





Phonetics helps to establish an ideal incisal edge position in relation to the vermilion border during phoneme articulation.
ObjectiveTo evaluate the relationship between the incisal edge of the anterior teeth and the vermilion border with the severity of the malocclusion and phonemes articulation of patients attending from January to February 2015 at the Orthodontics Service of Mexico Children's Hospital «Dr. Federico Gomez».
Material and methodsA prospective, observational and cross-sectional study was performed on 40 patients of both genders between the ages of 14 to 25 years old. A digital video sequence was recorded (2minutes) while the patients pronounced different words.
Results22.5% of the patients presented phoneme articulation problems (D, K, L, R, S); the phoneme S was found to have the most statistically significant error (8%).
ConclusionIt was not observed if a relationship exists between malocclusion severity, incisal edges- vermilion border and phonemes articulation.
La fonética ayuda a establecer la posición ideal de los bordes incisales con relación al borde bermellón del labio durante la articulación de los fonemas.
ObjetivoEvaluar la relación entre la posición de los bordes incisales-borde bermellón del labio y el grado de maloclusión con la articulación de fonemas en pacientes del Servicio de Ortodoncia del Hospital Infantil de México «Federico Gómez», de enero a febrero de 2015.
Material y métodosSe realizó un estudio prospectivo, observacional y transversal en 40 pacientes ambos sexos, de 14 a 25 años de edad en los cuales se grabó una secuencia de video digital (dos minutos), mientras el paciente realiza la pronunciación de diversas palabras.
ResultadosEl 22.5% de los pacientes presentó problemas en la articulación de fonemas (D, K, L, R, S); de los cuales la S se encontró con mayor error del 8%.
ConclusiónNo se logró observar si existe asociación entre el grado de maloclusión, bordes incisales-borde bermellón del labio con la articulación de fonemas.
It has been mentioned in the literature that beauty is related to the function of the lips and teeth during orthodontic treatment. However, none of these studies have been performed with a frontal assessment of liptooth relations from a phonetic and functional point of view.1
The relationship between lips and incisal edges is important for three reasons:
- 1.
The strength of the lips influences dental alignment and stability.
- 2.
The lower lip is related to the upper incisors by placing the incisal edges in their position for a proper function of both.
- 3.
Lip closure should be easy and delicate.
When the lips are in a proper functional relationship with the incisal edges of the anterior teeth a good arch position and shape is revealed.1,2
In 410 university students with malocclusion it has been found that 87% presented speech problems, 62% an average speech function and 35% had no speech problems. It was concluded that speech problems were directly related to the severity of the dental malocclusion.3
Speech pathology involves defects in the articulation of phonemes or sounds, pace of voice and language; which involve both the orthodontist and the phoniatrist. Speech problems and dental malocclusions have a common cause: as a product of abnormal orofacial movements, as a product of neurological and myopathic conditions, of genetic origin or habits. Patients who have abnormal or immature muscular orofacial function patterns during mastication and deglutition also present malocclusion and speech disorders.4
