


This study compares the validity of two different methods with linear and angular measurements (Olive-Basford's method and Olmos’ method) used as predictive methods of mandibular third molar impaction.
MethodsA long-term follow-up study analyzing measurements over dental panoramic radiographs in three consecutive times (at the time of baseline evaluation (t1) and 3 (t2) and 6 (t3) years later) during six years was realized in 32 orthodontic patients. The discrimination accuracy in each time was evaluated by using the Receiver Operating Characteristic (ROC) curve.
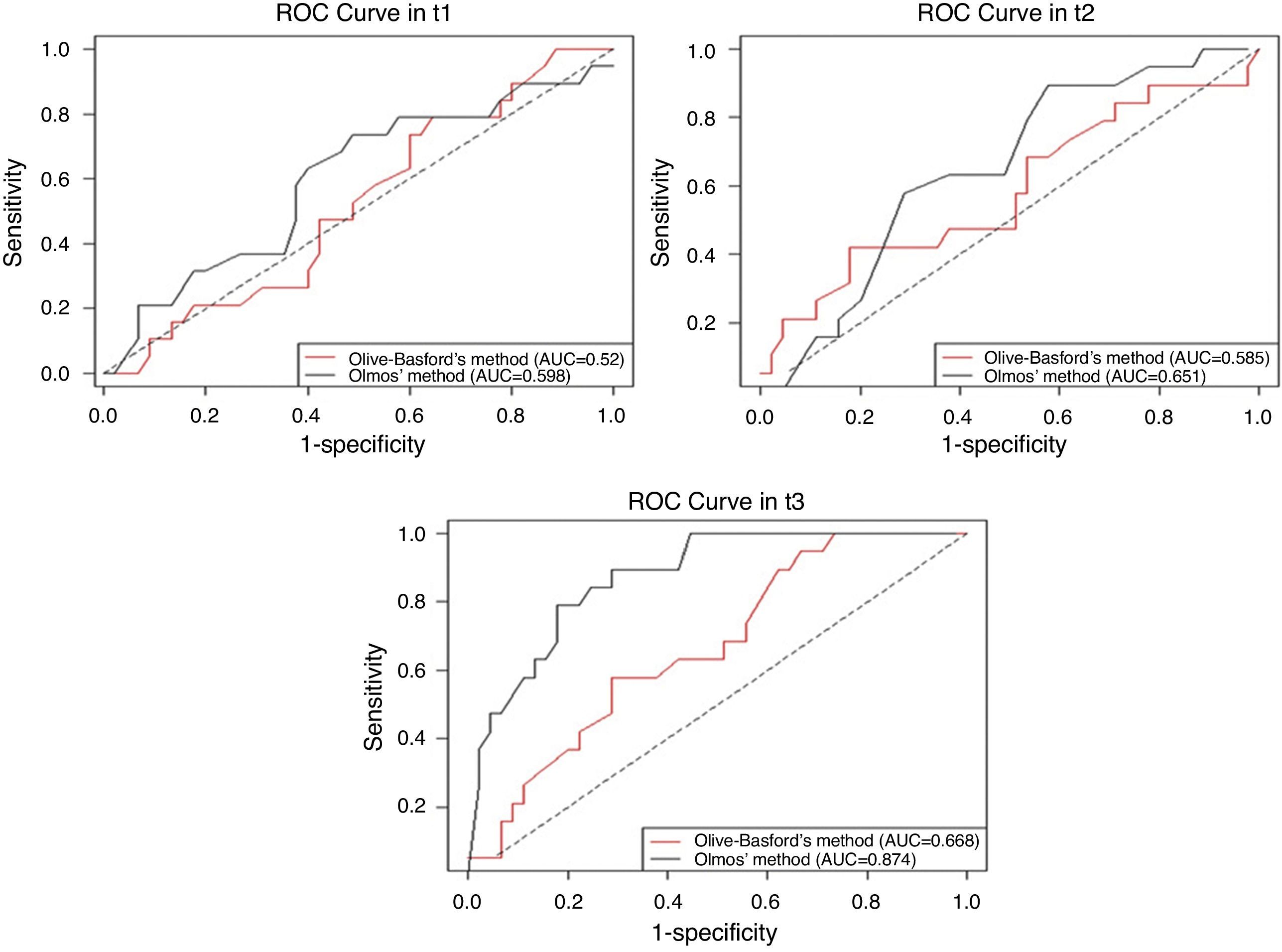
ResultsThe area under the ROC curve (AUC) in t1 and t2 was slightly higher in the Olmos’ method, but there were no statistically significant differences between both methods (p=0.483 and p=0.552, respectively). However, in t3, significant differences were detected (p<0.05), where the AUC for Olmos’ method was 0.874 (95% CI: 0.788–0.959), showing a high discrimination capacity of this method.
