




The prevalence and expression of Cluster B personality disorders during adolescence have been poorly analysed. The main aim of this research was to analyse the rate of Cluster B maladaptive personality traits in Spanish adolescents. We also examined dimensional structure underlying the influence of sex and age in its phenotypic expression, was also examined.
MethodThe sample consisted of a total of 1440 participants (mean=15.9 years, SD=1.2). The self-reporting questionnaire used was the Personality Diagnostic Questionnaire-4+ (PDQ-4+).
ResultsMaladaptative «dramatic» or «erratic» personality traits are common among adolescents, particularly antisocial and borderline facets. Using the PDQ-4+ cut-off points, 20.3% of the sample submitted had a Cluster B personality disorder. The analysis of the internal structure of the Cluster B items of the PDQ-4+ yielded a factorial solution centred on three interrelated factors, including: Antisocial, Borderline and Histrionic/Narcissistic. There were differences by gender in the subscales of Cluster B, but not in function of age.
ConclusionsThese data yield new insights that improve the understanding of the Cluster B personality disorders and traits in this sector of the population. Future studies should use measurement tools that take into account the concern, conviction and distress associated with such experiences.
La prevalencia y la expresión de los trastornos de la personalidad del cluster B durante la adolescencia han sido escasamente analizadas. El objetivo de esta investigación fue analizar la tasa de los rasgos y los patrones desadaptativos de la personalidad del cluster B autoinformados en adolescentes españoles. También se examinaron la estructura dimensional subyacente y la influencia del sexo y la edad en su expresión fenotípica.
MetodoLa muestra la formaron un total de 1.440 participantes (media=15,9 años; DE=1,2). El instrumento de medida utilizado fue el Personality Diagnostic Questionnaire-4+ (PDQ-4+).
ResultadosLos rasgos de las personalidades «dramáticas» o «erráticas» son comunes entre la población adolescente, particularmente las facetas antisocial y límite. El 20,3% de la muestra presentaría, según los puntos de corte del PDQ-4+, un patrón desadaptivo de la personalidad del cluster B. El análisis de la estructura interna de los ítems del cluster B del PDQ-4+ arrojó una solución factorial concretada en 3 factores interrelacionados, a saber: Antisocial, Borderline e Histriónico/Narcisista. Se encontraron diferencias en función del sexo en la subescalas del cluster B, no así en función de la edad.
ConclusionesEstos datos arrojan nuevas pistas que permiten mejorar la comprensión de los rasgos de la personalidad del cluster B en este sector de la población. Futuros estudios deberían utilizar instrumentos de medida que tuvieran en cuenta la preocupación, la convicción y el estrés asociado a tales experiencias.
The study of disorders and maladaptive personality traits during adolescence has recently increased because of the need to integrate the perspective of developmental psychopathology and the dimensional model of personality in the same framework.1–4 Adolescence is a period of human development in which a wide variety of psychopathological disorders and symptoms can occur,5–7 among which maladaptive personality patterns stand out.8–10 Many of the personality disorders (PD) that appear in adults seem to organise themselves and have their etiological roots in earlier developmental stages,1,11,12 as the DSM-IV-TR13 establishes well for their diagnosis.
Diagnosing PD during adolescence and studying maladaptatives personality traits is a controversial subject that is being debated with interest. The DSM-IV-TR13 considers that PD can be diagnosed in individuals younger than 18 years old; however, they are relatively rare cases, in which the maladaptive personality traits tend to expand, to persist and not to be limited to a particular developmental stage, and they last less than a year. There is a growing body of scientific knowledge that reveals the need to assess maladaptive personality traits in the adolescent population.11 PD have been diagnosed in adolescentes in the general population,10,14,15 as well as in our centres.16–18 Prevalence rates for PD in non-clinical adolescentes are elevated, ranging from 14.4% to 17%.10,14,19 Likewise, PD traits or PD diagnosed in this developmental stage clearly affect adulthood (early and late) at work, interpersonal and social levels, as well as impacting mental and physical health (suicide attempts, substance abuse, depression, etc.).20–23 These data emphasise the need to assess and understand the expression of maladaptive personality traits in this sector of the population, to establish strategies for prevention, intervention and resource management.