The difficulty for the correct articulation of phonemes (sounds) is called «dyslalia», which can be classified into distortion, omission and inappropriate replacement of the consonants and vowels sounds during speech. The phoniatrist works more closely with the orthodontist in the management of combined problems of consonant sounds, when planning the amount of dynamic anterior tooth crown exposure during orthodontic treatment.4
Patients with problems for phoneme articulation tend to have a higher incidence of malocclusions, but such difficulties may also be found in normal occlusions. However, when a speech problem is present, it cannot be assumed that it is strictly related to the malocclusion; in some cases, the tongue and lips are capable of adapting to severe dental malocclusions, in other cases, where the malocclusion is mild to moderate, defects in phonemes articulation may prevail.5
Phonology is the study of the phonemes or sounds of language. The learning process of the phonological system usually begins in the first years of life and is completed at the age of 8, when the child will have the sound production and articulation of an adult.6
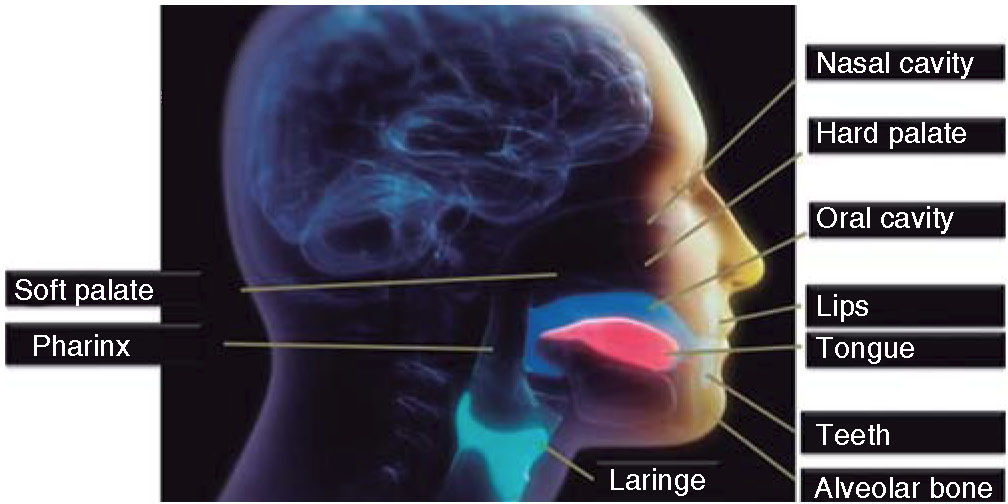
The anatomical components of the various systems used in the production of the voice are as follows:7
- •
The respiratory apparatus: Voice production depends on the balanced relationship between the forces exerted by the intrinsic muscles of the larynx and the force exerted by the air (air pressure) when exhaled from the lungs. The slightest deviation of this balance produces a significant alteration in the tone, power or quality of the voice.7
- •
Phonal system: The system that produces the sound that we call voice consists of a cartilaginous structure called larynx. The movement that results from the contraction of the intrinsic laryngeal muscles produces the characteristics of mass, length and tension that alter the vocal folds (Figure 1).7
- •
The resonance system: Resonance is a nonacoustic phenomenon that occurs when a vibrating structure (sound source) excites air in a chamber filled with air that in turn produces a similar vibration in the walls of the chamber. The human voice would sound as a weak whispering if it was not for resonance.
.")
- -
Anomalies in the vocal tube configuration that result from different tongue positions or when coupling the nasal resonance (nasal cavity) to the rest of the vocal system, produce notable acoustic changes.7
Mainly, the oral and laryngeal system is a speech mechanism. The orthodontist's job is related primarily to the sound articulation and resonance processes, which are intimately connected.8
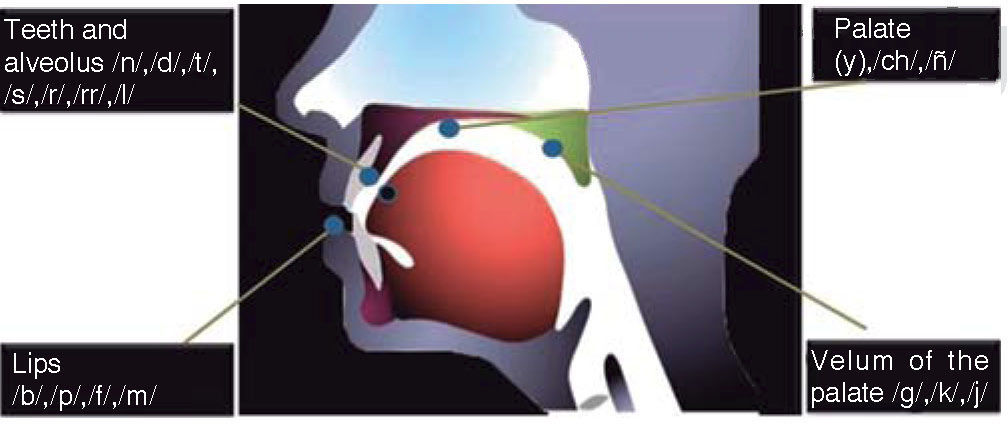
The tongue makes contact with different areas of the oral cavity in order to produce different articulation points for phonemes. These points are classified as follows:
- •
Linguovelar: the posterior portion of the tongue contacts the soft palate.
- •
Linguopalatal: the lingual dorsum contacts the hard palate.
- •
Linguoalveolar: the tip of the tongue rises to contact the alveolar ridge.
- •
Linguodental: The tip of the tongue protrudes and contacts the teeth.8
Lip function participates in two articulation points:
- 1.
Labiodental: upper incisors and lower lip.
- 2.
