







Goldenhar's syndrome, named after Dr M Goldenhar, is normally reserved for cases presenting hemi-facial microsomy. This syndrome normally affects upper and lower jaws, pinna, and adjacent tissues in a hemi-face. The target of this rehabilitation is to restore to its maximum possible extent patient's esthetics and masticatory function. We present intra-oral rehabilitation of a Goldenhar Syndrome patient who attended the maxillofacial prosthesis clinic. The patient exhibited complete edentulism, maxillary and mandibular hypoplasia (this latter compensated with a titanium chain). Prosthetic bi-maxillary rehabilitation was undertaken, bearing in mind circumstances of facial asymmetry, mandibular movement limitations and decreased alveolar ridges. Treatment was mainly focused on improvement of esthetic, phonetic and masticatory functions, which, as a whole are crucial in patient's day-to-day life and quality of life.
El síndrome de Goldenhar en honor al Dr. M. Goldenhar suele reservarse para los casos que presentan microsomía hemifacial. Este síndrome suele afectar principalmente maxilar, mandíbula, pabellón auricular, globo ocular y tejidos adyacentes de una hemicara. El objetivo de esta rehabilitación es devolver en medida de lo posible, la función masticatoria y estética al paciente. A continuación se presenta la rehabilitación intraoral de una paciente con síndrome de Goldenhar que acudió a la clínica de PMF presentando, eden- tulismo total hipoplasia maxilar y mandibular (esta última compensada con una cadena de titanio). Se realizó rehabilitación protésica bimaxilar, teniendo en cuenta la asimetría facial, la limitación de movimiento mandibular y la disminución de los procesos alveolares. El tratamiento fue enfocado principalmente en mejorar la función masticatoria, fonética y estética, que en conjunto son determinantes en la cotidianidad del paciente y su calidad de vida.
Description of this syndrome corresponds to Dr Goldenhar (1952) who established its clinical definition as: association of malformations of the eyeball and ear, particularly of dermoid, epibulbar, pre-auricular appendix and pre-auricular fistula. Gorlin (1963) named it «ocular-auricular-vertebral dysplasia». Other synonyms are «Goldenhar-Gorlin syndrome» «Hemi-facial microsomy» and «First and Second branchial arch syndrome».1–4 Jones (1988) considers it a spectrum and torso as «sequence» since it offers varied degrees of a same initial morphogenesis disorder.5–7 Mean incidence varies from one in 3,000 to 5,000 live births.1
Two types of treatments, surgical and prosthetic, are used to rehabilitate these patients.4 Surgical treatment is preferred: it consists on several surgical interventions to achieve long term results, which oftentimes are not the expected ones.4–6 According to the case and involvement degree of patient's anatomical structures, the following treatments can be used: removable partial prostheses, fixed prostheses, full prostheses as well as overdentures.
In general, rehabilitation by means of a prosthesis, is an individualized treatment, which for the patient represents the advantages of being low cost and non invasive.
A patient afflicted with «Goldenhar syndrome» was treated at the Maxillofacial Prosthesis Clinic of the UNAM (National Autonomous University of Mexico). Due to bone circumstances presented by the patient, treatment consisted on placement of individualized full prostheses.
ObjectiveManufacture of a full upper prosthesis and a hybrid lower prosthesis. The upper denture was hollowed out in order to lighten the device's weight, the lower denture was left with full weight so as to improve stability and restore patient's esthetics and function.