Cluster B PD groups together a set of «dramático» or «erratic» syndromes, which the DSM-IV-TR13 classifies as individuals that are excessively extroverted, emotional, impulsive and unstable (that is to say, immature personalities). These include the antisocial, borderline, narcissistic and histrionic personality disorders.13 This set of disorders has been analysed extensively, although it is true that the antisocial and borderline disorders have received comparatively greater attention in the literature to date,24,25 and specifically during adolescence.26–28 This grouping is based on previous work carried out with factor and cluster analysis studies13,17,29,30; nevertheless, genetic studies have found greater association between antisocial and borderline PD31 than among the other PD. Likewise, Asimismo, from the dimensional personality models, PD traits (such as, for example, those of the borderline personality) can be found in the general population, distributed throughout a continuum of severity and without necessarily being associated with stress, worry, incapacity and/or need of treatment. From this dimensional perspective, PD traits are considered as a variation or extreme and maladaptive expression of normal personality traits.32,33 Epidemiological studies on non-clinical adolescent and adult populations using instruments that assess Cluster B personality traits run in this line.15,34,35 Specifically, the prevalence of Cluster B PD in non-clinical adolescentes is estimated to be on the order of 0.9–7.1%,10,19,36 with higher rates for clinical adolescent samples.18,37
As the studies indicate, both in community samples of adolescents and adult as well as in the clinical populations, the phenotype expression of PD and of their traits seem to vary depending on sex and/or age.38–40 In the adult population specifically, it has been found that, within Cluster B personality disorder, the borderline and histrionic types seem to exist among women39,41,42; in general, other studies have found higher prevalence of Cluster B in men,43 or do not replicate these findings.44 In adolescent populations, higher rates of borderline PD have been found in women15,35,40 and greater frequency of behaviour disorder in men.45–47 However–and just as happens with adults–other studies did not find this association.10 As for age, the youngest participants usually show higher scores in the PD when compared with those who are older. Analysing Cluster B PD traits longitudinally, prevalence can be seen to decrease with age and mean scores decrease from adolescence to adulthood.10,44,48
To date there have been few emperical studies that try to analyse and understand the prevalence and expression of Cluster B personality traits in the Spanish general adolescent population general to shed new light on these contradictory results. Within this research context, the objective of this study was to examine the prevalence rates of maladaptative Cluster B personality patterns and traits in a representative sample of Spanish adolescents using the Personality Diagnostic Questionnaire-4+ (PDQ-4+).49 Likewise, we examined the dimensional structure underlying this group of «dramátic» or «errátic» traits, as well as the influence of sex and age the expression of Cluster B maladaptive personality traits.
MethodParticipantsThe adolescents were selected using a stratified random classroom sampling, by clusters, in an approximate initial population of 36,000 students in the autonomous community of Principado de Asturias (a region in northern Spain). The layers were created on the basis of the geographical area (East, West and Central) and school level (obligatory and post-obligatory). The selection probability of each centre was directly proportional to the number of students corresponding to it. The adolescents belonged to different school centres: state, state-subsidised private and private, for secondary education and vocational training cycles. The initial sample consisted of 1,628 students; however, we eliminated participants who presented: (1) more than 2 points on the Oviedo Infrequency Scale (n=64); (2) learning difficulties (n=6); (3) age over 18 years (n=35); (4) ommision of demographic data or unanswered questionnaires (n=32); and (5) outlier scores (n=51). A total of 1440 students comprised the final sample, 695 male (48.3%) and 745 (51.7%) female, from 28 school centres and 90 classrooms. Mean age was 15.91 years (standard deviation [SD]=1.18), ranging between 14 and 18 years of age. Sample distribution based on age was as follows: 14 years (n=193; 13.3%), 15 years (n=352; 24.4%), 16 (n=408; 28.3%) years, 17 years (n=352; 24.4%) and 18 years (n=135; 9.4%).
InstrumentsThe PDQ-4+49 is a self-report developed to assess personality disorder traits as a function of the DSM-IV criteria.50 The PDQ-4+ consists of 99 items distributed along 12 subscales, 10 referring to the diagnostic categories included by the DSM-IV on axis II and another 2 to assess categories of PD appearing in Appendix B. In this study we used a 5-category Likert response format (1 «completely disagree»; 5 «completely agree»). Using a Likert response format improves score reliability and favours obtaining valid evidence51,52; likewise, a dimensional score in psychopathology substancially betters the validity and reliability of the measurement.53 For the present study, we used the 34 items that assessed the antisocial, borderline, histrionic and narcissistic subscales. It should be mentioned that PDQ-4+ Items 98 and 99, which form part of the borderline and antisocial subscales, have a different response scale. In these items, the participants have to make a cross mark or tick to choose from among a group of impulsive (drink excessively, spend money, etc.) and/or criminal (fighting, cruelty, etc.) behaviours. If there are more than 2 behaviours on Item 98 or more than 3 on Item 99, that item is considered as positive. For that reason, these 2 items were presented in a dichotomous format (0–1) in this study. Item 33, which referred to «problems in paying bills from not remaining a long time at work», was changed to «problems in paying for my things because I don’t manage well the money I get for my allowance». The PDQ-4+ has been used in a wide variety of epidemiological studies and its properties are widely accepted.9,54–56 In our study, we used the version adapted to Spanish by Calvo et al57 for young adults, which has also been used with psychiatric out-patient patients58 and non-clinical adolescents.59
The Oviedo Infrequency Scale60 is a self-report made up of 12 items in Likert-type format of 5 categories (1 «completely disagree»; 5 «completely agree») developed following test construction directives.61 Its goal is to detect the participants that respond in a random, pseudo-random or dishonest way on self-reports (it includes items such as for example, «The distance between Madrid and Barcelona is greater than that between Madrid and NewYork»). This measurement instrument has been used in previous studies on adolescents.62 Once the items were dichotomised, the students who presented a score equal to or more than 2 points were automatically eliminated from the study.