Labial: both lips work together.8
The most significant consonants classification method for the orthodontist identifies those consonants that are most afflicted by dental conditions:
- •
Labiodental consonants: The /f/ phoneme is produced by forcing air through the contact of the upper incisors with the lower lip.8
- •
Linguodental consonants: /t/ and /d/ are produced by forcing air through the contact or the approximation of the tip of the tongue between the upper and lower incisors.8
The aim was to assess the relationship between the incisal edges- vermillion border and the degree of maloclussion with phoneme articulation (Figure 2).
MATERIAL AND METHODS.")
The study was conducted in 40 Mexican patients between the ages of 14 and 25, who attended the Orthodontics Service of the Children's Hospital of Mexico «Federico Gomez» in the period from January to February 2015. The Specialist in Orthodontics assessed the 40 patients, who were descendants from Mexican parents. Inclusion and exclusion criteria are shown in tables I and II.
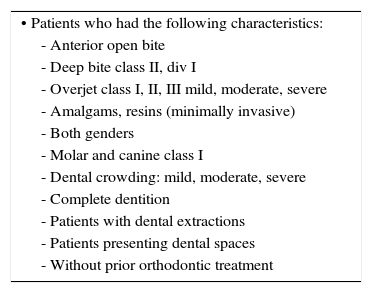
Inclusion criteria.
| • Patients who had the following characteristics: |
| - Anterior open bite |
| - Deep bite class II, div I |
