




Suicide is an important public health problem, it represents one of the major causes of unnatural death, and there are many factors that affect the risk of suicidal behaviour. The present study analyzes the temporal and spatial variations of mortality by suicide in Spain and its relationship with gross domestic product (GDP) per capita.
Material and methodsA retrospective study was performed, in which deaths by suicide, sex and age group in 50 Spanish provinces between 2000 and 2012 were analysed. The annual trend of suicide mortality was assessed using Kendall's tau-b correlation coefficient. Seasonality and monthly and weekly behaviour were evaluated by performing the ANOVA test and the Bonferroni adjustment. Finally, the relationship between GDP per capita and suicide was studied.
ResultsBetween 2000 and 2012, 42,905 adult people died by suicide in Spain. The annual average incidence rate was 95 suicides per million population. The regions located in the south and in the northwest of the country registered the highest per capita mortality rates. There is a decreasing trend in mortality by suicide over the period studied (CC=–.744; P=.0004) in adults over the age of 64, and a seasonal behaviour was identified with summer maximum and autumn minimum values (f=.504; P<.0001). The regions with the highest GDP per capita showed the lowest mortality by suicide (r=–.645; P<.0001) and the relationship is stronger among older age groups.
ConclusionsMortality by suicide does not follow a homogenous geographical distribution in Spain. Mortality in men was higher than in women. Over the period of study, there has been a decrease in mortality by suicide in Spain in adults over the age of 64. The seasonal cycle of suicides and the inverse relationship with GDP per capita found in this study, provide information which may be used as a tool for developing prevention and intervention strategies.
El suicidio es un problema de salud pública, ya que representa una de las principales causas de muerte no natural. Hay múltiples factores que influyen en el riesgo de la conducta suicida. Este trabajo analiza la distribución geográfica del suicidio en España, el patrón temporal y la relación entre la tasa de suicidios y el producto interior bruto (PIB) per cápita en el país.
Material y métodosSe ha realizado un estudio retrospectivo en el que se han analizado las muertes por suicidio, por sexo y por grupos de edad, en las 50 provincias españolas entre 2000 y 2012. La tendencia anual de los suicidios se calculó mediante el coeficiente de correlación Tau b de Kendall, y se empleó el análisis de varianza (ANOVA) y el test de Bonferroni para evaluar las diferencias en la mortalidad a escala estacional, mensual y semanal. Finalmente, se evaluó la asociación entre el PIB per cápita y las muertes autoinflingidas en las provincias.
ResultadosEntre 2000 y 2012 fallecieron 42.905individuos de 15años de edad en adelante por suicidio en España. La tasa media anual de incidencia durante el periodo de estudio fue de 95suicidios/millón de habitantes. El sur y el noroeste de España acumularon las mayores tasas de mortalidad por esta causa. A escala global, en el país existió una tendencia descendente en las muertes por suicidio en personas de más de 64años (CC=–0,744; p=0,0004), y los suicidios siguieron un patrón estacional con máximos en verano y mínimos en otoño (f=0,504; p<0,0001); asimismo, se encontró una relación inversa entre el PIB per cápita y la tasa de suicidios de cada provincia (r=–0,645; p<0,0001), que se intensificó en los grupos poblacionales de mayor edad.
ConclusionesLos suicidios no siguen una distribución geográfica homogénea en el país y la tasa de suicidios en varones es muy superior a la tasa en mujeres. Existió un descenso en la tasa de suicidios en las personas de más de 64años, por lo que parece que las medidas de actuación tomadas en España estuvieran siendo efectivas. El patrón espacio-temporal encontrado, así como la relación con el PIB, sirven de base para en futuros estudios poder profundizar en los factores de riesgo asociados.
The worldwide suicide rate stands at 114 suicides/million inhabitants, and it is one of the main causes of death in general, and most especially non-natural death. Preventive measures are a public health priority.1
Depression, toxic habits and anxiety have been identified as some of the main risk factors in suicide attempts.2 However, the majority of studies agree that to understand suicidal behaviour it is necessary to include many variables: ones that are biological, psychological, social, economic and educational.3,4
Some authors have identified a seasonal pattern in suicides which varies depending on the geographical characteristics of each country and most especially the influence of the climate.5
Although Spain has traditionally had one of the lowest suicide rates in Europe, from 1975 to 1994 it increased pronouncedly. This was attributed to social factors that were especially linked to sex, as well as the AIDS epidemic and the epidemic of addiction to parentally administered drugs which occurred in the 1980s and 1990s.6
This study analyses the incidence and geographical distribution of suicide in Spain in the 13 years from 2000 to 2012, together with differences according to sex and age group, the time of year and the relationship between gross domestic product (GDP) and mortality due to this cause.