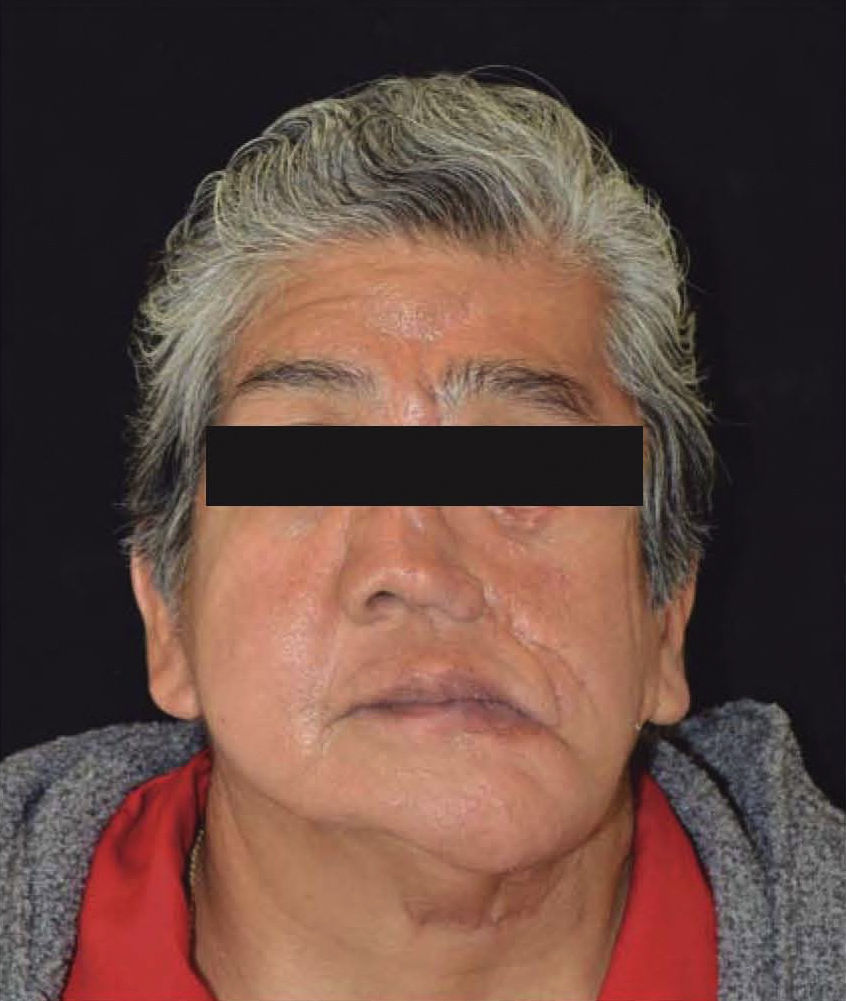
MATERIAL AND METHODSA 64 year old female patient, diagnosed with Goldenhar's syndrome, she had undergone 21 surgeries to improve function and esthetics (Figure 1). One of the conducted surgical procedures was a mandibular osseous distraction, which resulted in osteomyelitis. As a result, a hemi-mandibulectomy with titanium chain placement was conducted in order to compensate resulting bone defect. In consequence a practically non-existent residual ridge was obtained (Figures 2 and 3). The patient exhibited a «V» shaped palate, with portions of mobile tissue and generalized bone loss causing considerable loss of vertical dimension (Figure 4).




Treatment: a hollowed-out full upper denture was manufactured so as to alleviate its weight; a lower denture with «Remanium» bar was manufactured so as to slightly increase the denture's weight without increasing its volume.
PROCEDUREImpressions: Primary impressions were taken with alginate (Jeltrate Chromatic® Dentsply) as well as prefabricated trays (Den Tray® II, Sultan Health).
These impressions were achieved in a positive model, in type III plaster (Quick Stone®, Whip Mix). Based on the aforementioned models, an individual tray was manufactured for each arch, and a new impression was taken with polysulfide rubber (Permalastic® Kerr). A positive model was obtained with type IV plaster (Silky Rock®, Whip Mix), so as to later manufacture a recording base and all-season pink wax rolls. OJ (Rogson® Wax.
Model mounting: After achieving cranio-mandibular recordings, models were mounted with facial arch in a semi-adjustable articulator (Bioart articulator). Cross bite teeth (Ivostar®, Ivoclar Vivadent) were used.
Muffle use: Once teeth were aligned and suitable tests were performed on the patient, direct muffle procedure was undertaken by placing over articulated teeth a heavy body silicon coat (Speedex®, Coletene Whaledent) in order to achieve a clean, easy to polish denture. Lost-wax technique was used. Once the dentures were de-waxed a horseshoe with the length of the lower arch was modeled in wax. It was then cast in metal so as to become the weight of the lower denture. Once the metal horseshoe was trimmed and polished, it was overshadowed so as to avoid staining the acrylic which would have given a negative appearance to the denture.
For the upper denture, in the right side presenting larger bone loss, it was decided to compensate with larger amounts of material. This denture was hollowed out in order to avoid greater weight. An acrylic half base (Lucitone 199® Dentsply) was manufactured on the positive plaster model of the upper arch. A small portion of heavy silicon (Speedex® Coltene/ Whaledent) was placed over it as filling material to temporarily occupy the space in the acrylic of the denture, and thus lighten its weight.
Final detailing: Both dentures were retrieved from the muffle, they were then trimmed and polished.