| - Overjet class I, II, III mild, moderate, severe |
| - Amalgams, resins (minimally invasive) |
| - Both genders |
| - Molar and canine class I |
| - Dental crowding: mild, moderate, severe |
| - Complete dentition |
| - Patients with dental extractions |
| - Patients presenting dental spaces |
| - Without prior orthodontic treatment |
Exclusion criteria.
| • Temporomandibular joint dysfunction |
| • Previous orthodontic treatment |
| • Periodontal problems |
| • Patients with craniofacial abnormalities, alterations of the central nervous system, language problems syndromes, sequel of cleft lip and palate, diseases of the respiratory system, laryngeal malformations, surgical interventions, therapeutic manipulations, laryngeal trauma |
In the clinical chart, the measurements obtained from each patient were recorded as follows:
- •
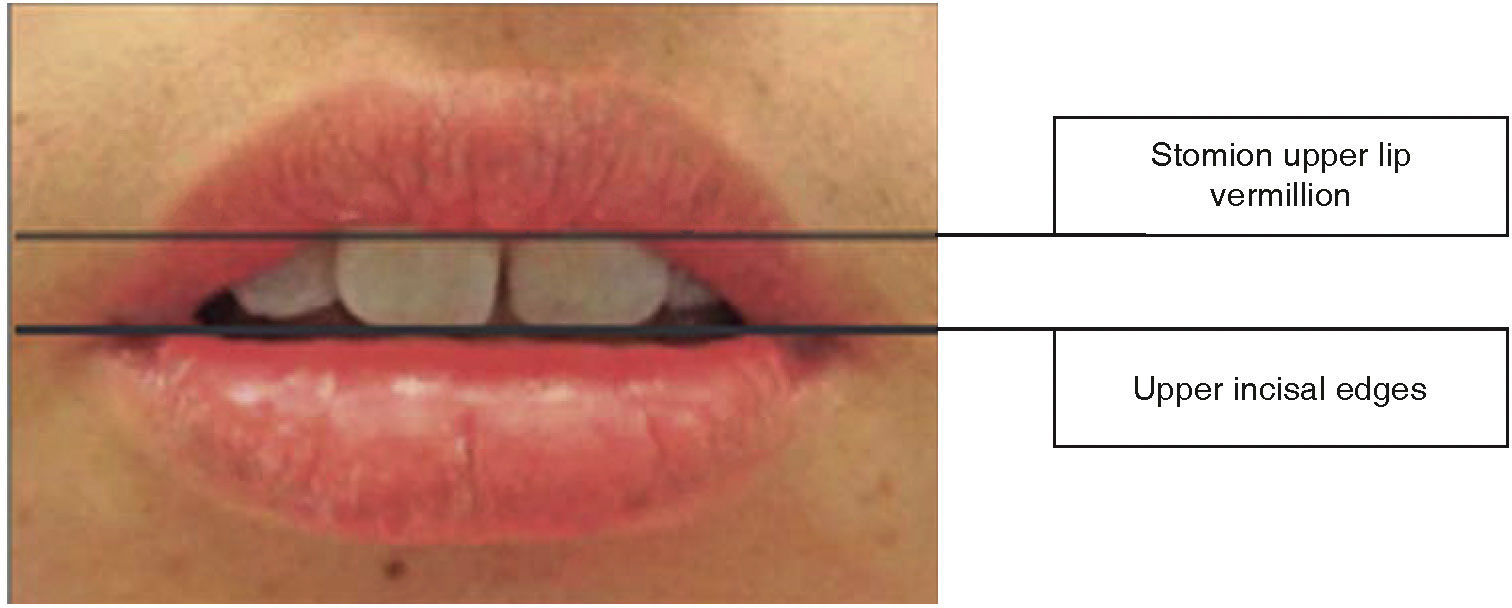
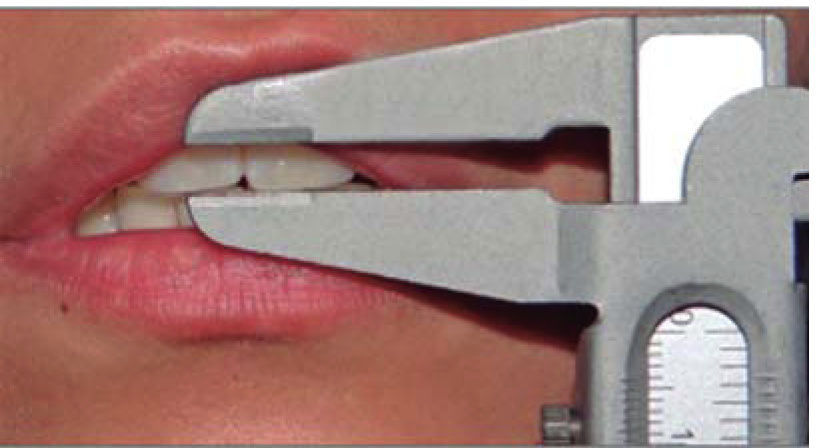
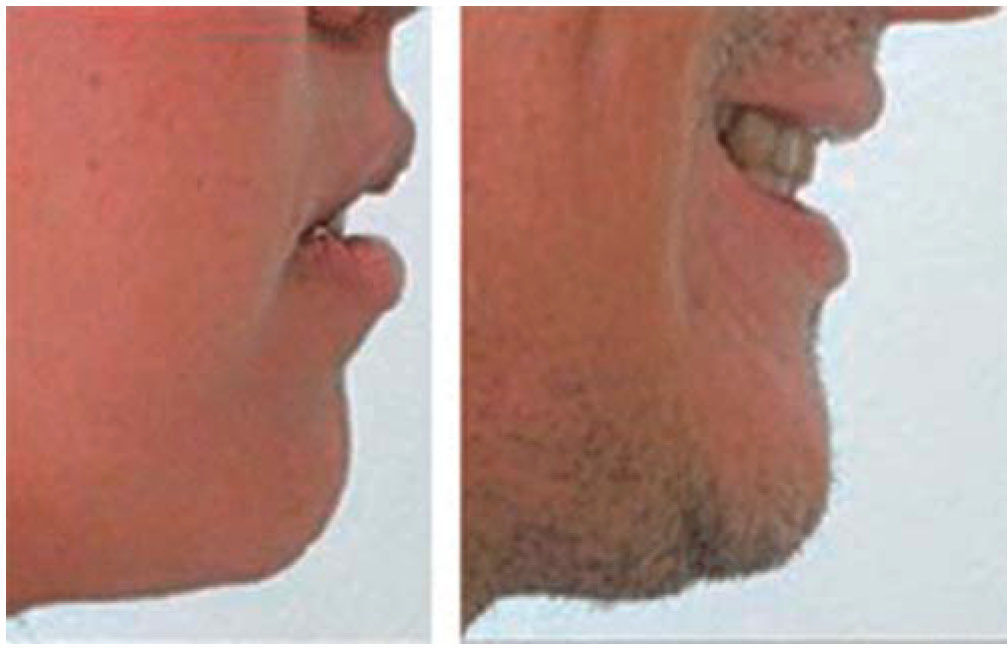
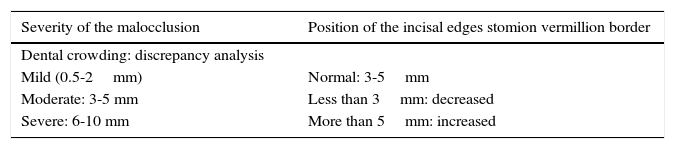
Stomion length (lower edge) of the upper vermillion border to upper incisal edges, which was classified in three categories: normal 3 to 5mm, decreased less than 3mm, increased greater than 5mm (Table IIIandFigure 3).