ConclusionsThe Olmos’ method improves the prediction of the third molar eruption, allowing a higher level of discrimination in clinical practice to identify the likelihood of impaction on panoramic radiographs.
Este estudo compara a validade de 2 métodos diferentes, com medidas lineares e angulares (método de Olive-Basford e método de Olmos) usados como métodos preditivos da impactação do terceiro molar mandibular.
MétodosUm estudo de seguimento analisa as medições sobre radiografias panorâmicas em 3 vezes consecutivas (no momento da avaliação inicial [T1], 3 anos [T2] e 6 anos [T3]), durante 6 anos, realizado em 32 pacientes ortodônticos. A precisão da discriminação em cada tempo foi avaliada usando o Receiver Operating Characteristic (ROC).
ResultadosA área sob a curva ROC (AUC) em T1 e T2 foi ligeiramente superior no método de Olmos, mas não houve diferenças estatisticamente significativas entre os 2 métodos (p=0,483 e p=0,552, respetivamente). Entretanto, em T3, foram detetadas diferenças significativas (p<0,05) em que a AUC para o método de Olmos foi 0,874 (IC 95%: 0,788-0,959), que mostra uma alta capacidade de discriminação deste método.
ConclusõesO método de Olmos demonstrou permitir uma maior capacidade de previsão de erupção do terceiro molar na prática clínica e da probabilidade de impactação através da análise de radiografias panorâmicas.
The third molar eruption is a complex multifactorial process. It has been previously reported that patterns of facial growth, jaw development and tooth size are inherited and the eruption pattern differs between populations, races and gender. All these factors are crucial to the eruption pattern and impaction status of mandibular third molar that exhibit the highest rate of tooth impaction reported.1 The mandibular third molars are the most frequently impacted teeth that can be found in human without sexual dimorphisms.2–4 The prevalence of the third molar impaction ranges from 16.7% to 68.8%.3 Third molar impaction may be caused by inadequate space, limited skeletal growth, distal eruption of the dentition, vertical direction of condylar growth, increased crown size of impacted teeth, and the late or retarded maturation of the third molars.2 Although the average age for eruption of the third molar is considered 20 years old by Garcia and Chauncey (1989), the time of the eruption shows considerable variations among populations ranging from 14 to 24 years old.5,6 The frequency of mandibular third molar impaction was 56.8% in orthodontic patients and the tooth position observed most often was mesioangular inclination with a frequency of 50.0%.7
A strategy to prevent impaction or partial eruption of the third molars need first identify when the third-molar impaction occurs. The prediction of eruption of the third molar tooth is associated with great uncertainty. An important variable to predict eruption of third molars is mesiodistal space between the distal surface of the second molar to the ascending ramus of the mandible.8 Some authors were reported that if this mesiodistal space is large than the mesiodistal width of the third molar crown the probability of its eruption is approximately 70%. However third molar eruption cannot be guaranteed despite adequate space available in the jaw.9 Several methods to predict the third molar eruption have been presented using lateral radiographs, bite-wings, anterior-posterior radiographs, periapical radiographs or panoramic radiographs.10–15 The different methods included measurement of the available space,10,11 mandibular size and growth10,12 and third molar angulation.14,16 Prediction in the patient during growth could be of great interest and help planning future dental treatments (orthodontic, prosthesis or surgical exodontia). Because when most dental treatments start, third molars often show a limited amount of calcification and just start to develop. Probably the excessive high rate of asymptomatic third molar extraction is due to a lack of reliable and simple predictive tools. Therefore, it is often very difficult to predict whether these teeth will erupt or remain impacted.5 Third molar impaction is a major problem in modern human without interproximal attrition.7 Skull materials indicate that third molar impaction was relatively infrequent in primitive populations.8 Few studies in the scientific literature have been conducted to compare different predictive methods in the prognosis of the third molar eruption.17 In fact, a high number of third molar eruption prediction methods have been described by various authors but none of these methods predicted the third molar eruption with great accuracy.18
The aim of the present study was to evaluate accuracy of two different methods (Olive-Basford’19 and Olmos’ methods20), used to predict the impaction of the mandibular third molar and measured on panoramic radiographs.
