




A 46 year-old male presented suffering from refractory erectile dysfunction. The patient had a past history of pelvic chondro-sarcoma. This case was a challenge for us; the surgery performed for excision of the sarcoma has resulted in the elimination of both pubic ramia together with excision of part of both corpora and left hemiscrotum. The procedure included a sling application on one side with a mesh sock wrapped around the rear part of the extendor cylinder. Another sling was applied on the contra lateral side without a mesh sock.
Varón de 46 años que presenta el sufrimiento por disfunción eréctil refractaria. El paciente tenía antecedentes de condro sarcoma pélvico. Este caso fue un reto para nosotros; la cirugía realizada para la extirpación del sarcoma ha dado como resultado la eliminación de ambas ramas púbicas junto con la extirpación de parte de ambos corpus y hemisrcotum izquierdo. El procedimiento incluyó una aplicación de eslinga en uno de los lados con una funda de malla envolviendo la parte trasera del cilindro extensor. Se aplicó otra eslinga en el lado contra lateral sin una funda de malla.
Chondrosarcoma is the second most common malignant tumor of bone. It is characterized by tumor cells producing cartilage matrix. The estimated incidence of chondrosarcoma is 1 in 200,000 per year.1 A variety of histological types with diverse clinical behavior have been described, with conventional types being the most common. The sites of predilection of the skeleton are pelvis, femur and proximal humerus.2 Survival in chondrosarcoma has remained unchanged over the last 30 years with no significant improvement as emphasized in Surveillance, Epidemiology, and End Results (SEER) database study.1 Chondrosarcoma of axial skeleton revealed poorer oncologic outcomes than appendicular skeleton.1,3,4Guder et al. (2015) had shown that a wide tumor resection is essential in the therapy of primary malignant bone tumors to minimize the risk of local recurrence and ensure long-term survival particularly in chondrosarcoma.5
Case reportWe are hereby to present this 46 year-old male, known to have multiple hereditary exostosis, a genetic disorder characterized by multiple bone osteochondromata. One of them started to enlarge progressively. The patient also suffered from difficulties in urination and pain with erection as result of this mass. He sought medical advice for his condition. An x ray and MRI were done for him (Fig. 1). His condition necessitated wide bone and soft tissue resection. The patient was admitted on to Kasr Al-Ainy Hospital, the Orthopedic Department, Cairo University on the 20th April 2015.