- •
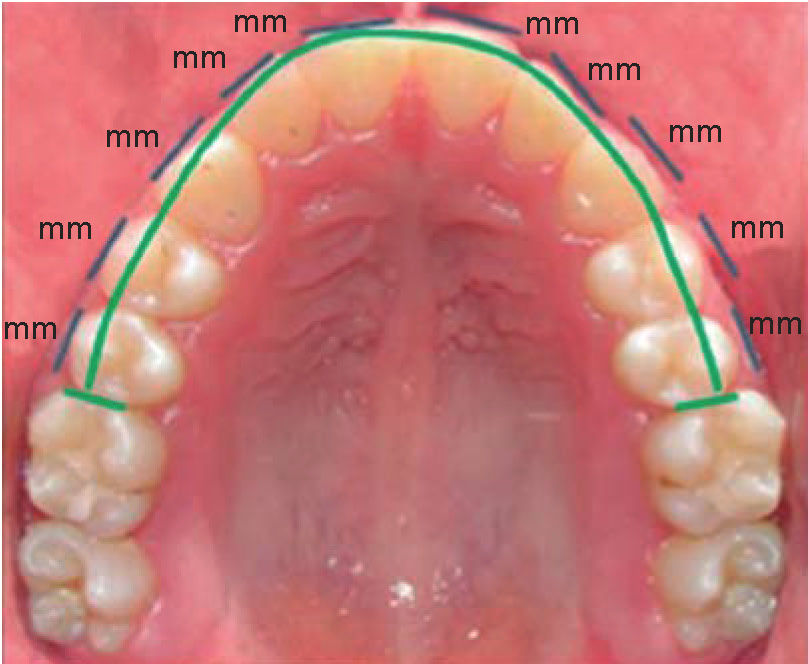
The degree of malocclusion based on the discrepancy analysis, in order to determine the degree of dental crowding that the patients presented which was classified in: mild (0.5-2mm), moderate (3-5mm), severe (6-10mm) (Table III andFigure 4).


Analysis of the upper arch based on the Nance space demand analysis performed directly in the patient's mouth.
Example: AS-RS=_______mm
Difference in millimeters between the available space and the required space was determined as the severity or degree of crowding (Figure 5).

Once the facial and intraoral measurements were obtained, 2 frontal and 2 lateral photographs were taken (one with relaxed lips and one during smile) as a backup from a static image of the position of the incisal edges. Each photograph was recorded in .jpg format with the same resolution and size (Figures 6 and 7). Subsequently, each patient was individually, assessed by the medical specialist in Speech Therapy. The phonemes considered in this study were B, C, CH, D, F, K, L, M, P, R, S. The evaluation was performed using the «Questionnaire for Child Phonological Assessment» (QCPA), that evaluates the patient's pronunciation since its structure and registration system allows for the proper assessment of the link between all phonemes. The test consisted of two parts. First, a sequence of drawings was shown to the patient who named each of them by answering the question: «What is this?» or «how is it called?». The test evaluated each phoneme articulation using the following codes: N (normal), S (replacement), O (omission), D (distortion) (Table IV). In the second part of the test the medical specialist in Speech Therapy recorded the results of the phoneme articulations where problems were found (D, K, L, R, S) in the evaluation sheet.


Terms used for the assessment of phoneme articulation.
| Sustitution |
| When a sound is replaced by other. It may occur at the beginning, in the middle or at the end of the word Example: «abble» for «apple» |
| Omition |
| When the phoneme that cannot be pronounced is omitted. |
| Example: «ipper» for «zipper» |
| Distortion |
| When there is a failure to produce a sound. The sound is pronounced in a similar way but it is not quite correct |
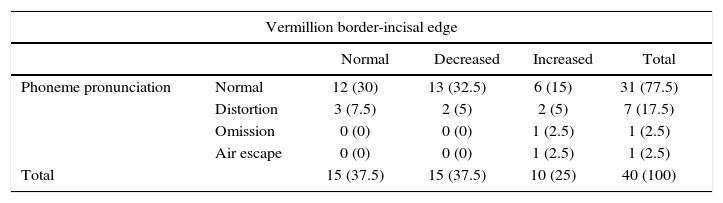
22.5% of the patients presented speech problems in relation to the incisal edge-vermillion border tables V and VI.