MethodologyData analysedThe National Statistics Institute (Instituto Nacional de Estadística) (INE) was asked to supply data on deaths due to intentional self-inflicted injuries. This Institute collects data from the Judicial Statistical Bulletin of Deaths (Boletín Estadístico de Defunción Judicial) (BEDJ).
Daily data were collected from each province, including the sex variable as well as the age group of the individual (15–44 years old, 45–64 years old or 65 years old and above).
The causes of death analysed in this work are those which are included in the tenth revision of the International Classification of Diseases (ICD-10) with codes from X60 to X84, i.e., deaths due to self-inflicted intentional injuries using physical means and poisoning.
Analysis of geographical distributionTo analyse the geographical distribution of deaths the mortality rate was first calculated for all of the provinces in Spain; the annual population data were collected for this per province, sex and age group (source: INE).
The rates were then standardised using the direct adjustment method.7
The population of the whole country in the year 2000 was selected as the reference population, thereby eliminating the distortion of the confusion factor that would arise due to the different population distribution in each location.
The average for the period was obtained based on these standardised annual rates.
The process was implemented by obtained a single value for intentional self-inflicted mortality for each province, sex and age group.
Map creation was the method selected to visually represent the standardised mortality rates. They were designed and created using the QGIS tool (an open code geographical information system [GIS]).
Analysis off the difference in mortality according to sex was undertaken by calculating the normalised rates ratio.
Analysis of behaviour over timeTo calculate the national tendency the gross annual rate was used, selecting Kendall's Tau-b correlation coefficient.
The average numbers of suicides per day in each season, month and day of the week were then calculated based on the daily series. Finally, variance analysis (ANOVA) and Bonferroni's test were used to evaluate whether the differences in self-inflicted deaths according to these variables were statistically significant.