The surgical approach was extraperitoneal and is detailed as follow, an ilioinguinal incision was done with both abdominus recti diverted, and the bladder was protected. Both pubic rami of adductors were released. Bony excions were done including symphysis pubis, superior and inferior pubi rami on both sides. The whole symphysis and both pubic rami were resected. The tumor was, also, adherent to both corpora cavernosa which necessitated excision of part of the corpora on both sides. Histopathology revealed chondrosarcoma on top of exostosis.
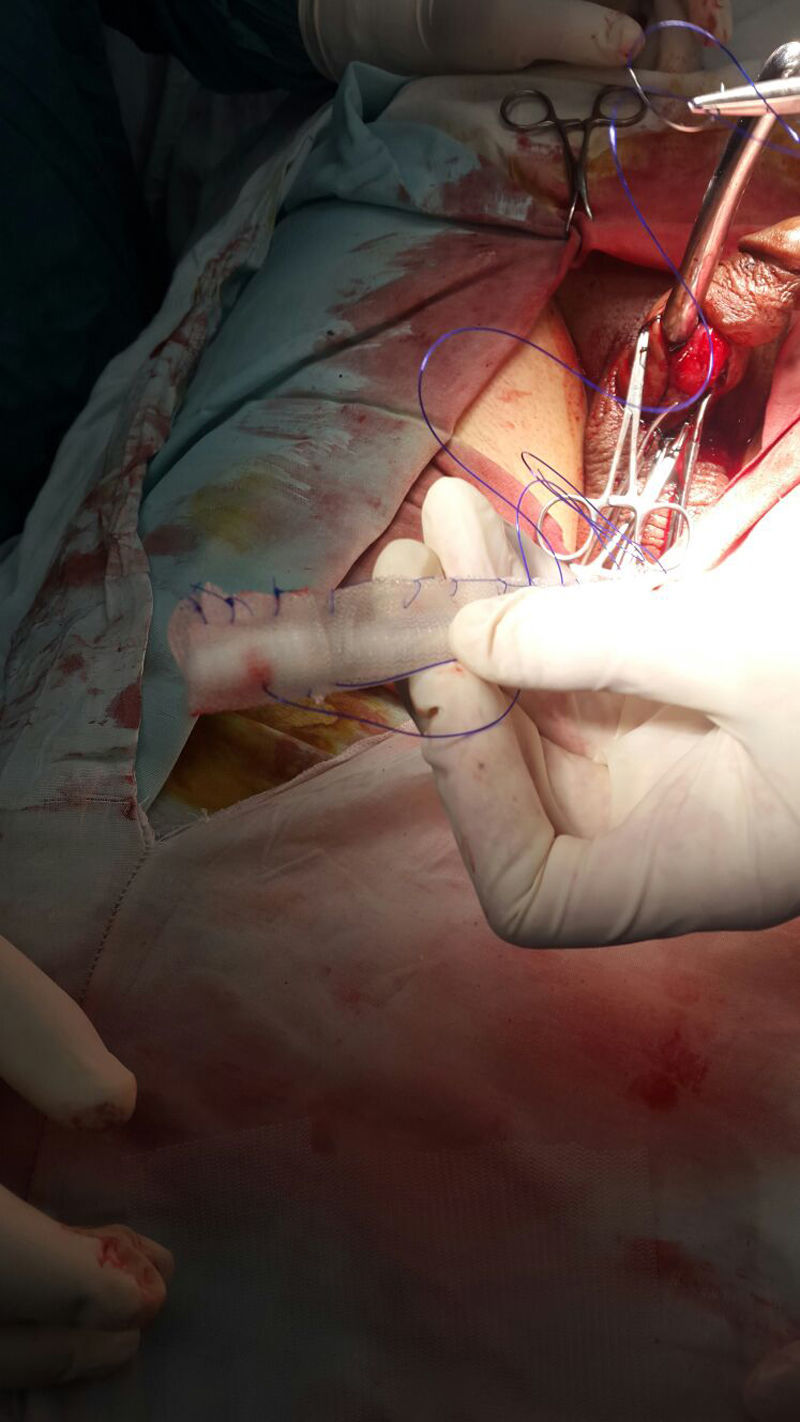
DiscussionThe case was challenging because of the distorted surgical anatomy of this patient following extensive bone and soft tissue excision. The X-ray before penile prosthesis showed absence of ischial tuberosities on both sides. The Shortened corpora made the implant vulnerable to posterior perforation during sexual intercourse making the choice of inserting hydraulic implant impossible. Additionally, post-operative instruction to the patient so as not to lift heavy objects and to wear scrotal suspensory in the absence of the left hemiscrotum made the insertion of the pump impossible as it would induce pressure on the pelvis. The patient underwent the operation on 7/2/2016 at the Andrology Surgical Unit, Kasr Al-Ainy Hospital, Faculty of medicine, Cairo University. In the surgical procedure, we used TUBE malleable semi rigid penile implant (Promedon). The approach was penoscrotal incision followed by dissection of buck's fascia and finally a corporotomy incision 4cm long to facilitate insertion of both rods. The length of both cylinders was 15.5cm in addition to 0.5cm extenders.
The girth of both cylinders was 12. Interestingly, we did not find any resistance during dilation of both corpora. However, both copora ended abruptly proximally. This intraoperative finding obliged us to use a prolene mesh (PROLENE®Polypropylene Mesh – Ethicon Inc) as a sock around the rear end of the cylinder (TUBE malleable semi rigid implant). A sling of prolene 1/0 was applied via suturing through the mesh, the extender of the rear end of both cylinders, the tunica albuginea and the proximal end of the corporotomy. This mesh was inserted through the same penoscrotal incision.