The table is represented relating phoneme pronunciation * vermillion border-incisal edge.
| Vermillion border-incisal edge | |||||
|---|---|---|---|---|---|
| Normal | Decreased | Increased | Total | ||
| Phoneme pronunciation | Normal | 12 (30) | 13 (32.5) | 6 (15) | 31 (77.5) |
| Distortion | 3 (7.5) | 2 (5) | 2 (5) | 7 (17.5) | |
| Omission | 0 (0) | 0 (0) | 1 (2.5) | 1 (2.5) | |
| Air escape | 0 (0) | 0 (0) | 1 (2.5) | 1 (2.5) | |
| Total | 15 (37.5) | 15 (37.5) | 10 (25) | 40 (100) | |
* Frequency is shown and between parentheses the percentage inside the variable vermillion border-incisal edge.
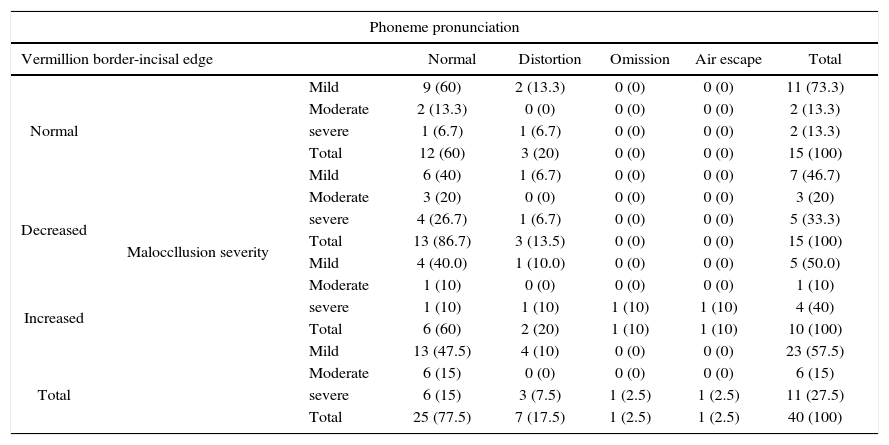
The table is represented relating the malocclusion severity * phoneme pronunciation * vermillion border-incisal edge.
| Phoneme pronunciation | |||||||
|---|---|---|---|---|---|---|---|
| Vermillion border-incisal edge | Normal | Distortion | Omission | Air escape | Total | ||
| Normal | Maloccllusion severity | Mild | 9 (60) | 2 (13.3) | 0 (0) | 0 (0) | 11 (73.3) |
| Moderate | 2 (13.3) | 0 (0) | 0 (0) | 0 (0) | 2 (13.3) | ||
| severe | 1 (6.7) | 1 (6.7) | 0 (0) | 0 (0) | 2 (13.3) | ||
| Total | 12 (60) | 3 (20) | 0 (0) | 0 (0) | 15 (100) | ||
| Mild | 6 (40) | 1 (6.7) | 0 (0) | 0 (0) | 7 (46.7) | ||
| Decreased | Moderate | 3 (20) | 0 (0) | 0 (0) | 0 (0) | 3 (20) | |
| severe | 4 (26.7) | 1 (6.7) | 0 (0) | 0 (0) | 5 (33.3) | ||
| Total | 13 (86.7) | 3 (13.5) | 0 (0) | 0 (0) | 15 (100) | ||
| Mild | 4 (40.0) | 1 (10.0) | 0 (0) | 0 (0) | 5 (50.0) | ||
| Increased | Moderate | 1 (10) | 0 (0) | 0 (0) | 0 (0) | 1 (10) | |
| severe | 1 (10) | 1 (10) | 1 (10) | 1 (10) | 4 (40) | ||
| Total | 6 (60) | 2 (20) | 1 (10) | 1 (10) | 10 (100) | ||
| Mild | 13 (47.5) | 4 (10) | 0 (0) | 0 (0) | 23 (57.5) | ||
| Total | Moderate | 6 (15) | 0 (0) | 0 (0) | 0 (0) | 6 (15) | |
| severe | 6 (15) | 3 (7.5) | 1 (2.5) | 1 (2.5) | 11 (27.5) | ||
| Total | 25 (77.5) | 7 (17.5) | 1 (2.5) | 1 (2.5) | 40 (100) | ||
* Frequency is shown and between parentheses the percentage inside the variable vermillion border-incisal edge.