Analysis of the relationship between economic factors and deathsStudy of the relationship between per capita GDP (data source: INE) and the normalised suicide rate was undertaken using Pearson's correlation coefficient after weighting the suicide rate with the logarithm of the population of each province. Data from 2000 to 2011 was used, as the GDP for these years was available. A single value of each variable per province was used for analysis of the relationship. The average over the 12 years of the study was calculated for the population and per capita GDP; in the case of the normalised suicide rate the median was calculated due to inter-annual differences. This analysis was then reproduced while introducing the age group variable.
ResultsGeographical distribution of suicides in Spain according to sex and age group42,905 individuals over the age of 15 years old died due to suicide in Spain from 2000 to 2012. The rate during the period studied was 95 suicides/million inhabitants.
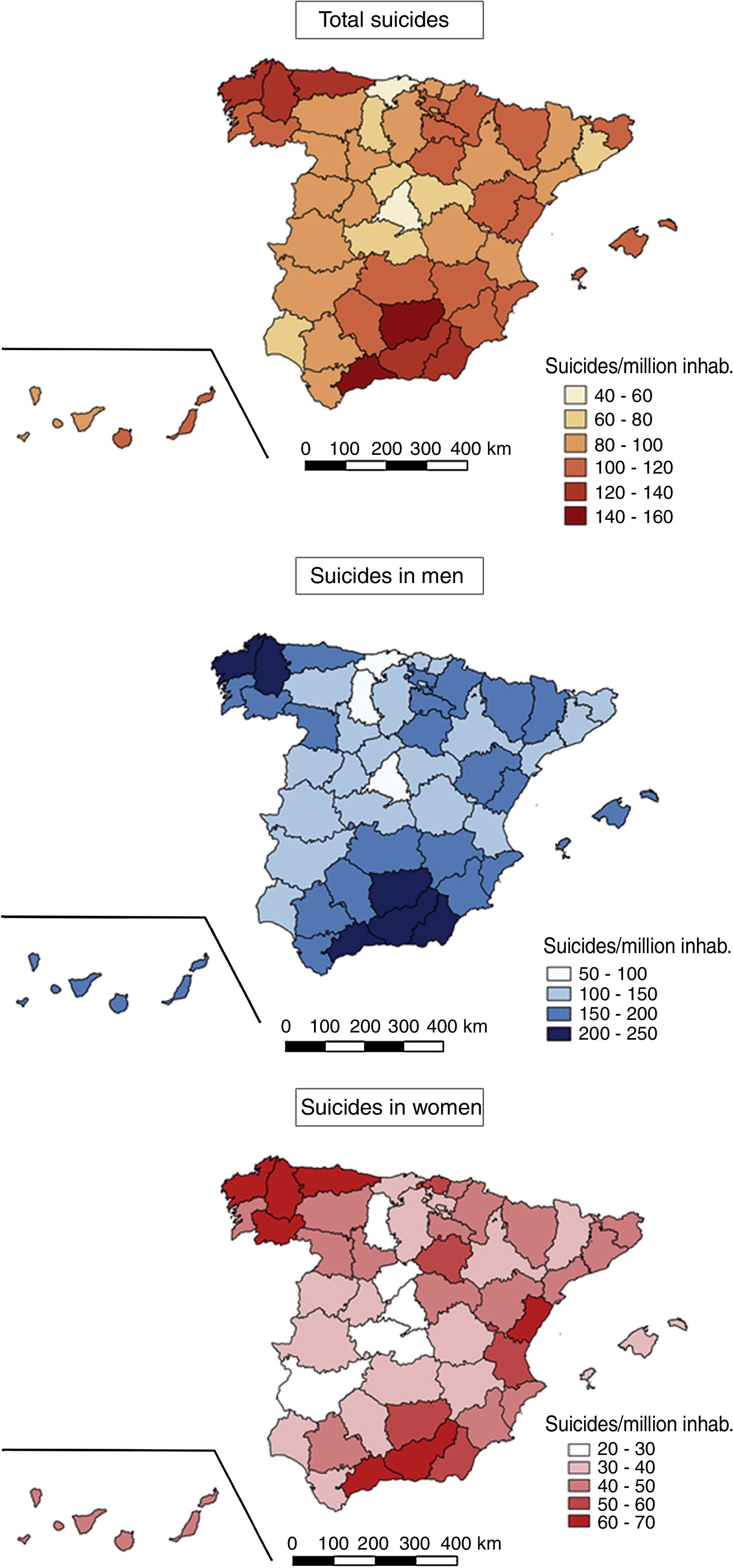
The geographical distribution was not homogeneous throughout the country; as can be seen in Fig. 1, the southern provinces and more specifically Malaga and Jaen had the highest rates, at 149.68 and 141.39 suicides/million inhab., respectively, followed by those in the north west of the Peninsular. The provinces with the lowest rates were the Community of Madrid, with 49.71 suicides/million inhabitants, and Cantabria with 55.51 suicides/million inhabitants.
. In descending order: the upper map shows total suicides, the one in the middle shows suicides in men and the lower map shows suicides in women.")
32,809 of the total number of intentional self-inflicted deaths corresponded to men, with a rate of incidence in those over the age of 14 years old of 150 suicides/million inhabitants, while 10,096 corresponded to women, with a rate of incidence of 44 suicides/million inhabitants.
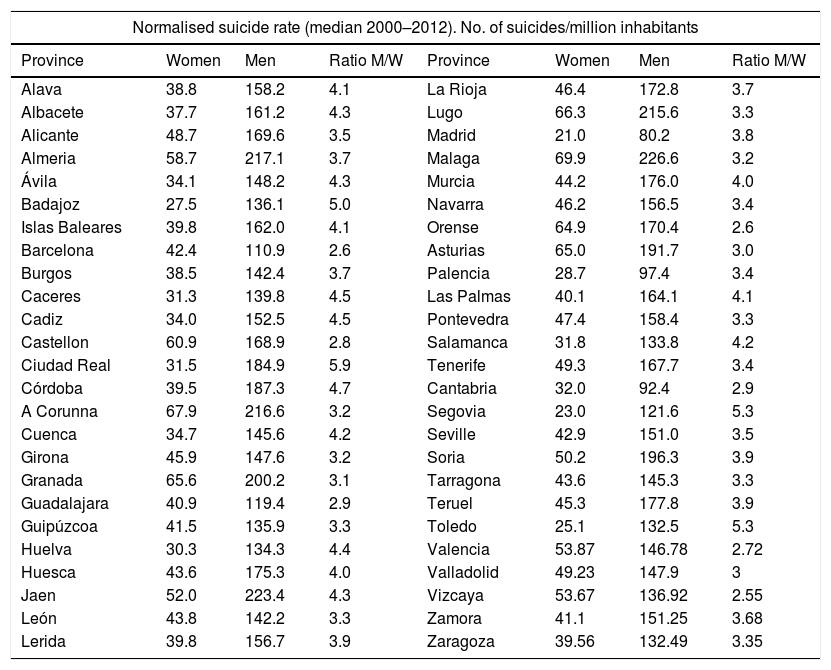
When provincial rates are compared according to sex (using the average of the normalised annual rates) this shows that the province with the smallest difference between the suicide rates of the sexes is Vizcaya, with 2.55 male suicides for each female one, while the greatest difference is in Ciudad Real, with 5.87 suicides in men for every suicide in women (Table 1).