ProcedureThe questionnaires were administered collectively, in groups of 10–35 students, during school hours and in a classroom set up for the purpose. The study was presented to the participants as an investigation into the various characteristics of personality, guaranteeing them that their replies were confidential and that their participation was voluntary. The adolescents did not receive any incentives for their participation. The tests were administered under the supervision of a collaborator at all times. This study falls within the framework of a larger investigation on early detection and intervention of psychological disorders in adolescence. The study was approved by the ethics committee at the University of Oviedo and the Department of Education in the Principado de Asturias.
Data analysisFirst of all, the descriptive statistics were calculated for the items making up the Cluster B subscales on the PDQ-4+. In this study, we used a 5-point Likert response format, in contrast to previous studies that used a dichotomous format (True/False). To compare our data with previous studies, descriptive statistics were also obtained dichotomising the item responses, considering the values of 1–3 as «0» and the values of 4–5 as «1». Secondly, we examined the internal structure of the 34 items that make up the 4 subscales on the PDQ-4+ Cluster B using an exploratory factor analysis. The minimun rank factor analysis and Promax rotation methods were used. Factor loads were estimated from the Pearson correlation matrix. The procedure to determine the number of dimensions was the optimal implementation of parallel analysis.63 Next, we compared the mean scores of the Cluster B subscales as a function of sex and age. To do so, we performed a multivariate analysis of variance (MANOVA), taking age and sex as set factors, and the PDQ-4+ Cluster B subscales and total score as dependent variables. Just as with the study at item level, the subscale scores were calculated considering the Likert nature of the variables and dichotomising the items. We used the Wilks λ value to observe whether there were statistically significant differences among all the dependent variables taken as a group. As an index of the size of the effect, we used the partial eta-squared (η2 partial) statistic. The statistical programme SPSS 15.064 and the programme FACTOR 8.0 were used for the data analysis.65
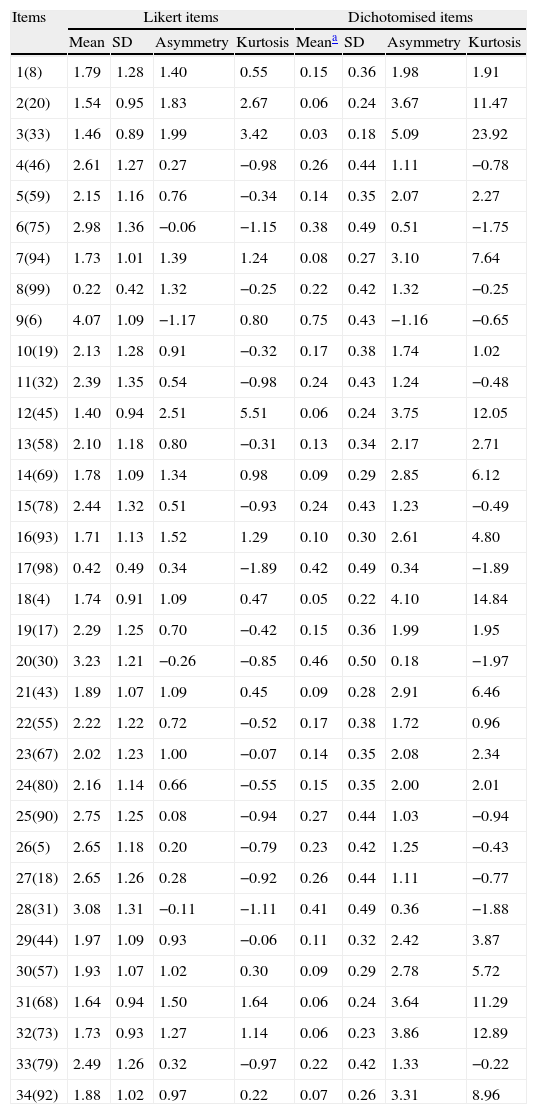
ResultsDescriptive statisticsIn Table 1, the descriptive statistics for the items on the antisocial, borderline, histrionic and narcissistic subscales are collected, both for the items in Likert format and once dichotomised. Parting from the dichotomised items, if the value of the table is multiplied by 100, you obtain the percentage of participants in the total sample that answered affirmatively for a specific trait. For example, 75% of the sample responded affirmatively to Item 9 («I would do whatever it takes to keep those I love from abandoning me»), while 46% responded positively to Item 20 («I show my emotions easily»). In contrast, approximately 3%-6% of the sample indicated «I have tried to harm myself or to commit suicide» (Item 2) or «Some people think that I take advantage of others» (Item 31).
