





Polycystic ovary syndrome is one of the main causes of infertility in women. It occurs in 4–10% of the female population of childbearing age, its main symptoms being pain during the menstrual cycle and its prolongation, as well as abnormal growth of body hair. The case of a 22-year-oldpatient with 7 follicular cysts in each ovary is presented. She is treated with acupuncture in combination with percutaneous electrical stimulation, resulting in relief of symptoms, as well as a decrease in the size of follicular cysts.
El síndrome del ovario poliquístico es una de las causas principales de infertilidad en las mujeres. Se produce en el 4 al 10% de la población femenina en edad fértil, siendo sus síntomas principales el dolor durante el ciclo menstrual y su prolongación, así como el crecimiento anormal del vello corporal. Presentamos el caso de una mujer de 22 años de edad con 7 quistes foliculares en cada ovario. Fue tratada con una combinación de acupuntura y estimulación eléctrica percutánea, que se tradujo en un alivio de los síntomas y una reducción del tamaño de los quistes foliculares.
The polycystic ovary syndrome (POS) is a multifactorial distress, this public health issue affects to the female population in childbearing age and reproductive, it's estimated to imply a high cost to the health system, being the most common motives of consult, infertility characterized for chronic hyper androgenic anovulation which leads to an ovarian dysfunction, acne, menstrual disorders, obesity and hirsutism.2–5,26–28
The POS diagnosis is based in the presence of two of the following three criteria: alterations or menstrual irregularities (amenorrhea, oligo menorrhea), clinic hyper androgenism (hirsutism, virilism or both), biochemical (free testosterone, androstenedione and dehydroepiandrostenedione for its acronym DHEA), just like ultrasound findings at least one of the two ovaries with a volume over to 10 cm2 and/or present twelve or more follicles from 2 to 9 mm of diameter; other clinical demonstrations of higher relevance are: acne, obesity, increase of the abdominal perimeter, complications in pregnancy (recurrent abortion, gestational diabetes, and preeclampsia), increase of cardiovascular risk, hyper prolactinemia, alopecia, acanthosis nigricans, hyper insulemnia, sleep disorders, and neuropsychiatric syndromes.1,2,4,6,7–9,11,21,24
Inside the possible causes of the POS relations with anxiety disorders and depression, are associated with high levels of DHEA, and a kind of androgen hormone (however more studies are needed about it), and low serotonin levels, so they are more susceptible to anxiety, stress or depression, which goes from moderate to severe cases.8,10–12
In the differential diagnose we can find an androgen-secreting tumor, external administration of androgen, chusting syndrome, non-classic congenital adrenal hyper plasia, acromegaly, genetic defects of the insulin action, primary ovarian failure, thyroid disease.12
The POS affects form 4–10% of the female population in childbearing age, however each time the age range is decreasing, since it's been presented cases of POS in 24% of girls between 3 and 18 years. The prevalence of early puberty in women has a higher index than in men. This last has an estimated risk of 1–400, the excessive sexual hormone production causes a decrease in the gonadotropins production, diagnosed regularly, autonomous ovary follicular cysts in these girls, same which when growing in size, increase the estrogen production leading to the early mammal develop, bleeding of vaginal fluid, and/or increase in the labia minora.14–16,21
This is a public health issue, since it represents a high cost and decreases notably the women quality life, this without mentioning the consequences that his disorder can condition in a future, higher prevalence of having diabetes, ovary cancer, uterus cancer, mammal cancer, dyslipidemias, cardiovascular problems.3,13
It's been proven that an integral treatment which considers changes in the patient lifestyle, as well as weight loss, diet, exercise, pharmacological therapy, surgical, and complementary therapy generate a positive effect. Acupuncture helps to regulate and manage menstrual periods, also it contributes in the weight loss, headache and improves the mood, this thanks to the endogenous opioid release, and the influence it exerts in the acupunctural stimulation in the autonomous nervous system, peripheral and central, favoring the activation of the hypothalamic–pituitary-adrenocortical axis.2,13,17–20,25,29–32
Clinical case descriptionFemale patient of 22 years old, comes to acupuncture consultation with previous diagnosis of ovarian follicular cyst with 2 years of evolution, presents oligomenorrhea cycles of 45–60 days in the last year, hypomenorrhea with pink-orange coloration and presence of clots in the last 6 months, intense cramps ENA 8–10 in the right and left iliac fossa radiating to the hypogastrium one day before and the first 2 days of menstruation, she adds frequent episodic tension headache predominantly in the frontoparietal area, every day, polydipsia, dysphoria with a feeling of wanting to cry all the time and hyperphagia. On physical examination hyperandrogenism present, moderate hirsutism (24 points on the Ferriman and Gallwey scale), acne on the back, T-zone of the face and slightly on the chest grade 1 in EGAE, on deep palpation in the left iliac fossa presence of a slight fixed lump the size of a chickpea 0.5 cm approximately, with slight discomfort (ENA 3–10.) A gynecological pelvic ultrasound and female hormonal profile were performed.