Material and methodsThe present study was undertaken after approval by the Research Ethics Committee of the University of Santiago de Compostela. All subjects agreed to participate in the study after prior informed consultation and signed a written informed consent. Forty-two patients attending the Valladares and Olmos Clinic in Pontevedra (Spain) for orthodontic treatment were reviewed from the database. The patients with unerupted mandibular third molar at the time of the baseline (t1) evaluation were selected to participate. The subjects included in this study fulfilled the following criteria: no previous orthodontic or orthognathic surgical treatment, no missing or extracted permanent teeth, no history of medical conditions that could alter the growth or tooth eruption and all panoramic images were of good quality. The time interval between the panoramic radiographs did not exceed 3 years in the second evaluation (t2) and 6 years in the latest evaluation (t3).
The radiographs of all patients were made under standard conditions with Satelec X Mind Pano Cephat machine (Satelec®, Acteon Group® Dental Equipment, France) in the baseline time (t1) and in the other two times (t2 and t3) by the same operator radiological technician (70Kvp, 16mA, analog position of patient, 20s).
A total of 64 third molars were selected and the eruption status was registered. Thorough oral examination of the status of the mandibular third molar in follow-up periods ((t2 and t3) that included emergence of third molar in oral cavity (eruption) or incomplete eruption (uneruption) defined as impaction.
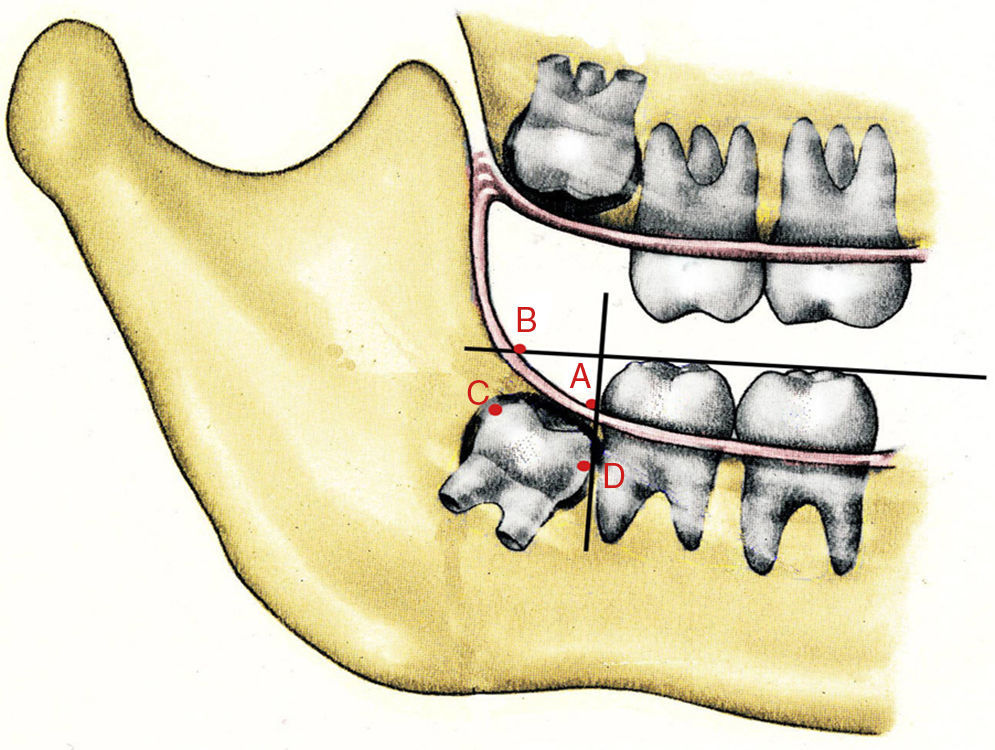
The prediction of eruption was assessed in all third molars with two radiographic methods by the same operator (MVD) in the three evaluation times (t1, t2 and t3): Olive-Basford's and Olmos’ methods. The Olive-Basford's method19 to predict eruption or impaction of the lower third molars is based on measurements of the Space-Width Ratio found by dividing the space available (AB) by the mesiodistal width of the lower third molar (CD). The occlusal plane is defined as the line drawn through the cusp tip of the first premolar and the cusps of the second molar. The measurements were done by a single operator using a right-angle T and a black ink marker waterproof extra-fine tip. The points were identified in Fig. 1: A is the point on the occlusal plane perpendicularly above the most distal point on the crown of the lower second molar. B is the intersection of the lower occlusal plane and the anterior border of the mandibular ramus. C and D mark the maximum mesiodistal width of the lower third molar. The space available AB, the mesiodistal width of the lower third molar CD, and Space-Width Ratio (AB/CD) was calculated. For a ratio AB/CD×100>120% it was assigned a future probability of eruption for a ratio, AB/CD≥1 ideal relationship to erupt; AB/CD=0.75 acceptable relationship to erupt and AB/CD<0.75 probable dental impaction.