Descriptive statistics for the Cluster B subscale items on the Personality Diagnostic Questionnaire-4+.
| Items | Likert items | Dichotomised items | ||||||
| Mean | SD | Asymmetry | Kurtosis | Meana | SD | Asymmetry | Kurtosis | |
| 1(8) | 1.79 | 1.28 | 1.40 | 0.55 | 0.15 | 0.36 | 1.98 | 1.91 |
| 2(20) | 1.54 | 0.95 | 1.83 | 2.67 | 0.06 | 0.24 | 3.67 | 11.47 |
| 3(33) | 1.46 | 0.89 | 1.99 | 3.42 | 0.03 | 0.18 | 5.09 | 23.92 |
| 4(46) | 2.61 | 1.27 | 0.27 | −0.98 | 0.26 | 0.44 | 1.11 | −0.78 |
| 5(59) | 2.15 | 1.16 | 0.76 | −0.34 | 0.14 | 0.35 | 2.07 | 2.27 |
| 6(75) | 2.98 | 1.36 | −0.06 | −1.15 | 0.38 | 0.49 | 0.51 | −1.75 |
| 7(94) | 1.73 | 1.01 | 1.39 | 1.24 | 0.08 | 0.27 | 3.10 | 7.64 |
| 8(99) | 0.22 | 0.42 | 1.32 | −0.25 | 0.22 | 0.42 | 1.32 | −0.25 |
| 9(6) | 4.07 | 1.09 | −1.17 | 0.80 | 0.75 | 0.43 | −1.16 | −0.65 |
| 10(19) | 2.13 | 1.28 | 0.91 | −0.32 | 0.17 | 0.38 | 1.74 | 1.02 |
| 11(32) | 2.39 | 1.35 | 0.54 | −0.98 | 0.24 | 0.43 | 1.24 | −0.48 |
| 12(45) | 1.40 | 0.94 | 2.51 | 5.51 | 0.06 | 0.24 | 3.75 | 12.05 |
| 13(58) | 2.10 | 1.18 | 0.80 | −0.31 | 0.13 | 0.34 | 2.17 | 2.71 |
| 14(69) | 1.78 | 1.09 | 1.34 | 0.98 | 0.09 | 0.29 | 2.85 | 6.12 |
| 15(78) | 2.44 | 1.32 | 0.51 | −0.93 | 0.24 | 0.43 | 1.23 | −0.49 |
| 16(93) | 1.71 | 1.13 | 1.52 | 1.29 | 0.10 | 0.30 | 2.61 | 4.80 |
| 17(98) | 0.42 | 0.49 | 0.34 | −1.89 | 0.42 | 0.49 | 0.34 | −1.89 |
| 18(4) | 1.74 | 0.91 | 1.09 | 0.47 | 0.05 | 0.22 | 4.10 | 14.84 |
| 19(17) | 2.29 | 1.25 | 0.70 | −0.42 | 0.15 | 0.36 | 1.99 | 1.95 |
| 20(30) | 3.23 | 1.21 | −0.26 | −0.85 | 0.46 | 0.50 | 0.18 | −1.97 |
| 21(43) | 1.89 | 1.07 | 1.09 | 0.45 | 0.09 | 0.28 | 2.91 | 6.46 |
| 22(55) | 2.22 | 1.22 | 0.72 | −0.52 | 0.17 | 0.38 | 1.72 | 0.96 |
| 23(67) | 2.02 | 1.23 | 1.00 | −0.07 | 0.14 | 0.35 | 2.08 | 2.34 |
| 24(80) | 2.16 | 1.14 | 0.66 | −0.55 | 0.15 | 0.35 | 2.00 | 2.01 |
| 25(90) | 2.75 | 1.25 | 0.08 | −0.94 | 0.27 | 0.44 | 1.03 | −0.94 |
| 26(5) | 2.65 | 1.18 | 0.20 | −0.79 | 0.23 | 0.42 | 1.25 | −0.43 |
| 27(18) | 2.65 | 1.26 | 0.28 | −0.92 | 0.26 | 0.44 | 1.11 | −0.77 |
| 28(31) | 3.08 | 1.31 | −0.11 | −1.11 | 0.41 | 0.49 | 0.36 | −1.88 |
| 29(44) | 1.97 | 1.09 | 0.93 | −0.06 | 0.11 | 0.32 | 2.42 | 3.87 |
| 30(57) | 1.93 | 1.07 | 1.02 | 0.30 | 0.09 | 0.29 | 2.78 | 5.72 |
| 31(68) | 1.64 | 0.94 | 1.50 | 1.64 | 0.06 | 0.24 | 3.64 | 11.29 |
| 32(73) | 1.73 | 0.93 | 1.27 | 1.14 | 0.06 | 0.23 | 3.86 | 12.89 |
| 33(79) | 2.49 | 1.26 | 0.32 | −0.97 | 0.22 | 0.42 | 1.33 | −0.22 |
| 34(92) | 1.88 | 1.02 | 0.97 | 0.22 | 0.07 | 0.26 | 3.31 | 8.96 |
The number in brackets indicates the item number corresponding to the Spanish versión of the Personality Diagnostic Questionnaire-4+.