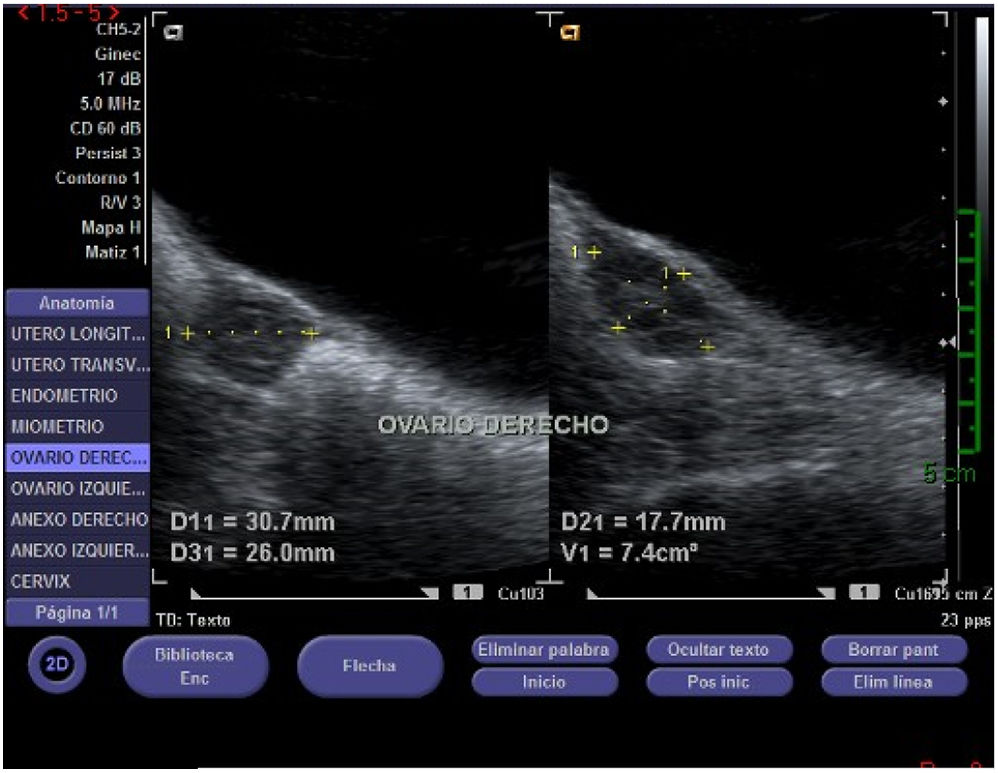
The female hormonal profile showed clinical data within normal parameters, on the other hand in the transabdominal pelvic ultrasound can be visualized 7 follicular images in each ovary between 0.3 and 0.7 cm (Fig. 1).

Ultrasonography was performed to support the results of the treatment with acupuncture and percutaneous electrical stimulation.