A small opening in the palate was performed in the upper denture so as to be able to remove silicon filling, resulting space was then sealed with self-curing acrylic (Figure 5). To finish procedure, dentures were polished to a high gloss with the help of a bench motor (High Speed Alloy Grinder AG05® Ray Foster), mounted pink stone (pink color mounted stones YINJILI), polishing strips and polishing material (Polyacril®) (Figure 6).


Some selective adjustments were achieved with articulating paper (Progress 100® Bausch).
RESULTSProstheses compensated excessive decrease of vertical dimension.
The patient reported comfort and denture acceptance after conducting intra-oral tests of lateral mobility and occlusion.
Prosthetic treatment helped to improve patient's esthetic, phonetic and masticatory functions. She informed of improved masticatory and phonetic functions which enhanced her self esteem and quality of life.
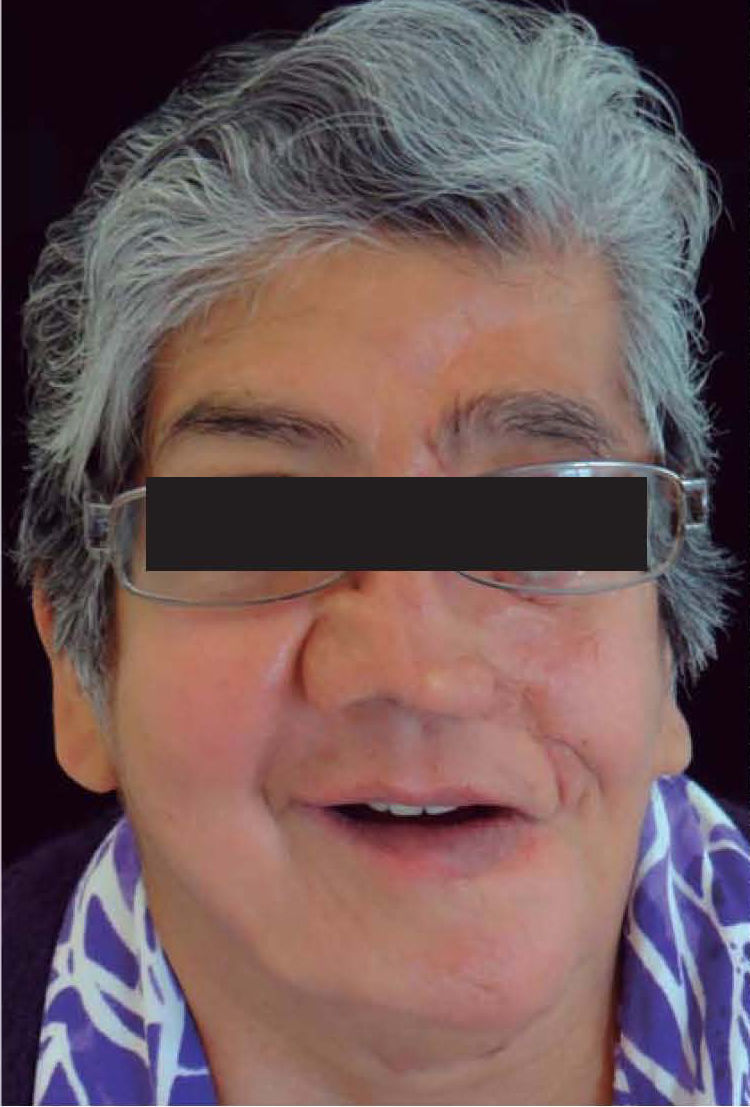
Patient follow-up after one month, six months and one year revealed that dentures remained comfortable and functional (Figure 7).
DISCUSSION
Patients presenting Goldenhar symptoms are oftentimes subjected to excessive and multiple surgeries aimed at the correction of hypoplasia.4-6 In the present clinical case, the patient had been previously subjected to so many surgeries, that she flatly refused any further ones, even though the stability of her prosthetic rehabilitation could have been improved with implants. This type of apparently conventional rehabilitation finds itself outside of the standards established and dictated in total Prosthodontics. It nevertheless allowed us to improve the patient's quality of life in a non-invasive manner, and elicit satisfactory results.
CONCLUSIONBased on rehabilitation results presented in the present article we might be able to conclude that hybrid dentures were manufactured which met, as far as possible, prosthetic objectives such as phonetics, mastication and esthetics.
This article can be read in its full version in the following page: http://www.medigraphic.com/facultadodontologiaunam