It was found that in the majority of patients with a mild degree of malocclusion and a decreased or increased vermilion lip border; as well as, in a small number of patients with a moderate to severe degree of malocclusion there was a correct pronunciation (Table VI).
Once the phonemes where there were pronunciation problems as: distortion, omission, air exhaust identified evaluated individually in relation with the incisal edge-to-edge lip vermilion (Tables VII to XI).
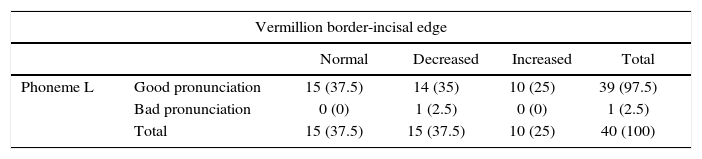
The table shows the relationship of phoneme L.
| Vermillion border-incisal edge | |||||
|---|---|---|---|---|---|
| Normal | Decreased | Increased | Total | ||
| Phoneme L | Good pronunciation | 15 (37.5) | 14 (35) | 10 (25) | 39 (97.5) |
| Bad pronunciation | 0 (0) | 1 (2.5) | 0 (0) | 1 (2.5) | |
| Total | 15 (37.5) | 15 (37.5) | 10 (25) | 40 (100) | |
*The frequency is shown and between parenthesis, the percentage inside the variable vermillion border-incisal edge.
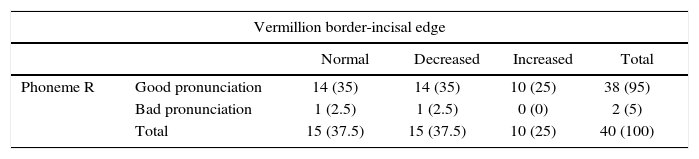
The table shows the relationship of phoneme R.
| Vermillion border-incisal edge | |||||
|---|---|---|---|---|---|
| Normal | Decreased | Increased | Total | ||
| Phoneme R | Good pronunciation | 14 (35) | 14 (35) | 10 (25) | 38 (95) |
| Bad pronunciation | 1 (2.5) | 1 (2.5) | 0 (0) | 2 (5) | |
| Total | 15 (37.5) | 15 (37.5) | 10 (25) | 40 (100) | |
*The frequency is shown and between parenthesis, the percentage inside the variable vermillion border-incisal edge.
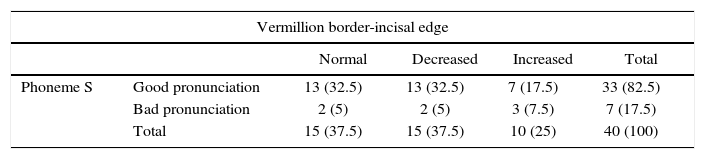
The table shows the relationship of phoneme S.
| Vermillion border-incisal edge | |||||
|---|---|---|---|---|---|
| Normal | Decreased | Increased | Total | ||
| Phoneme S | Good pronunciation | 13 (32.5) | 13 (32.5) | 7 (17.5) | 33 (82.5) |
| Bad pronunciation | 2 (5) | 2 (5) | 3 (7.5) | 7 (17.5) | |
| Total | 15 (37.5) | 15 (37.5) | 10 (25) | 40 (100) | |
* The frequency is shown and between parenthesis, the percentage inside the variable vermillion border-incisal edge.
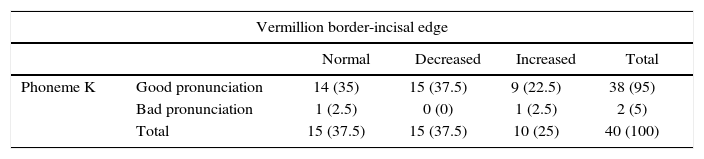
The table shows the relationship of phoneme K.
| Vermillion border-incisal edge | |||||
|---|---|---|---|---|---|
| Normal | Decreased | Increased | Total | ||
| Phoneme K | Good pronunciation | 14 (35) | 15 (37.5) | 9 (22.5) | 38 (95) |
| Bad pronunciation | 1 (2.5) | 0 (0) | 1 (2.5) | 2 (5) | |
| Total | 15 (37.5) | 15 (37.5) | 10 (25) | 40 (100) | |
* The frequency is shown and between parenthesis, the percentage inside the variable vermillion border-incisal edge.