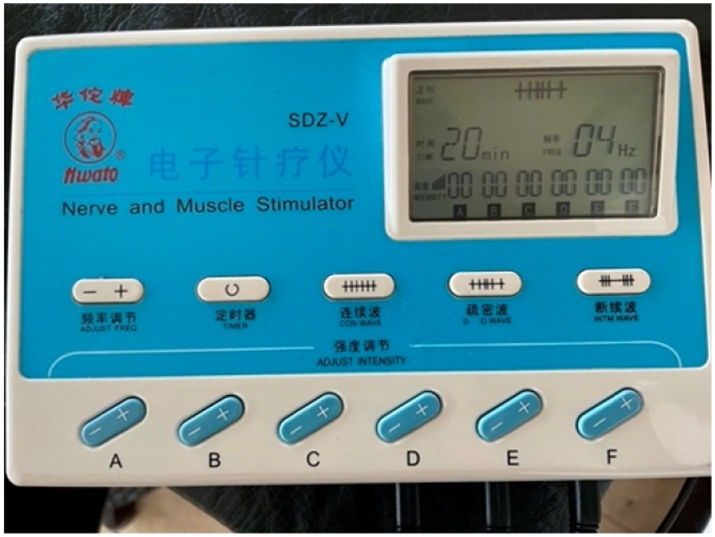
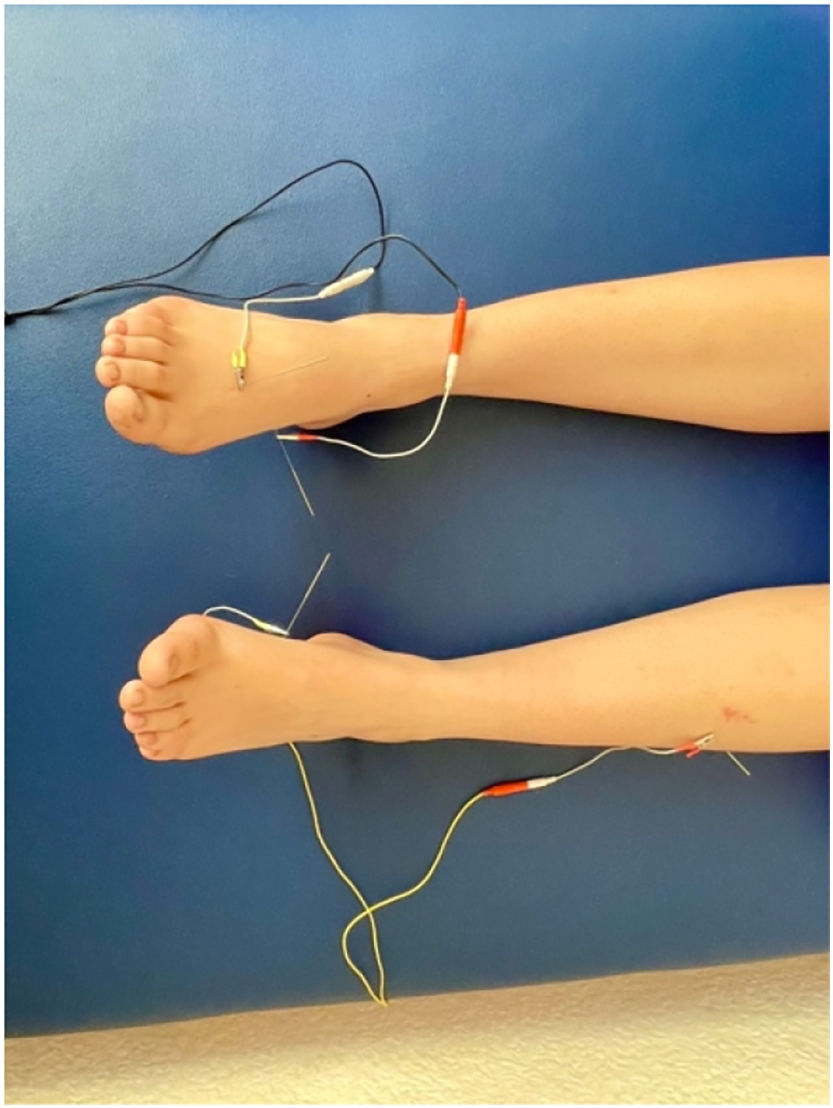
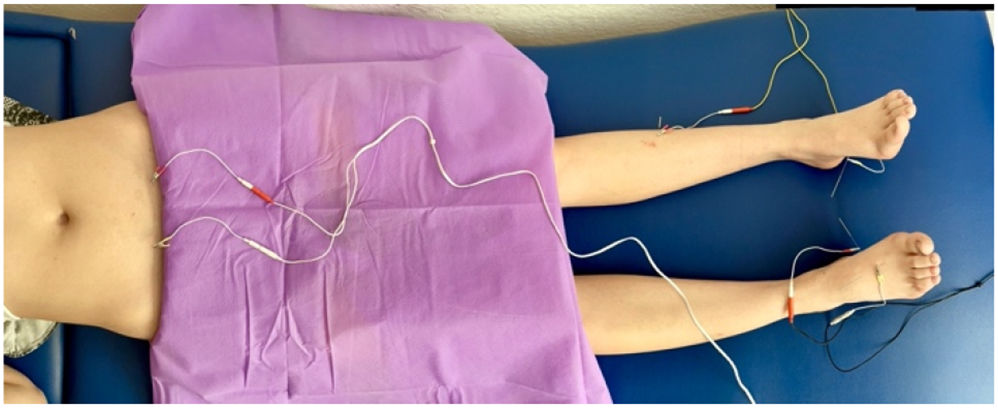
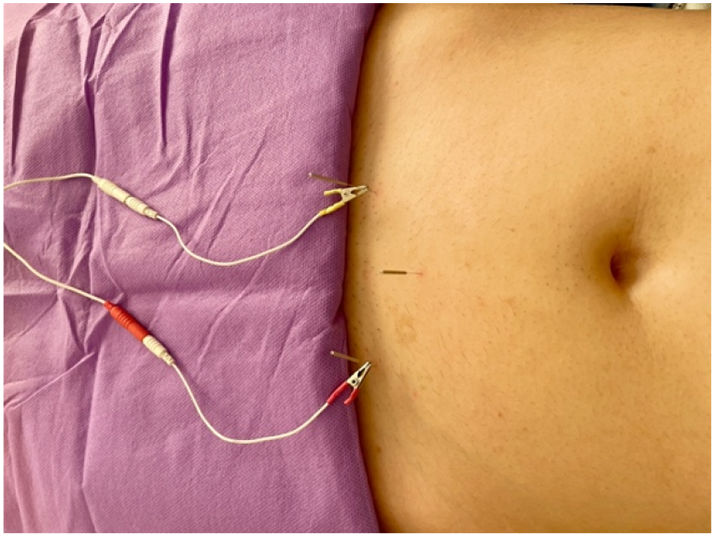
The points B4 gongsun and Pc 6 neiguan bilateral were used to open the Chong mai channel, H3 Taichong unilateral alternating in each session, E40 fenglong unilateral alternating in each session, RM 4 guanyuan, E29 Guilai bilateral and DM26 Renzhong, with percutaneous electrostimulation, asymmetric biphasic current, with a pulse width of 80 microseconds for a sensitive effect, and a frequency of 4 HZ (Fig. 1) connecting the points B4 gongsun with E40 fenglong (Fig. 2), B4 gongsun and H3 Taichong (Fig. 2), E29 guilai bilateral (Figs. 3, 4). The treatment implemented was 10 sessions, two per week with a duration of 20 min each, repeating the protocol.