Median normalised annual suicide rate per sex in Spanish provinces from 2000 to 2012.
| Normalised suicide rate (median 2000–2012). No. of suicides/million inhabitants | |||||||
|---|---|---|---|---|---|---|---|
| Province | Women | Men | Ratio M/W | Province | Women | Men | Ratio M/W |
| Alava | 38.8 | 158.2 | 4.1 | La Rioja | 46.4 | 172.8 | 3.7 |
| Albacete | 37.7 | 161.2 | 4.3 | Lugo | 66.3 | 215.6 | 3.3 |
| Alicante | 48.7 | 169.6 | 3.5 | Madrid | 21.0 | 80.2 | 3.8 |
| Almeria | 58.7 | 217.1 | 3.7 | Malaga | 69.9 | 226.6 | 3.2 |
| Ávila | 34.1 | 148.2 | 4.3 | Murcia | 44.2 | 176.0 | 4.0 |
| Badajoz | 27.5 | 136.1 | 5.0 | Navarra | 46.2 | 156.5 | 3.4 |
| Islas Baleares | 39.8 | 162.0 | 4.1 | Orense | 64.9 | 170.4 | 2.6 |
| Barcelona | 42.4 | 110.9 | 2.6 | Asturias | 65.0 | 191.7 | 3.0 |
| Burgos | 38.5 | 142.4 | 3.7 | Palencia | 28.7 | 97.4 | 3.4 |
| Caceres | 31.3 | 139.8 | 4.5 | Las Palmas | 40.1 | 164.1 | 4.1 |
| Cadiz | 34.0 | 152.5 | 4.5 | Pontevedra | 47.4 | 158.4 | 3.3 |
| Castellon | 60.9 | 168.9 | 2.8 | Salamanca | 31.8 | 133.8 | 4.2 |
| Ciudad Real | 31.5 | 184.9 | 5.9 | Tenerife | 49.3 | 167.7 | 3.4 |
| Córdoba | 39.5 | 187.3 | 4.7 | Cantabria | 32.0 | 92.4 | 2.9 |
| A Corunna | 67.9 | 216.6 | 3.2 | Segovia | 23.0 | 121.6 | 5.3 |
| Cuenca | 34.7 | 145.6 | 4.2 | Seville | 42.9 | 151.0 | 3.5 |
| Girona | 45.9 | 147.6 | 3.2 | Soria | 50.2 | 196.3 | 3.9 |
| Granada | 65.6 | 200.2 | 3.1 | Tarragona | 43.6 | 145.3 | 3.3 |
| Guadalajara | 40.9 | 119.4 | 2.9 | Teruel | 45.3 | 177.8 | 3.9 |
| Guipúzcoa | 41.5 | 135.9 | 3.3 | Toledo | 25.1 | 132.5 | 5.3 |
| Huelva | 30.3 | 134.3 | 4.4 | Valencia | 53.87 | 146.78 | 2.72 |
| Huesca | 43.6 | 175.3 | 4.0 | Valladolid | 49.23 | 147.9 | 3 |
| Jaen | 52.0 | 223.4 | 4.3 | Vizcaya | 53.67 | 136.92 | 2.55 |
| León | 43.8 | 142.2 | 3.3 | Zamora | 41.1 | 151.25 | 3.68 |
| Lerida | 39.8 | 156.7 | 3.9 | Zaragoza | 39.56 | 132.49 | 3.35 |
Ratio: median normalised annual rate in men/median normalised annual rate in women.
