration of the interventions. If we increase the weeks of duration of the intervention, the number of sessions of the intervention, and the relationship between the number of sessions and the duration of the intervention in weeks, then the effects on QoL increase, too. Nevertheless, those variables must be understood within the patients’ clinical context, since they are often determined by the conditions of the health services. The neuropsychological deficit's etiology is another substantive variable seeming to influence the effects of rehabilitation on QoL. Accordingly, neuropsychological interventions do not seem to bear a positive effect on QoL in persons who suffered from traumatic brain injury, but instead they do on patients with cognitive alterations due to other etiologies. The patients’ age also had an important mediating effect. Younger persons seem to obtain greater increases in their QoL after rehabilitation.
With regard to the method's variables, the works using a clinical trial classic methodology obtained greater increases in QoL after clinical interventions than the studies using a pre-test post-test methodology and the case and control studies, since in the latter the rehabilitation bore no significant effect on QoL. However, most of the studies included in the present meta-analysis used the clinical trial methodology, for which reason the number of patients included in this sub-sample is much larger than in the other two, which could bias the statistical effects found in this work. As for the extrinsic variables, the year of publication influences the effect size of post-intervention QoL. Accordingly, it is highest in the group of papers published between 2007 and 2009. Yet again, the number of works published in this period is higher than in the other periods studied, with a greater accumulated sample size, which entails a possible bias effect on the estimated effect size.
When comparing the results of the present works to those of Spanish-speaking samples (Guàrdia et al., 2012), we must highlight the following conclusions. Both present important differences as regards the results obtained. The present paper has a higher total sample size than the Spanish-speaking samples and comprises originals with a higher average number of participants. Likewise, among the studies included in this meta-analysis, there are more of them using a clinical trial methodology and, in general, from the methodological point of view, i.e., the originals included in this meta-analysis have a higher methodological quality than those included in Guàrdia et al. (2012). Important differences also exist between them regarding several substantive variables that have an important mediating effect on QoL. Therefore, in the present work, the duration and the intensity of neuropsychological interventions were higher than in Guàrdia et al. (2012). The patients’ average age in this study is lower than in the study with Spanish-speaking samples, and the time elapsed between the onset of the disease and the administration of neuropsychological treatment is shorter in this paper than in Guàrdia et al. (2012). Likewise, important differences exist between both meta-analyses regarding the type of treatment administered. In both works, a significant proportion of the patients were treated using only retraining techniques, but in the study with Spanish-speaking samples, a great number of patients were treated only with compensatory techniques, and very few were treated with a combination of both techniques. In contrast, in the present study, the opposite tendency was observed. More patients were treated with a combination of techniques than with compensatory strategies only.
Even more significant are the differences between both studies as regards substantive variables such as the patients’ age, the time elapsed between the onset of the disease and the treatment, or its intensity. We must point out that such variables usually affect the neuropsychological treatment's outcome (Niemeier, Kreutzer, Marwitz, Gary, & Ketchum, 2011), for which reason it might also be expected that they should have a direct effect on the patients’ quality of life. Despite all these differences, the general conclusions of the present work agree with those of Guàrdia et al. (2012). In both cases, we can conclude that neuropsychological rehabilitation has a positive effect on HRQoL, with a moderate effect size. However, as the follow-up time goes by, the effects of neuropsychological rehabilitation tend to diminish and even disappear. Therefore, both studies also agree on this change seemingly not being permanent. The fact that the central conclusion of both meta-analyses agrees on substantive variables is important, given that it favors the idea that our interpretation of the data is correct and, therefore, our conclusions are accurate. Our study presents an important limitation, which is that it was not possible to analyze the mediating effect of such variables as the severity of the pathology or the patient's socio-economic context. These are variables which, as is known, influence the outcome of the neuropsychological rehabilitation (Arango, 2012), they could affect QoL, and they are indeed part of that construct (Mayo, Moriello, Asano, Van der Spuy, & Finch, 2011). This is because the works considered here have not involved analyzable data in relation to those variables. Leaving aside the latter consideration, the consonance between the results obtained in both populations allow us to guarantee a clear line in the effects found, as well as serious limitations in the effect's perdurability.
Conflicts of interestThe authors declare that they have no conflicts of interest.
This research was made possible by the PSI2010-21214-C02-01 project and was carried out by members of the Generalitat de Catalunya's SGR 388 Consolidated Research Group.