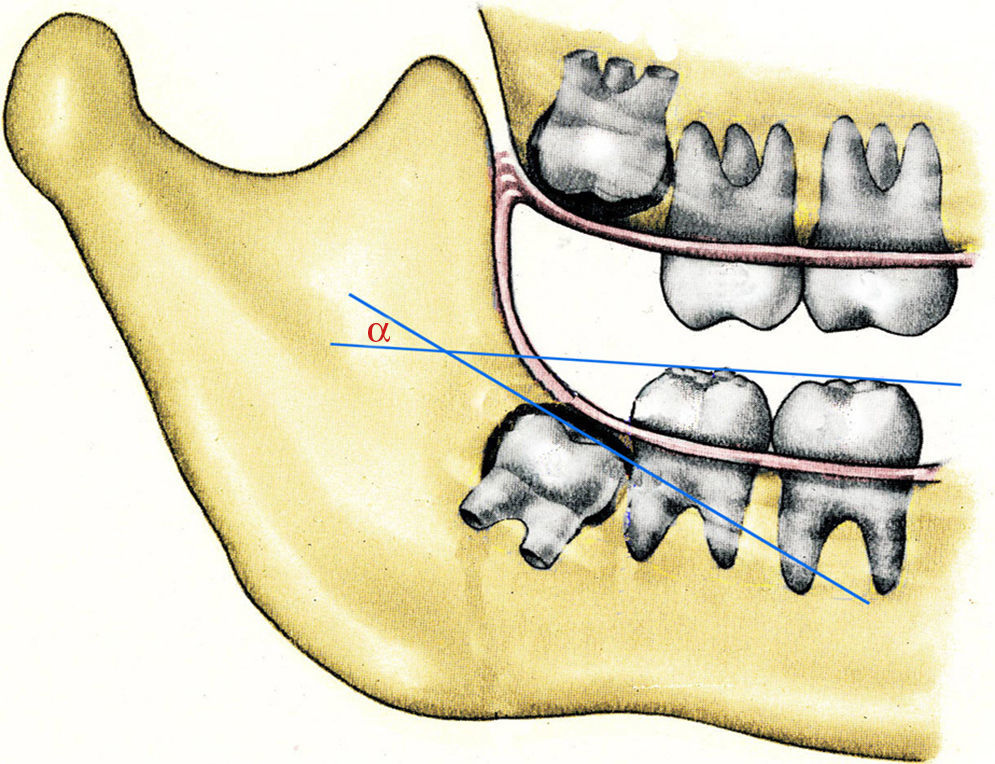
The Olmos’ method20 assesses the inclination of the mandibular third molar angle formed by the tangent through the occlusal surface of the mandibular third molar and the tangent through the occlusal surfaces of lower first molar, first and second premolars; or lower first molar and lower first and second molar and first and second lower temporary molars (Fig. 2). This method determines that if the angle is less than or equal to 32°, the third molar eruption is possible, but if the angle is higher than 32°, the lower third molar has the potential to impact. The angle measurements were determined for using of a protractor on panoramic radiographs.

Qualitative variables were expressed as frequencies and percentages; quantitative variables were expressed as mean±standard deviation. The assumption of normality was analyzed through the Kolmogorov-Smirnov test. The χ2 test was used as required to compare qualitative variables. The one-way ANOVA test was used to contrast quantitative and qualitative variables.
The discrimination accuracy of these methods (Olive-Basford's method and Olmos’ method) as predictors of eruption of mandibular third molar was evaluated in the three times pre-established, by using the Receiver Operating Characteristic (ROC) curve. It is a commonly used diagnostic tool, in which the Sensitivity (probability that the method classifies an erupted third molar correctly) is plotted against the 1-Specificity (probability that the method classifies incorrectly an un-erupted molar) for all possible values of the corresponding method considered as cut-points. The gold standard (true status) was the status of the third molar (erupted/un-erupted) at the end of the follow-up (t3). The information provided by the ROC curve is usually summarized in a numerical index as the area under the curve (AUC).21,22 This can be interpreted as the probability that in a randomly selected pair of un-erupted and erupted third molars, the value of the method is higher for the erupted molar. Values of AUC close to 1 indicate that the method has a high diagnostic accuracy. It was accompanied by its corresponding 95% confidence interval.22 The accuracy of two predictive methods was compared to determine the best method using the homogeneity areas test based on the statistic Chi-square statistic.23 All statistical analyses were carried out with R 2.12.0 statistical software.24
ResultsA total of 64 mandibular third molar teeth (32 left and 32 right third molars) from 15 (46.88%) female and 17 (53.12%) male patients were included in this study. The average age of the subjects was 12.70±1.83 years in t1, 15.24±1.78 years in t2 and 17.9±2.45 years in t3.