On the right side, we found difficulty to wrap a mesh sock around the rear end of the cylinder due to wide gaping of the corporotomy. Hence, we were satisfied by doing sling procedure only on the right side (Fig 2). The added value of the sling procedure was to reinforce both corpora proximally. The operation lasted 2.5h without encountering an important bleeder or any other complications. Montorsi et al. (2004) was the first one to offer a solution for proximal perforation that occurs intra-operative. He used polydioxane sutures passing through the rear tip of the cylinder and the tunica albuginea at the most proximal end of the corporotomy to anchor the cylinder in a proper place. Alternatively, a Dacron sock can be sutured to the rear tip of the prosthesis and fixed to the wall of the tunica with one or two sutures.6

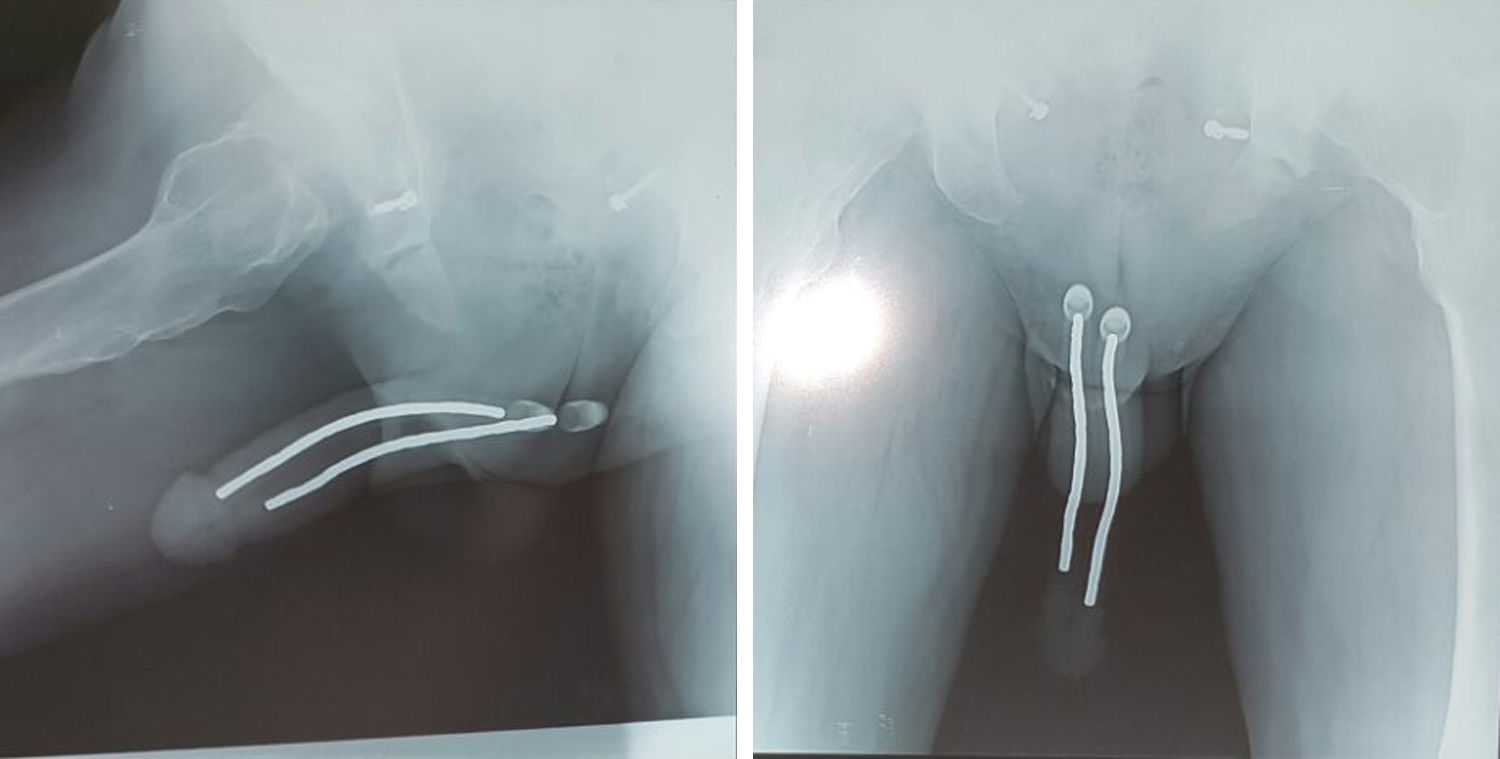
The follow up of our patient included pelvic X-ray, 3 months from the operation 19/5/2016 (Fig. 3). A photo of the patient was also being taken during the out-patient clinic visits (Fig. 4). During this period, the patient was asked about his satisfaction regarding the girth and length of the implant and the ease of use of this implant. The patient implied his satisfaction with the improved quality of life.
Ethical disclosuresProtection of human and animal subjects

The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflict of interestAll authors declare no conflict of interest.
All authors declare that they have not received any grants for this work as this case was done for free in our Andrology Department, Kasr Al-Ainy Faculty of Medicine and they have not any financial ties with the manufacturer of the semi-rigid implant mentioned in this case report. Eventually, we would like to thank Dr Lamiaa Tawfik for her sincere effort to perform English editing of this manuscript.