The following results were obtained:
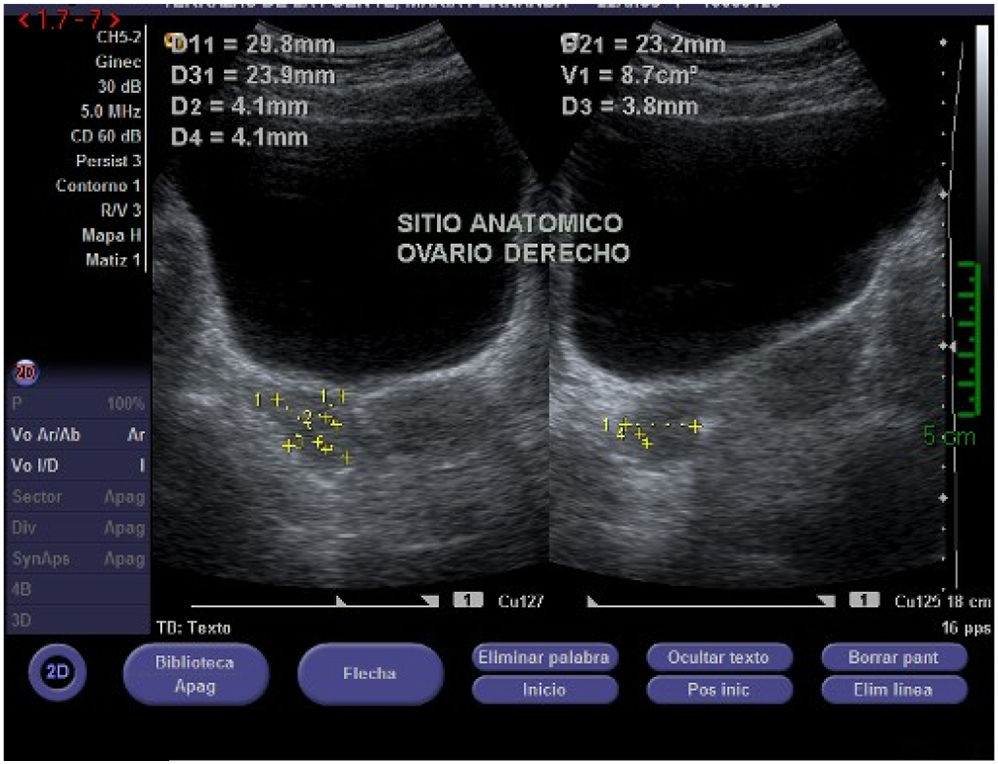
Table 1 shows the results of the evolution of ultrasound in the right ovary, in Fig. 5 show the results of the first ultrasound performed before treatment, in Fig. 6 ultrasound taken at 5 sessions, and the Fig. 7 the final results of treatment.