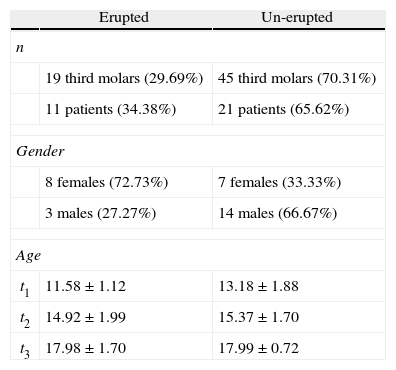
Three years later (t2) only one tooth erupted and at the end of the follow-up time, 6 years later (t3), 19 teeth (29.69%) were erupted in 11 patients (8 females and 3 males). Taking into account the final status of the third molar (eruption/un-eruption) in t3, no statistically significant differences were detected between the ages of the patients of these two groups in t2 and t3 (p=0.361 and p=0.986, respectively), mainly in t3, where ages were virtually the same in both groups (see Table 1). However, there were significant differences in t1 (p≤0.001).
Distribution of study sample by gender and age in erupted and un-erupted third molars at final follow-up time.
| Erupted | Un-erupted | |
| n | ||
| 19 third molars (29.69%) | 45 third molars (70.31%) | |
| 11 patients (34.38%) | 21 patients (65.62%) | |
| Gender | ||
| 8 females (72.73%) | 7 females (33.33%) | |
| 3 males (27.27%) | 14 males (66.67%) | |
| Age | ||
| t1 | 11.58±1.12 | 13.18±1.88 |
| t2 | 14.92±1.99 | 15.37±1.70 |
| t3 | 17.98±1.70 | 17.99±0.72 |
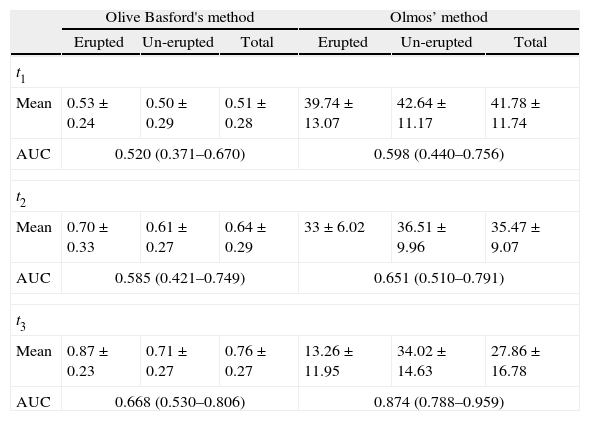
The means of Olive-Basford's and Olmos’ methods were calculated for each of the groups divided into erupted and un-erupted based on the t3 status for all three time intervals (see Table 2).
Mean values and AUCs for Olive Basford's and Olmos’ methods in erupted and un-erupted third molars at final follow-up time.
| Olive Basford's method | Olmos’ method | |||||