According to the PDQ-4+ manual criteria, 20.3% (n=293) of the sample present a maladaptive pattern of Cluster B personality. A total of 9.1% (n=131) scored 4 (3+Item 99) or more on the antisocial subscale, while 10.3% (n=148) of the sample scored 5 or more on the borderline subscale. A total of 2.9% (n=42) of the participants scored 5 or more on the histrionic subscale, while 5.1% (n=74) of the sample did so on the narcissistic subscale. As for the number of possible maladaptive personality patterns, 14.9% (n=215) of the sample scored positively on a single pattern; 4.1% (n=59) on 2; 1% (n=14) on 3 and 0.3% (n=5) of the participants on the 4 patterns.
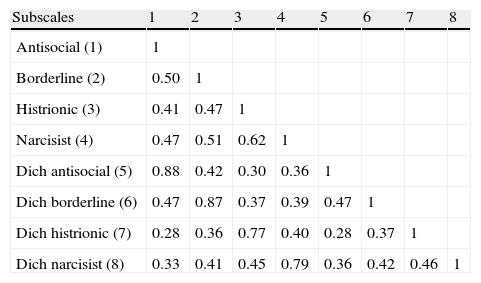
In Table 2, we present the Pearson correlations among the PDQ-4+ subscales, in the 2 response formats: (1) items in Likert format and (2) items in dichotomous format. In the first case, the correlacions among the subscales were high and statistically significant, ranging between 0.41 and 0.62. In the second case, the correlacions among the Cluster B subscales with dichotomous items ranged between 0.28 and 0.47, also being statistically significant. Likewise, the table makes it possible to see the degree of association between the scores with Likert and dichotomous format items.
Pearson correlations between the Cluster B subscales on the Personality Diagnostic Questionnaire-4+.
| Subscales | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| Antisocial (1) | 1 | |||||||
| Borderline (2) | 0.50 | 1 | ||||||
| Histrionic (3) | 0.41 | 0.47 | 1 | |||||
| Narcisist (4) | 0.47 | 0.51 | 0.62 | 1 | ||||
| Dich antisocial (5) | 0.88 | 0.42 | 0.30 | 0.36 | 1 | |||
| Dich borderline (6) | 0.47 | 0.87 | 0.37 | 0.39 | 0.47 | 1 | ||
| Dich histrionic (7) | 0.28 | 0.36 | 0.77 | 0.40 | 0.28 | 0.37 | 1 | |
| Dich narcisist (8) | 0.33 | 0.41 | 0.45 | 0.79 | 0.36 | 0.42 | 0.46 | 1 |
Dich: dichotimosed items.
All correlations are statistically significant: P≤.01.
Cronbach's alpha coefficient for the 34 items–Likert format–of the PDQ-4+ that made up the total score was 0.86, being 0.69, 0.67, 0.55 and 0.70 for the 4 antisocial, borderline, histrionic and narcissistic subscales respectively. Cronbach's alpha coefficient for the total score on the 34 items–dichotomised format–of the PDQ-4+ was 0.79, being 0.63, 0.55, 0.41 and 0.79 for the subscales respectively.
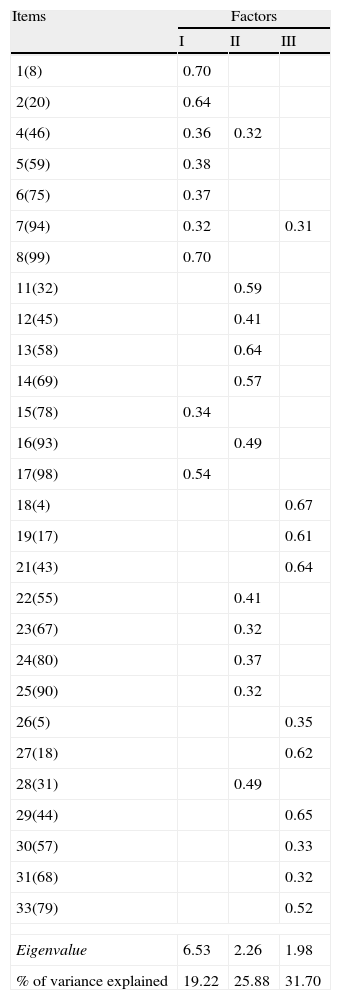
Evidence of internal structureNext, we carried out an exploratory factor analysis with the 34 items that make up the 3 subscales. The Bartlett spherical index was 10,396.3 (P<.001) and the Kaiser–Meyer–Olkin value was 0.89. In Table 3, the estimated factor loads, eigenvalue and percent of cumulative variance explained are shown. The optimal implementation of parallel analysis advised the extraction of 3 factors, which explained 31.70% of the total variance. The RMSR value was 0.042, the CFI was 0.99 and Bentler's simplicity index was 0.97. What is more, the resulting factors had a clear psychological interpretation. The first factor collects items related to behaviour, impulsiveness and legal problems, which is why this was called the antisocial factor. The second factor includes items related to borderline and histrionic facets (e.g., that only some people understand and appreciate the participant, the need for serious affective relationships, being easily influenced by others), so it was called the borderline factor. The third factor collects items related to the histrionic and narcissistic facets, so it was called the dramatic factor. The correlation between the factors ranged between 0.31 (FI–FII) and 0.42 (FII–FIII) (P<.01).