Evolution of ultrasound values of the right ovary (figs. 5,6,7).



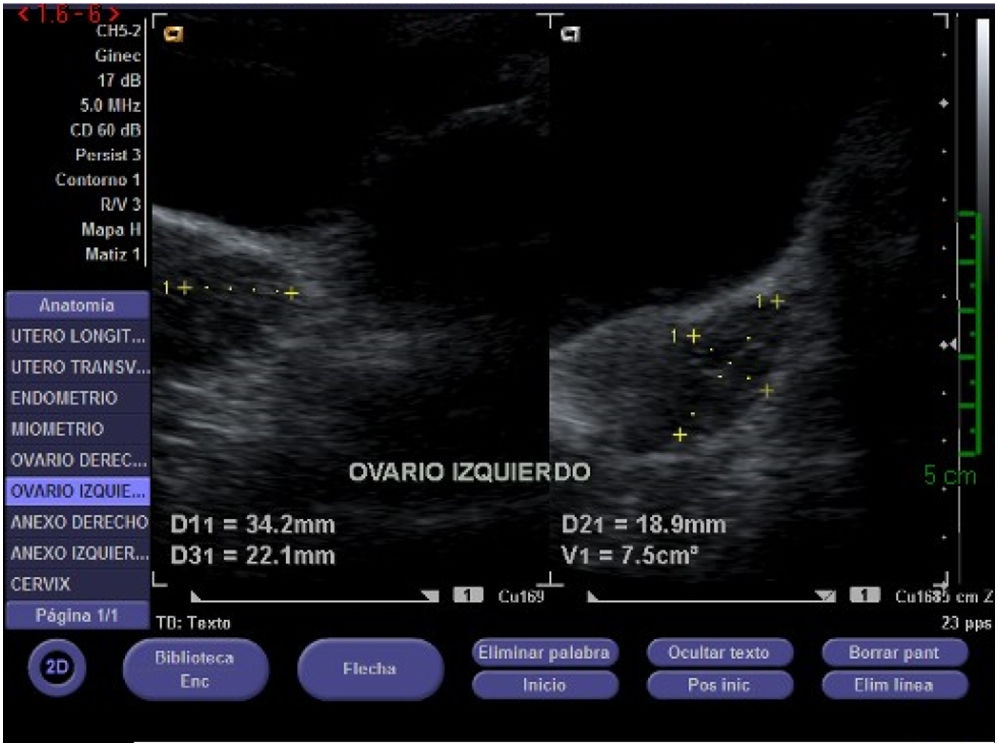
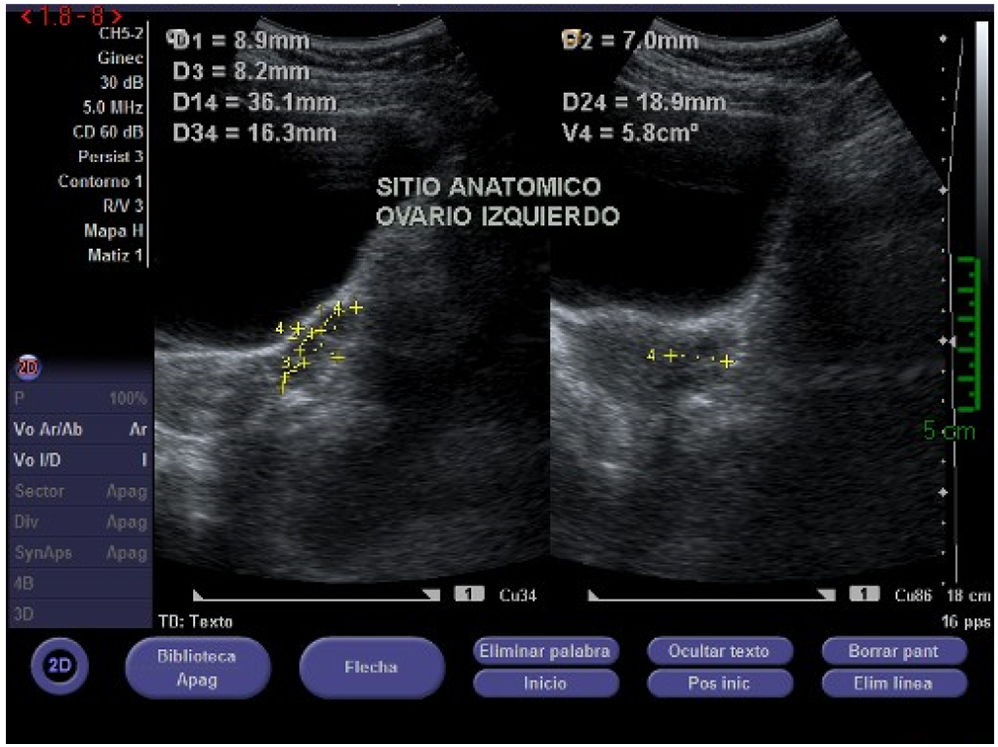
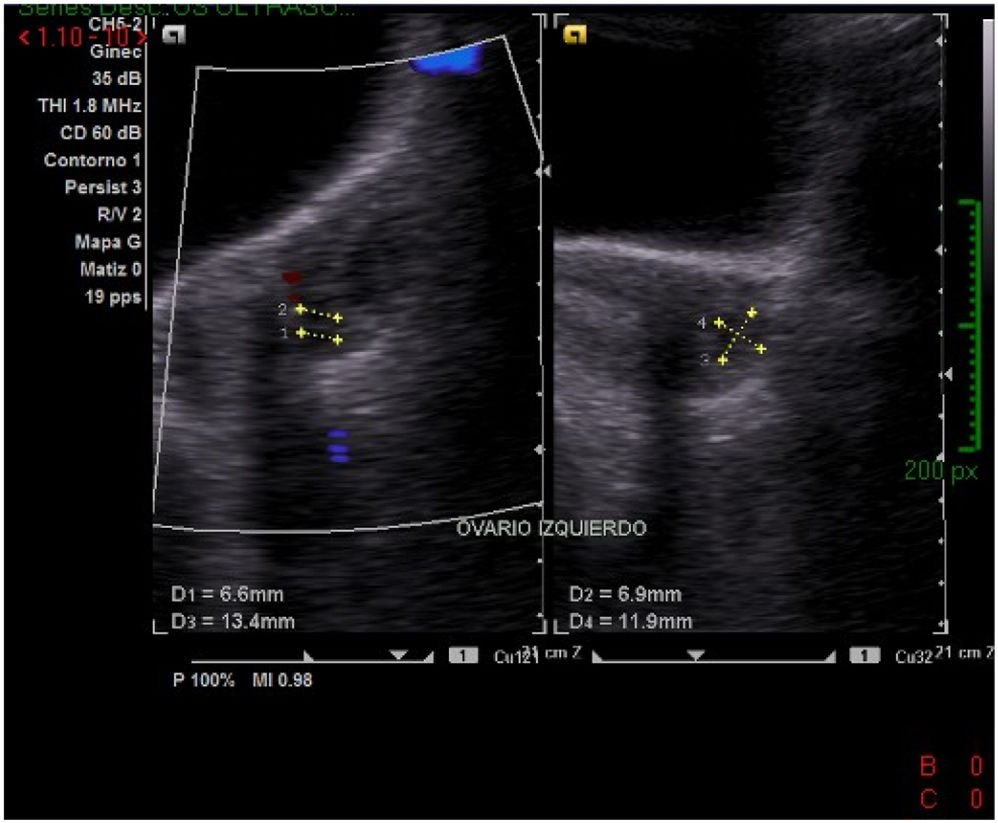
Table 2 shows the results of the evolution of ultrasound in the left ovary, Fig. 8 before treatment, Fig. 9 taken at 5 sessions and Fig. 10 the final results of treatment.