In age-group terms, in individuals aged from 15 to 44 years old the rate was 70 suicides/million inhabitants; in the 44–64 year old age-group the rate was 99 suicides/million inhabitants, and the highest rate was recorded for those aged over 64 years old, at 153 suicides/million inhabitants.
Behaviour over timeTendency analysisTendency analysis based on the gross annual rates in the country over the 13 years covered by the study shows that it is only statistically significant in over 64 year old age group, where moreover it is falling (Kendall Tau b=–.744; P=.0004).
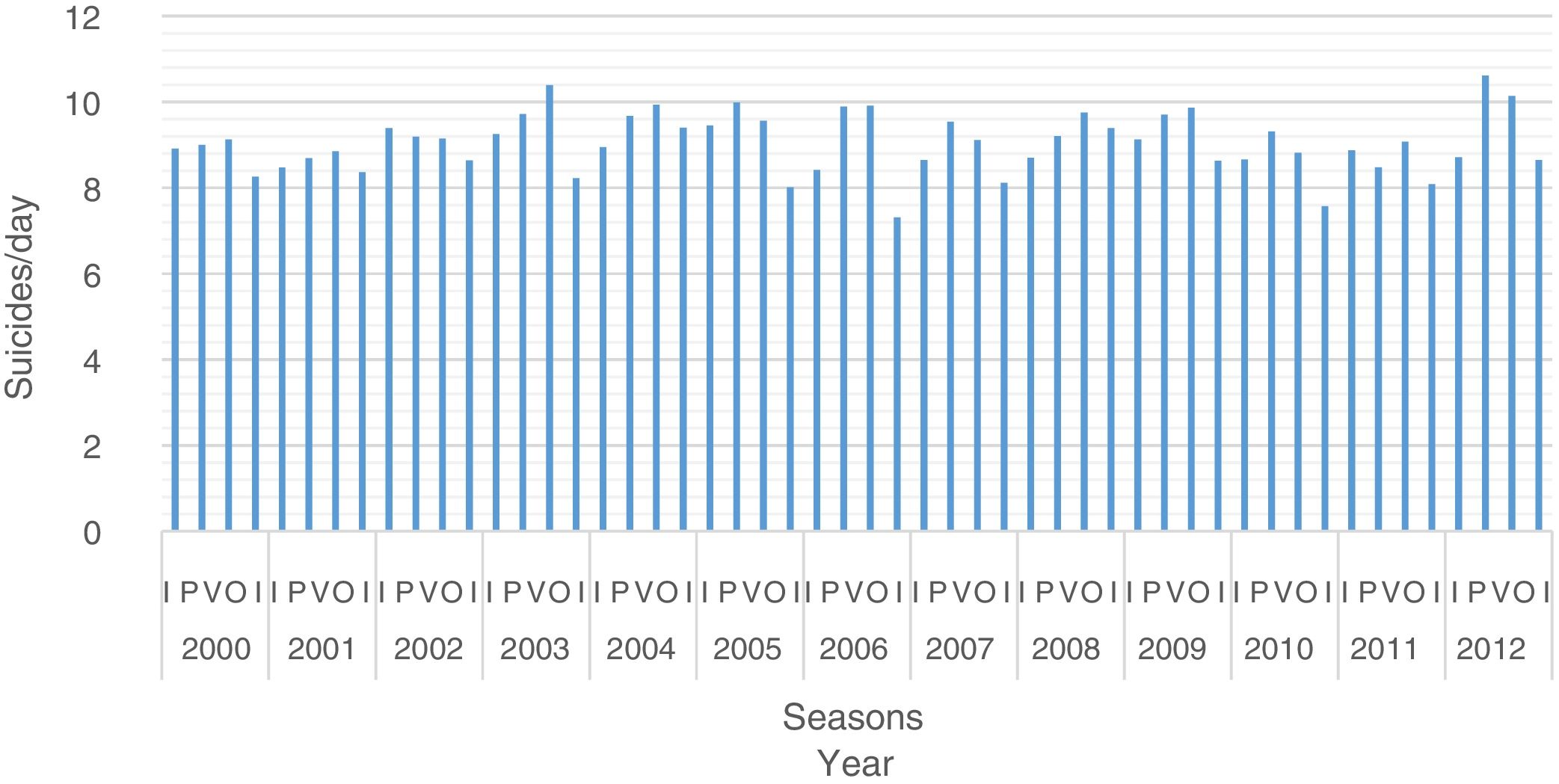
The seasonal, monthly and weekly patternSuicides in Spain are markedly seasonal (f=.504; P<.0001) (Fig. 2). Summer is the season with the highest average suicide rate, with 13.8% more suicides than the season with the fewest, autumn.