| Erupted | Un-erupted | Total | Erupted | Un-erupted | Total | |
| t1 | ||||||
| Mean | 0.53±0.24 | 0.50±0.29 | 0.51±0.28 | 39.74±13.07 | 42.64±11.17 | 41.78±11.74 |
| AUC | 0.520 (0.371–0.670) | 0.598 (0.440–0.756) | ||||
| t2 | ||||||
| Mean | 0.70±0.33 | 0.61±0.27 | 0.64±0.29 | 33±6.02 | 36.51±9.96 | 35.47±9.07 |
| AUC | 0.585 (0.421–0.749) | 0.651 (0.510–0.791) | ||||
| t3 | ||||||
| Mean | 0.87±0.23 | 0.71±0.27 | 0.76±0.27 | 13.26±11.95 | 34.02±14.63 | 27.86±16.78 |
| AUC | 0.668 (0.530–0.806) | 0.874 (0.788–0.959) | ||||
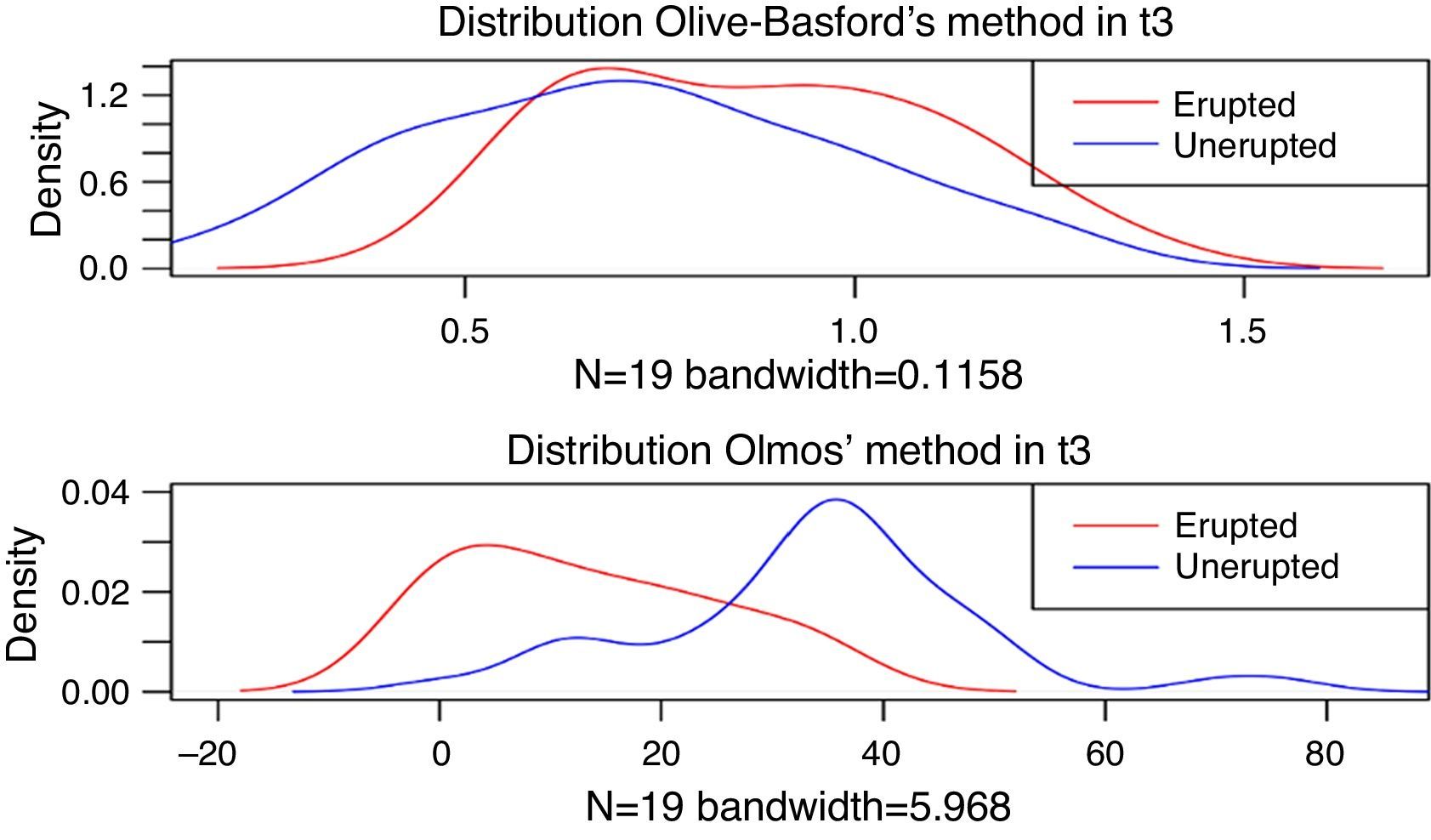
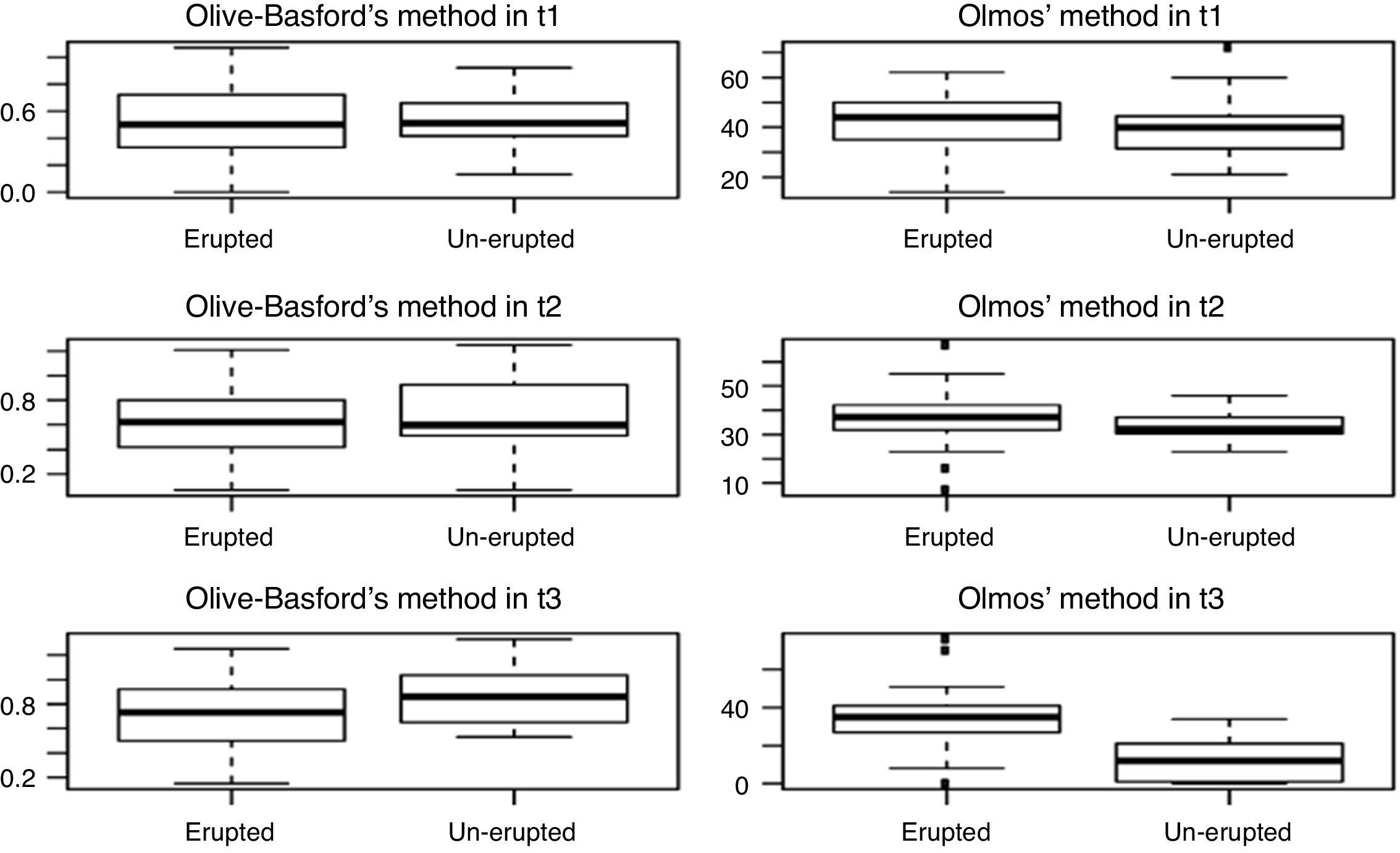
Although Olive-Basford's method reached higher values in erupted third molars than in un-erupted molars in all times, only statistical significant differences were registered between both groups in t3 (p<0.05). For Olmos’ method there were also differences in t3 (p<0.001) but in this case with lower values in the group of final erupted third molars (see Figs. 3–4).


The ROC curves for the two methods in each time, taking as gold standard the status of the third molar (erupted/un-erupted) at the end of the follow-up, are shown in Fig. 5. While in t1 and t2 the curves were more similar for both methods, in t3 differences were detected between the two curves, where the ROC curve of Olmos’ method always remained on top. This is also clearly reflected in terms of AUC.

The values of AUC for Olive-Basford's method in t1 and t2, and for Olmos’ method in t1 were not statistically significant (the 95% confidence intervals contain the 0.5 value in these cases). Moreover, although in t1 and t2, the AUC was slightly higher in the Olmos’ method, there were not statistically significant differences between the accuracy discrimination of both methods (p=0.483 and p=0.552, respectively). However, in t3, significant differences were detected (p<0.05), where the AUC for Olmos’ method was 0.874 (95% CI: 0.788–0.959) (see Table 2), showing a high discrimination capacity of the Olmos’ method in t3 (the AUC value is elevated, close to 1 in the 87% of the cases, the value of the Olmos’ method is higher for the erupted molar than for the un-erupted molar).
DiscussionThe eruption of the mandibular third molar is a complex multifactorial process because neither the eruption mechanism nor the contributors’ factors in the process are completely understood. The third molars are generally the last teeth to erupt into the arches and as a consequence they are also the most frequently impacted teeth. While many factors may affect the eruption of mandibular third molars, it has been established that the eruption of the third molar is primarily dependent upon the available space conditions at the posterior ends of the arch. Despite this apparently simple approach to planning tooth-extraction, the clinical controversy about asymptomatic third molar extraction and time of exodontia is still largely unresolved.