Exploratory factor analysis of the items on the Cluster B subscales on the Personality Diagnostic Questionnaire-4+.
| Items | Factors | ||
| I | II | III | |
| 1(8) | 0.70 | ||
| 2(20) | 0.64 | ||
| 4(46) | 0.36 | 0.32 | |
| 5(59) | 0.38 | ||
| 6(75) | 0.37 | ||
| 7(94) | 0.32 | 0.31 | |
| 8(99) | 0.70 | ||
| 11(32) | 0.59 | ||
| 12(45) | 0.41 | ||
| 13(58) | 0.64 | ||
| 14(69) | 0.57 | ||
| 15(78) | 0.34 | ||
| 16(93) | 0.49 | ||
| 17(98) | 0.54 | ||
| 18(4) | 0.67 | ||
| 19(17) | 0.61 | ||
| 21(43) | 0.64 | ||
| 22(55) | 0.41 | ||
| 23(67) | 0.32 | ||
| 24(80) | 0.37 | ||
| 25(90) | 0.32 | ||
| 26(5) | 0.35 | ||
| 27(18) | 0.62 | ||
| 28(31) | 0.49 | ||
| 29(44) | 0.65 | ||
| 30(57) | 0.33 | ||
| 31(68) | 0.32 | ||
| 33(79) | 0.52 | ||
| Eigenvalue | 6.53 | 2.26 | 1.98 |
| % of variance explained | 19.22 | 25.88 | 31.70 |
Factor loads less than 0.30 have been omitted. Items 3, 9, 10, 20, 23 and 34 have been eliminated. The number in brackets indicates the item number corresponding to the Spanish versión of the Personality Diagnostic Questionnaire-4+.
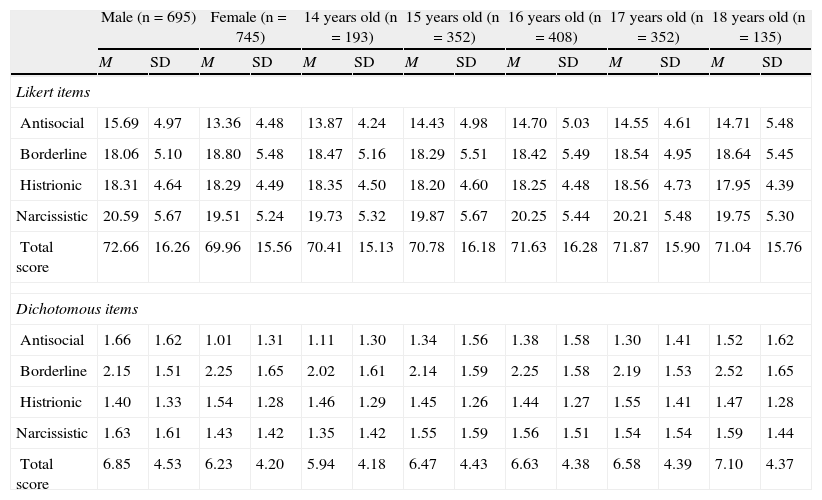
In Table 4, we present the means and SD on the subscales and the total score on the PDQ-4+ Cluster B by sex for the 5 age groups. Considering the score parting from the Likert format items, the Wilks λ value revealed that there were statistically significant differences as a function of sex (Wilks λ=0.898; P<.001), but not as a function of age (Wilks λ=0.993; P=.842). In relation to sex, statistically significant differences were found on the antisocial (F=79.56; P<.001; partial η2=0.053), borderline (F=4.92, P=.027; partial η2=0.003) and narcissistic subscales (F=10.74; P=.001: partial η2=0.007), as well as on the total Cluster B score (F=8.78; P=.003; partial η2=0.006). In the case of the antisocial and narcissistic subscales and the total score for Cluster B, boys presented higher mean scores than girls. No statistically significant interactions were found between the sex and age factors. Considering the score parting from the dichotomised items, the Wilks λ value revealed the presence of statistically significant differences in the sex factor (Wilks λ=0.931; P<.001), but not in the age factor (Wilks λ=0.992; P=.483). Males obtained higher mean scores than females in the antisocial (F=62.081; P<.001; partial η2=0.042) and narcissistic (F=7.489; P=.006; partial η2=0.005) subscales and on the total Cluster B score (F=7.827; P=.005; partial η2=0.005). Just as in the previous case, no statistically significant interactions between sex and age were found. Finally, when we compared the influence of sex and/or age on the type or number of PD presented, there were no statistically significant differences.