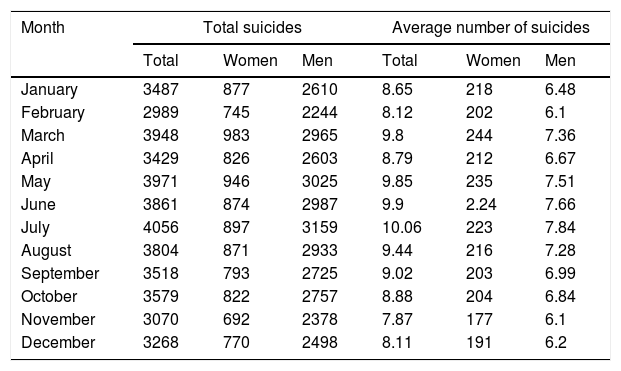
Statistically significant differences were also found at a monthly level (f=13.289; P<.0001), where July is the month with the highest number of suicides per day, with 27.9% more self-inflicted deaths than November, the month with the lowest average (Table 2).
Monthly series of suicides showing the total and overall average as well as according to sex.
| Month | Total suicides | Average number of suicides | ||||
|---|---|---|---|---|---|---|
| Total | Women | Men | Total | Women | Men | |
| January | 3487 | 877 | 2610 | 8.65 | 218 | 6.48 |
| February | 2989 | 745 | 2244 | 8.12 | 202 | 6.1 |
| March | 3948 | 983 | 2965 | 9.8 | 244 | 7.36 |
| April | 3429 | 826 | 2603 | 8.79 | 212 | 6.67 |
| May | 3971 | 946 | 3025 | 9.85 | 235 | 7.51 |
| June | 3861 | 874 | 2987 | 9.9 | 2.24 | 7.66 |
| July | 4056 | 897 | 3159 | 10.06 | 223 | 7.84 |
| August | 3804 | 871 | 2933 | 9.44 | 216 | 7.28 |
| September | 3518 | 793 | 2725 | 9.02 | 203 | 6.99 |
| October | 3579 | 822 | 2757 | 8.88 | 204 | 6.84 |
| November | 3070 | 692 | 2378 | 7.87 | 177 | 6.1 |
| December | 3268 | 770 | 2498 | 8.11 | 191 | 6.2 |
No statistically significant differences emerged when analysis was based on the day of the week (f=.504; P=.806) and this was also the case when weekends were compared to weekdays (from Monday to Friday) (f=.22; P=.882).
Study of behaviour over time according to sex showed that the seasonal pattern was also applicable to women (f=10.370; P<.0001). However, spring was the season with the highest average number of suicides, with 16.9% more deaths due to this cause than autumn (the season with the lowest average number). The differences were also significant at a monthly level (f=4.983; P<.0001). The maximum average number of deaths was attained in March, with 37.5% more suicides per day than the month with the lowest figure, November (Table 2). There were no differences in women according to the day of the week (f=.289; P=.943), and this was also the case when the weekend was compared to the other days (f=.003; P=.953).
The seasonal distribution of suicides also varied in men (f=18.934; P<.0001), where the highest average rate occurs in the summer, with 14.3% more intentional self-inflicted deaths than in autumn, the season with the lowest number of suicides/day. At a monthly level the maximum number occurred in July, with 28.6% more suicides/day than the month with the fewest, November. These differences are significant (f=12.165; P<.0001) (Table 2). No statistically significant differences were found between days of the week for men (f=.714; P=.638), and this was also the case when weekends were compared to the other days (f=.042; P=.838).
Relationship between gross domestic product (GDP) and suicidesA statistically significant inverse relationship was found between average provincial GDP and the median normalised suicide rate in the period studied, weighting the analysis according to the population of each province (r=–.645; P<.0001).
When the study is reproduced according to age group, although the statistically significant inverse relationship is still found in all 3 life-stages, as the age of the population rises the correlation coefficient increases (the correlation in young adults: r=–.376; P<.0001. In adults aged 45–64 years old: r=–.647; P<.0001. In adults aged 65 years old and over: r=–.661; P<.0001).