Evolution of ultrasound values of the left ovary (figs. 8,9,10).
| Month | Dimension | Quantity | Size |
|---|---|---|---|
| NOVEMBER 15/ 2021(Fig. 8) | 3.4 × 2.2 × 1.8 cm | 7 | 7 with dimensions between 0.3 and 0.7 cm |
| NOVEMBER 29/ 2021(Fig. 9) | 3.6 × 1.8 × 1.6 cm | 7 | 7 with dimensions between 0.7 and 0.8 cm |
| DECEMBER 16/ 2021 (Fig. 10) | 4.13 × 2.5 × 2.44 cm | 4 | 4 with dimensions between 0.66 and 0.69 cm, a larger cyst can be visualized 1.34 × 1.11 cm |



According to the table we have that in the right ovary, a reduction in the size of the cysts was achieved up to 50% (Figs. 5,7).
In the right ovary, the size was reduced from 25% to 50%, but not the number of cysts, while in the left ovary the size was reduced from 5.75% to 13.75% and it should be noted that only 4 cysts appeared (Figs. 8,10), therefore 3 of them disappeared, it is worth mentioning that only one of them increased its size by 67.5%. In addition to this, a reduction in the menstrual cycle time was achieved, starting with 45–60 days, to an average cycle of 33 days, from the second menstrual cycle, during the 28th day, the presence of light brown spots could be noticed. The permanence of the cycle was 5 days, the color of the flow from brown to bright red, the patient reported noticing a decrease in the amount of clots. As for menstrual cramps the pain decreased significantly to 5–10 ENA, the frequent episodic tension headache has only appeared on 3 occasions in the last 2 months, which proves that acupuncture can be a great ally in the regulation of the cycle and symptomatology, without presenting negative side effects.
DiscussionConventional treatment for polycystic ovary syndrome is multifactorial and aims to reduce symptoms, improve ovarian function by reducing androgen action.1,2,15,16,22,27,28
Pharmacological treatment should consider reproductive aspects with or without the desire to conceive. Clomiphene citrate, selective aromatase inhibitors, such as anastrozole and letrozole, are used as ovulation inducers; however, ovarian hyperstimulation syndrome, multiple pregnancies, hot flashes and gastric symptoms have been reported as side effects.2,3,22,23,28
On the other hand, contraceptive pills with ethinestradiol and progestin are the most commonly used in patients who do not wish to conceive, although there is still controversy as to the length of time they can be used.2,3
In the figures corresponding to the pelvic ultrasound performed on the patient, a notorious change in the size of the follicular images in the right ovary can be visualized.
By implementing acupuncture combined with percutaneous electrical stimulation, a considerable improvement was obtained in the quantity, duration and frequency of menstrual bleeding, as well as pain during menstrual bleeding. The frequency of tension headache decreased, the patient's mood improved and, as demonstrated by ultrasound, the size and number of follicular cysts decreased.
Ethical considerationsThe informed consent of the patient was obtained in writing, for the publication of this article.