Comparisons of the mean subscale scores and the total cluster B score on the Diagnostic Questionnaire-4+ based on sex and age.
| Male (n=695) | Female (n=745) | 14 years old (n=193) | 15 years old (n=352) | 16 years old (n=408) | 17 years old (n=352) | 18 years old (n=135) | ||||||||
| M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | |
| Likert items | ||||||||||||||
| Antisocial | 15.69 | 4.97 | 13.36 | 4.48 | 13.87 | 4.24 | 14.43 | 4.98 | 14.70 | 5.03 | 14.55 | 4.61 | 14.71 | 5.48 |
| Borderline | 18.06 | 5.10 | 18.80 | 5.48 | 18.47 | 5.16 | 18.29 | 5.51 | 18.42 | 5.49 | 18.54 | 4.95 | 18.64 | 5.45 |
| Histrionic | 18.31 | 4.64 | 18.29 | 4.49 | 18.35 | 4.50 | 18.20 | 4.60 | 18.25 | 4.48 | 18.56 | 4.73 | 17.95 | 4.39 |
| Narcissistic | 20.59 | 5.67 | 19.51 | 5.24 | 19.73 | 5.32 | 19.87 | 5.67 | 20.25 | 5.44 | 20.21 | 5.48 | 19.75 | 5.30 |
| Total score | 72.66 | 16.26 | 69.96 | 15.56 | 70.41 | 15.13 | 70.78 | 16.18 | 71.63 | 16.28 | 71.87 | 15.90 | 71.04 | 15.76 |
| Dichotomous items | ||||||||||||||
| Antisocial | 1.66 | 1.62 | 1.01 | 1.31 | 1.11 | 1.30 | 1.34 | 1.56 | 1.38 | 1.58 | 1.30 | 1.41 | 1.52 | 1.62 |
| Borderline | 2.15 | 1.51 | 2.25 | 1.65 | 2.02 | 1.61 | 2.14 | 1.59 | 2.25 | 1.58 | 2.19 | 1.53 | 2.52 | 1.65 |
| Histrionic | 1.40 | 1.33 | 1.54 | 1.28 | 1.46 | 1.29 | 1.45 | 1.26 | 1.44 | 1.27 | 1.55 | 1.41 | 1.47 | 1.28 |
| Narcissistic | 1.63 | 1.61 | 1.43 | 1.42 | 1.35 | 1.42 | 1.55 | 1.59 | 1.56 | 1.51 | 1.54 | 1.54 | 1.59 | 1.44 |
| Total score | 6.85 | 4.53 | 6.23 | 4.20 | 5.94 | 4.18 | 6.47 | 4.43 | 6.63 | 4.38 | 6.58 | 4.39 | 7.10 | 4.37 |
M: mean; SD: standard deviation.
The prevalence and expression of the traits in maladaptive Cluster B personality patterns during adolescence, specifically in Spanish populations, are rarely analysed and scarily understood. The objective of our research was to analyse the maladaptive traits and patterns of the Cluster B personality in a representative sample of non-clinical Spanish adolescents. In addition, we examined the underlying dimensional structure and the influence of sex and age on phenotypical expression. The meansurement instrument used was the PDQ-4+.49 These objectives attempted to find new empirical evidence on the distribution and expression of maladaptive Cluster B personality traits in the Spanish adolescent population. In addition, the data obtained on the prevalence and dimensional structure of these traits could be of interest in advancing in early detection of adolescents at risk of developing a maladaptative personality pattern.
The results showed that «dramatic» personality traits are common among the adolescent population. A total of 20.3% of the sample presented, according to the PDQ-4+ manual, maladaptive Cluster B personality pattern, ranging between 2.9% and 10.3% for the specific syndromes. The most frequents patterns were the antisocial and the borderline. With respect to this result, we should mention that diagnosis of a PD cannot be based exclusively on the results from a single test. The PDQ-4+ is a short questionnaire for detection, that provides the clinician rapid information on which personality disorder(s) is probably present and, after that, a more in depth assessment would allow the diagnosis to be confirmed or ruled out. In addition, it should be remembered that overdiagnosis is relatively frequent when measurement instruments of the self-report type are administered for assessing PD.66
Bearing these considerations in mind, we wish to mention first that the rates of self-reported Cluster B personality PD traits found in this study are similar to those found in previous ones. For example, Zanarini et al.35 in a study carried out with 6330 11-year-old students, found that a percentage of these students, even without being diagnosed with PD, reported some borderline PD criterion of the DSM-IV.50 These data underscore, in the line of this study, that maladaptive personality traits are fairly frequent in this sector of the population, and that they can be found present in the general population distributed along a continuum of severity.32,33 Secondly, the rates of possible maladaptive patterns found in this study are similar to those reported in previous studies carried out in both adolescent populations10,14,19 and in community samples.41–43 Without going any further, the prevalence rates of PD in non-clinical adolescents range between 14.4% and 17%, with the specific estimated prevalence for the Cluster B PD being on the order of 0.9%-7.1%.10,19,36 It is worthwhile mentioning that the narcissistic and histrionic PD have rarely been analysed in samples of adolescents from the general population. In this study, the rates found for the 2 patterns are similar to those reported by Bernstein et al.10 and Johnson et al.14 For example, Bernstein et al.10 found prevalence rates for narcissistic and histrionic PD of 4.1%/5.3% and 6.0%/8.7%, respectively. Johnson et al.14 found specific prevalence rates of 3.2% and 1.6% respectively. In this sense, and although the samples and measurement instruments used in the studies are different, the data appear to point towards a convergence in epidemiological rates.