In previous studies, lateral cephalometric radiographs and rotational panoramic radiographs were used to estimate the presence of space for the third molar and they also were used to estimate the retromolar space/third molar crown width ratio to assess the third molar eruption.13,16,25–27 However, panoramic radiography yielded one of the most accurate estimations in this field19,27 and it is the most popular dental record for the clinician, since it has been a common research tool for assessing lower third molars for extraction.8,26 In this study, were selected panoramic radiographs because they are the usual radiological exploration modality for dental screening in dental clinic. The radiographs were obtained by a single experienced operator, in the same machine, which reduced possible error related to the radiographic technique. Despite the fact that they cause magnification and distortion of the image, panoramic radiographs allow the measurements of the angles and the consistency between measurements can be assessed if the device and the settings are the same.27,28 The distortion in the position of mandibular third molars on panoramic radiographs may influence the surgical planning; however, this does not invalidate it as the main tool for diagnosis of mandibular third molar.29
Initially many lower third molars have a mesial inclination but they progressively become more upright up to the age of 25 and the teeth may erupt normally, usually between the ages of 18 and 24.6,11 The eruption may be prevented by the lack of space, so they become impacted. It has been previously reported that the retromolar space and mesiodistal angulation of impacted tooth are the most important factors for the eruption of third molars.8,10,21 Therefore these variables that describe spaces between the anterior of the ramus and the distal of the mandibular second molar and tooth size seemed to be the primary contributors to be observed between the non-impaction and the impaction groups studied. Other authors observed that there was also a significant difference in retromolar space/third molar crown width ratio. In such cases, when the crown width is larger than the retromolar space, the impacted tooth should be removed surgically by tooth sectioning or root sectioning in order to remove less bone around the impacted tooth. For all these reasons we have considered to use two different methods with linear and angular measurements in this study. In a previous study was observed that facial growth pattern and root configurations did not affect third molar impaction while the retromolar space of third molar was significantly smaller in the impacted group. In addition, retromolar space/third molar crown width ratio was significantly smaller in the impacted group.30
The protocol study has not taken into account the sexual dimorphism because the third molars behave differently to the other teeth; mature and erupt earlier in female subjects. Some authors concluded that the right and left mandibular molars have the same pattern of development and emergence and over the age of 18, no relevant differences were observed between sexes.3,4
Clinical assessment through the use of reliable and simple predictive tools is essential for evaluating the eruption of the mandibular third molar. This study has been developed for analyzing the capacity of discrimination in prediction of the eruption of the third molar of two different methods on panoramic radiographs. In our study, the results of the Olive-Basford's method increased while the Olmos’ method decreased with time. This shows that, as expected, over time, the discriminatory power of both methods was increased, making it easier to detect the possible eruption of the third molar. The older patient age gets the better prediction in both methods because the time factor determines the evolution of the eruptive process. One of the strengths of the present study is that in t3 (time closest to the possible eruption of third molar) it is shown that there were significant differences (p<0.05), and the capacity of discrimination of Olmos’ method was significantly higher than Olive-Basford's method. So, the discrimination of Olmos’ method was significantly higher than Olive-Basford's method 6 years later. This clinically means that the Olmos’ method could be used as a good method for discriminate in t3 between erupted and unerupted ones in clinical practice.
Other strength of this study was the criterion for patient selection and monitoring protocol followed. In most studies, the criteria used for determination of eruption status were emergence of any portion of the crown through the oral mucosa. This can give misleading results because many of the mandibular third molars do not continue to erupt and remain impacted in a partially erupted position.
The findings have determined an easy clinically applicable method for identify the probability of eruption or uneruption of the mandibular third molar based on panoramic radiographic measurements. Although it could be critical to the number of patients, this is a follow-up study for 6 years in patients with mandibular third molars without orthodontic treatment and the material is suitable.
Moreover, the present results are in agreement with a previous one.17 When they compared the prognosis of third molar eruption assessed by three different cephalometric methods employed panoramic radiographs: the Olive's method, the Ganss’ method and Venta's method, they determined that the Olive's method results in over-prediction compared with the other methods. The authors concluded that the three methods were not found to be reliable or accurate. They suggest that the methods used are only suited to the racial characteristics of those populations from whom they were originally extrapolate (North American population, Northern Germans population or Finnish population) and they would be inappropriate for populations of mediterranean origin.17
In the present study, were compared two different predictive methods by the analysis of the retromolar space and the direction of eruption, factors that were considered the most important in the third molar eruption. So, the predictive methods selected should be tested on a higher number of teeth due to the small number of teeth erupted in t2 and the range of application could be extended to younger ages. The results of this study show that the Olmos’ method could be more robust for Galician population.
ConclusionThe Olmos’ method demonstrated utility in assessment of eruption prediction of third mandibular molars in clinical practice with patients previous orthodontic treatment.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.