DiscussionThe main findings of this study are: (i) that suicides are not distributed homogeneously throughout the country; (ii) that analysis of the pattern of suicides over time reveals that there is a decline in the tendency in individuals over 64 years old in Spain, and that deaths due to this cause follow a seasonal pattern (peaking in summer), and that (iii) per capita GDP is inversely associated with the suicide rate in each province, and this association intensifies in the older population.
The high prevalence found in the south of Spain has been described by other authors in works using data from previous years,8 so that the geographical pattern presented here seems to be constant within the country. The higher rates of unemployment and lower level of life in this area were the main causes attributed to this higher rate; the inverse relationship with GDP shown in the results would also support this reason.9,10
As is the case in other Western countries, in Spain suicide rates are higher for men than they are for women. Some of the risk factors identified in men are: unskilled manual work, unpaid work, low income and unemployment; on the other hand, maternity has been described as a protective factor in women. The difference in the number of suicides committed according to sex may be due to the greater lethality of the methods used by men, as described in the study published by Mergl et al.11
The declining tendency found in adults aged over 64 years old may be explained by the cohort effect; when Chauvel et al. studied the variations in suicide rates over time in 25 countries, they found that in Spain there was a high mortality due to suicide in the cohorts born between 1965 and 1975, and that this fell with increasing age.12 On the other hand, the fall may be due to the effectiveness of preventive measures and the protocols developed over recent years. A recent review that analysed the efficacy of suicide prevention measures since 2005 found that access to lethal measures has been restricted. Most especially the sale of analgesics is now more strictly controlled, and safety precautions have been increased in “key” places for suicide by falling. Additionally, awareness-raising programmes have been developed in schools, while there have been notable advances in psychological and pharmacological treatments for some illnesses that give rise to risk, such as depression.13
Nevertheless, given the association described between suicides and GDP, it would be expectable for the tendency to increase due to the economic crisis. This was detected in other countries such as Greece,14 and it was even also found in a study in the Autonomous Community of Andalusia in Spain. The latter found an increase in suicides among adults aged from 35 to 54 years old, and the authors attributed this to higher rates of unemployment associated with economic decline.9 At this level our results agree with those of Iglesias-García et al., who underline that unemployment is associated with suicide during times of economic stability but not during periods of crisis.15 One of the limitations of our study has to be pointed out here: although the broader period of study made it possible to better analyse the effects of the economic crisis, given that in many cases they were experienced by the population after 2012, the years included in the analysis were delimited by the available mortality data and the way they were collected. After 2013 the INE had access to Madrid Anatomical Forensic Institute data, which led to a methodological change in the process of preparing statistics. This gave rise to changes in certain aspects of how cause of death is assigned in cases of judicial intervention after death. As a result of this, deaths which had been assigned to poorly defined causes were re-assigned to specific external causes; this means that data from the years after 2012 should not be compared with those from previous years.
On the other hand, another limitation of this study should also be mentioned. This refers to the origin of the suicide data: to perform a study of the whole country and covering several years, the INE is a priori the most suitable source, given that it is able to supply data that has been uniformly processed from a single source (the BEDJ). Moreover, the number of deaths due to suicide should coincide with the number of those “diagnosed” in the Legal Medicine Institutes (IML). Nevertheless, an analysis undertaken in several Spanish provinces showed that there were differences between the data recorded by the Institutes and those which finally reached the BEDJ. Although it is to be expected that the error will be similar all over the country, for data to be comparable we think it is important to include this result of the analysis by Guija et al. in the discussion16 and state that the cause of these differences has to be discovered.
Finally, the seasonal pattern and temporal differences depending on sex have also been detected in other parts of the world, in the northern and southern hemispheres.17–19 This indicates that environmental variables are involved in suicidal behaviour.
Although the descriptive results shown in this paper do not make it possible to identify causal variables, they do form a basis that makes it possible to formulate hypotheses so that future studies will be able to identify risk factors. The results also show the need to intensify preventive measures against suicide at certain times of the year.
Ethical disclousresProtection of people and animalsThe authors declare that no experiments took place on human beings or animals for this research.
Data confidentialityThe authors declare that no patient data are shown in this paper.
Right to privacy and informed consentThe authors declare that no patient data are shown in this paper.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Santurtún M, Santurtún A, Zarrabeitia MT. ¿Afecta el medio a los suicidios que se cometen en España? Análisis descriptivo del patrón temporoespacial. Rev Psiquiatr Salud Ment (Barc). 2018;11:192–198.