As it can be seen, an elevated percent of adolescents could present a maladaptive personality pattern, possibily causing a clear impact on not only personal, academic, family and social realms, but also at economic and health levels.20,67 What is more, many mental disorders have their beginnings in childhood and/or adolescence–approximately 50% have an onset before 15 year–and, in many cases, this symptomatology remains stable until adulthood.12,14,68,69 Likewise, it should be borne in mind that the presence of this type of symptom at an early age increases the later risk of developing a severe mental disorder in adulthood.9,22,70 That is why these data emphasise, without a doubt, the need to assess these psychopathological constructs early in the child-adolescent population. The objective for this is to prevent or delay the transition towards a clinical condition or mitigate the possible impact on multiple realms once it appears.
Analysis of the dimensional structure underlying the items on the antisocial, borderline, histrionic and narcissistic PDQ-4+ subscales revealed a possible 3-dimensional solution, specifically in the antisocial, borderline and histrionic/narcissistic factors. This result is difficult to compare with previous studies, given the nature and content of the measurement instrument used. It should be mentioned that the histrionic and narcissistic subscale items were grouped together under the same factor, while the items related to the affective and interpersonal relationships of the histrionic facet had weight in the borderline factor. These data partially support the validity of the internal structure proposed by the author of the PDQ-4+.49 It should also be borne in mind that the reliability of the PDQ-4+ subscale scores improved substantially because a 5-point Likert type response format was used. Consequently, in line with previous studies,51,52 we recommend future use of this format, as well as, in general, the construction of dimensional scores in other psychopathological measures.53
Participant gender influenced the expression of Cluster B personality traits, while age did not. As far as sex differences, males presented comparatively greater scores than females on the antisocial, histrionic and narcissistic subscales and on the total Cluster B score; male scores were especially high in the case of the antisocial facet, as the size of the effects show. Our females had a higher score than the males on borderline subscale, although it is true that these differences disappeared when a dichotomous response format was selected. Similar results were reached when the PD were examined in community population samples.38–40 For example, Samuels et al.43 found greater prevalence for Cluster B PD for men. Likewise, in the adult population it seems that antisocial or narcissistic types are more frequent among men, while borderline and histrionic types seem to be more frequent among women.39,41,42 In adolescent populations, higher PD rates have been found for females in borderline PD15,35,40 and higher rates of behaviour disorders found for males,45–47 although other studies have not found this association.10 On the other hand, we did not find any differences among the mean scores of the 5 age groups assessed. The absence of statistically significant age-based differences could be due to the limited age interval used in this study. Previous studies have found that the youngest participants usually present greater frequency of diagnosed PD.44 Likewise, the frequency of PD traits tends to decrease from adolescence to adulthood when examined longitudinally.48 The lack of agreement among studies may possible be caused by: (1) the heterogeneity of the samples and measurement instruments used, (2) the criteria used to consider PD and (3) the special characteristics of adolescence as a developmental stage, where the personality is still being formed.
The results found in this study should be interpreted in the light of the following limitations. In the first place, adolescence is a stage when the personality is still in developing, so the results should be framed within the maturation changes that occur in it. Even more, many of the traits that can be considered normal in a developmental stage, in another stage can be pathological (e.g., emotional instability). In the second place, there is a set of issues inherent to the application of any type of self-report (with the well-known overdiagnosis, possible lack of understanding the items and the limited capacity of introspection on the part of students); it would consequently have been interesting to use external informants, via outsider reports or structured interviews. Likewise, and with respect to the measurement instrument used, the PDQ-4+ has still not been scaled in adolescents and the derivation of a possible maladaptive personality pattern comes set by the cut-off points suggested by the manual for its use with adults. Consequently, the results found have to be viewed as approximate. In third place, the transversal nature of this investigation should not be forgotten; it is not possible to establish cause–effect inferences.
Future studies should use measurement instruments for maladaptive personality traits that consider the worry, conviction and stress associated with such experiences, and not only their frequency. Likewise, it would be interesting to establish specific cut-off points for this sector of the population, as well as longitudinal follow-up of the participants with high scores on this type of self-reports with a view to obtaining sensitifity and specificity values.
Ethical disclosuresProtection of human and animal subjectsThe authors state that no experiments were carried out on human being or animals for this research.
Confidentiality of dataThe authors state that no patient data appears in this article.
Right to privacy and informed consentThe authors state that no patient data appears in this article.
FundingThis research was funded by the Spanish Ministry of Science and Innovation (MICINN) and by the Instituto Carlos III, Biomedical Research Centre in the Mental Health Network (CIBERSAM). Project reference numbers: PSI 2011-28638, PSI2011-23818, PSI 2008-06220 and PSI 2008-03934.
Conflict of interestsThe authors have no conflicts of interests to declare.
Please cite this article as: Fonseca-Pedrero E, et al. Patrones desadaptativos de la personalidad del cluster B en adolescentes españoles. Rev Psiquiatr Salud Ment (Barc.). 2013;6:129–38.