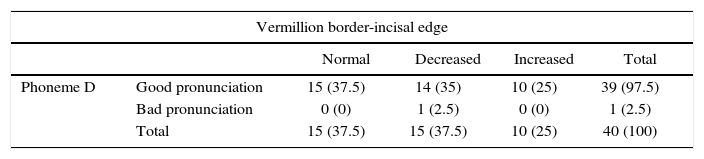
The table shows the relationship of phoneme D.
| Vermillion border-incisal edge | |||||
|---|---|---|---|---|---|
| Normal | Decreased | Increased | Total | ||
| Phoneme D | Good pronunciation | 15 (37.5) | 14 (35) | 10 (25) | 39 (97.5) |
| Bad pronunciation | 0 (0) | 1 (2.5) | 0 (0) | 1 (2.5) | |
| Total | 15 (37.5) | 15 (37.5) | 10 (25) | 40 (100) | |
* The frequency is shown and between parenthesis, the percentage inside the variable vermillion border-incisal edge.
In phonemes L, R, K, D 2.5% of the patients showed an incorrect pronunciation (Tables VII, VIII, X and XI).
With a decreased and an increased incisal edgevermillion border, 8% of the patients exhibited an incorrect pronunciation of phoneme S (Table IX).
DISCUSSIONFrom a physiological point of view, the correct pronunciation of words is that which is produced without any change in its functional and anatomical dynamics. Teeth positions and their relation to the support tissues are fundamental in the physiology of speech since changes in the positions of these hard and soft tissues affect the air flow necessary to produce the vocal pitch and normal or defective sounds. Vallino and Thompson9 in their investigations recognized that dental malocclusions are important factors in speech pathology; within their investigation group, it was determined that the lingual-dental consonant D was affected in 75% of the cases followed by the alveolar consonants R, RR, L in 60% of the cases, the dental consonant S in 45% and in a smaller frequency N, Z, and F in a 30% of the patients. These results coincide with the data obtained through this study where pronunciation problems were found in phonemes D, K, L, R and S out of the 11 studied phonemes.
The anomalies of dental occlusion are the most frequent cause of organic dislalias; increased overjet and diastemas were the malocclusions that most frequently caused articulation alterations.10 Groups with abnormal dental conditions or disorders of sound articulation have confirmed the 1 to 1 ratio between the dental condition and speech problems.8
Fymbo3 placed special emphasis on the importance of abnormal vertical relations of the arches especially open and deep bites where only 29% of the patients with deep bite and 21% with open bite had satisfactory language. In the present study the vertical relationship of the upper incisors with the upper lip vermillion border was considered and no relationship was found between a faulty pronunciation of the phonemes and a decreased or increased vermilion border.
Subtelny et al5 concluded that some patients with increased overjet adapted to produce sounds. Patients with normal pronunciations positioned the tip of the tongue slightly posterior to the lower incisors and those with language problems, protruded the tip of the tongue significantly ahead of the lower incisors to have contact with the surfaces of the upper incisors which were also protruded.
Fairbanks and Lintner11 studied the relationship between malocclusion and defects in sound articulation. 72% of the studied children showed that there was no relationship between speech problems and malocclusion. These results coincide with those obtained by Fairbanks and Lintner where no association was found between malocclusion severity and phoneme pronunciation.
Travis12 noted that «anomalies of the orofacial structures couldn’t be considered as primary causes of the defective articulation of phonemes». There is evidence of considerable adaptability in the use of the lips and tongue to compensate for dental malformations; that in most of the cases, adaptation or compensation exceeds the task of the malocclusion. In this study there was no association between malocclusion severity and phoneme pronunciation.
Bloomer13 stated that the effects on speech may be direct or indirect: indirect, due to mechanical difficulties of the person trying to achieve the correct position and movement of the tissues of the speech; and indirect, due to the influence that deformations may exercise in the physical and mental health of the individual.
The problem is not a simple relationship of cause and effect because some malocclusions do not cause discernible phonetic anomalies due to an excellent adjustment mechanism.14 It is important to mention that the abovementioned statement has a relationship with the results found in this study in which no association was found between the severity of the malocclusion, position of the incisal edges-vermilion border and phoneme pronunciation.
CONCLUSIONSNo direct association was found between malocclusion severity and the position of the incisal edges vermilion border with phoneme articulation due to the reduced amount of patients in the sample. Other factors may be associated with phoneme pronunciation such as the anatomical and physiological characteristics of the patient (tongue, frenulum, palate, lip tone and muscular, etc), degree of adaptability and neuromuscular control, so it is suggested to continue with a second phase of research to go into more detail on this study.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia