




The influence of age and gender in the electrical charge delivered in a given population was analysed using an electroconvulsive therapy (ECT) clinical database.
Material and methodAn observational, prospective, longitudinal study with descriptive analysis was performed using data from a database that included total bilateral frontotemporal ECT carried out with a Mecta spECTrum 5000Q® in our hospital over 6 years. From 2006 to 2012, a total of 4337 ECT were performed on 187 patients. Linear regression using mixed effects analysis was weighted by the inverse of the number of ECT performed on each patient per year of treatment.
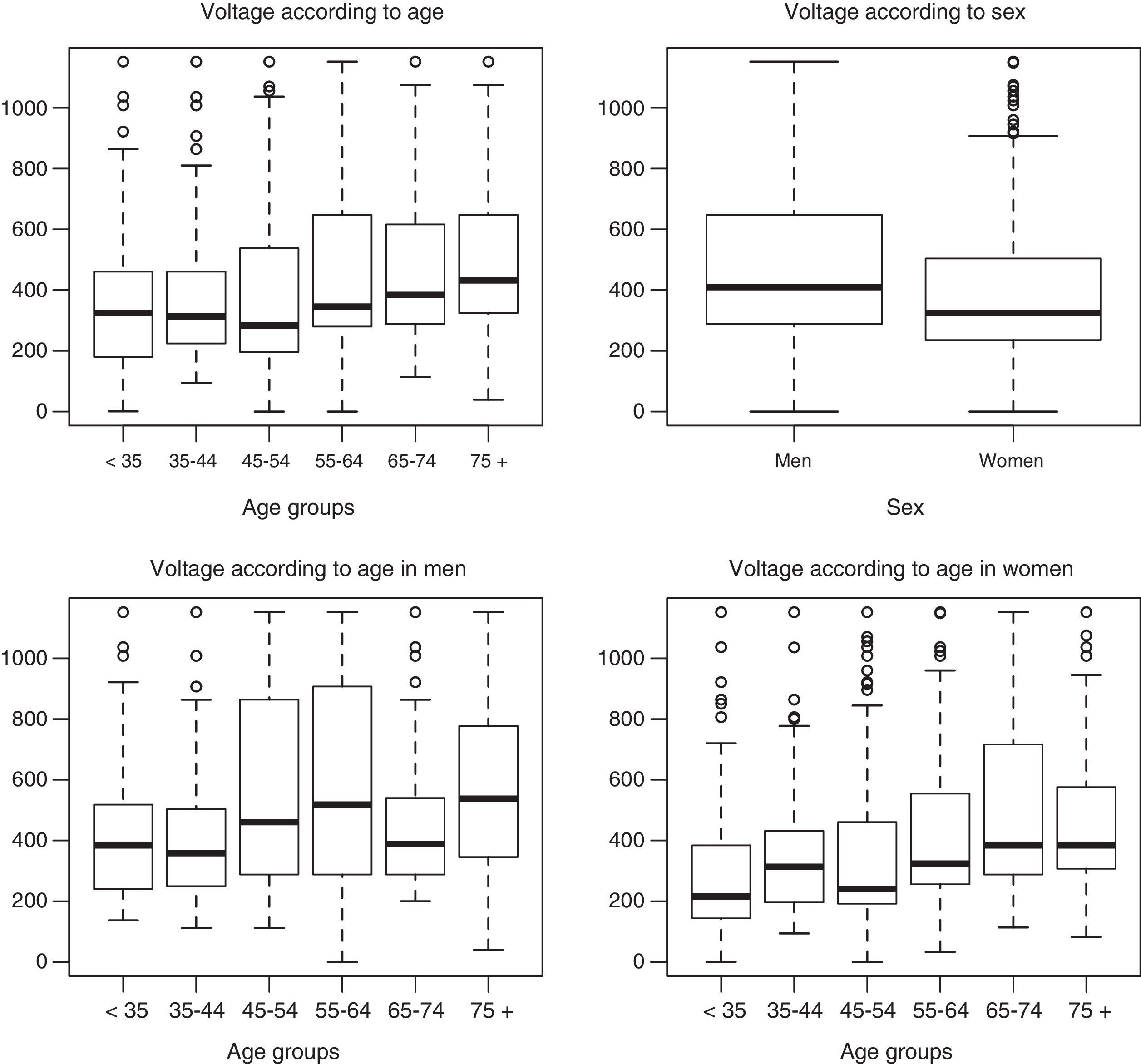
ResultsThe results indicate that age is related with changes in the required charge (P=.031), as such that the older the age a higher charge is needed. Gender is also associated with changes in charge (P=.014), with women requiring less charge than men, a mean of 87.3mC less. When the effects of age and gender are included in the same model, both are significant (P=.0080 and P=.0041). Thus, for the same age, women require 99.0mC less charge than men, and in both genders the charge increases by 2.3mC per year.
ConclusionsFrom our study, it is concluded that the effect of age on the dosage of the electrical charge is even more significant when related to gender. It would be of interest to promote the systematic collection of data for a better understanding and application of the technique.
A partir de una base de datos clínica de terapia electroconvulsiva (TEC) se pretende corroborar la influencia de la edad y el género en la carga eléctrica administrada en una población determinada.
Material y métodoEstudio observacional, prospectivo y longitudinal, con análisis descriptivo, de una base de datos que incluye el total de sesiones de TEC bilaterales frontotemporales realizadas con la Mecta spECTrum 5000Q® entre 2006 y 2012. Es una muestra de 4.337 sesiones de TEC realizadas a 187 pacientes. Mediante regresión lineal de efectos mixtos se realiza un análisis ponderado por el inverso del número de sesiones de TEC realizadas por cada paciente y por año de tratamiento.
ResultadosLos resultados indican que la edad está relacionada con cambios en la carga requerida (p=0,031): a mayor edad, mayor aumento de carga. El género también se relaciona con cambios en la carga (p=0,014): las mujeres requerirían 87,3mC menos de media que los hombres. Incluyendo los efectos de edad y género en el mismo modelo, ambos resultan significativos (p=0,0080 y p=0,0041), de modo que a igualdad de edad, las mujeres requieren 99,0mC menos de carga que los hombres, y en ambos géneros aumenta la carga 2,3mC por año de edad.
ConclusionesDel análisis se obtiene que el efecto de la edad en la dosificación de la carga eléctrica es todavía más significativo cuando se tiene en cuenta el género. Es de interés promover la recogida sistemática de datos para un mejor conocimiento y aplicación de la técnica.
There is little in the literature about electroconvulsive therapy (ECT) data base analysis, although the majority of studies published underline the advantages of such an analysis.1 It has been said that having clinical ECT databases available would make it possible to gain more knowledge about clinical practice and implement programs to improve the quality of the technique.1
The majority of the factors that may alter the initial convulsive threshold in ECT were described in a meta-analysis.2 Considering only prospective studies as the inclusion criteria, the levels of convulsive threshold are significantly associated with the following factors: sex,3,4 age,4,5 accumulated treatments,4,6 electrode location,5,7 dynamic impedance,8,9 electrical stimulation parameters10–13 and sleep deprivation.14
Of these factors, male sex4,15,16 and bilateral placement of the electrodes7 were the factors associated the most closely with a higher initial convulsive threshold.2 Other factors that influence this include the anaesthetic drugs used, oxygenation or concomitant medication. Some drugs such as benzodiazepines and anticonvulsants raise the convulsive threshold17,18; and others such as antipsychotics lower it.
This study will quantify the influence of age and sex on the electrical current required for an adequate convulsion, analysing a 6-year clinical ECT database.
Material and methodThis study is observational, prospective and longitudinal, with descriptive analysis. Its sample is the total number of ECT sessions in a Psychiatric Department from April 2006 to January 2012.
The sample includes patients treated using ECT while admitted to hospital as well as for maintenance therapy, with different psychiatric diagnoses. Propofol was used as the anaesthetic and the myorelaxant was succinylcholine. Psychoactive drugs were used in practically all of the cases, together with other medication when necessary. Re-stimulation was used once when it was needed, and some patients had received ECT beforehand.
The spECTrum 5000Q® Mecta apparatus was used, with bilateral frontotemporal electrodes. The study variables were recorded during each ECT session in a computerised database.
The current (mC) was recorded, defined as the amount of current in a single pulse multiplied by the number of pulses produced in the series.19 Static energy (joules) was also recorded, this being the estimated energy prior to applying the stimulus. This is calculated at an average estimated impedance of 220Ω.20 Dynamic energy (joules) is included too, which is considered to be the dynamic impedance, a parameter that is unknown until the stimulus is applied. Due to this the current is the one indicated to express the total stimulus dose.19
Statistical analysisRegression analysis with mixed effects was applied with a random effect (the patient) and a fixed effect (initial age, sex and treatment time), based on the average electric current required (weighted according to the inverse of the number of ECT sessions per individual, so that each patient had the same weighting in the analysis). The comparison according to sex or age group (defined based on the mean) was performed using non-parametric statistics (Mann–Whitney's U test).
The analysis used is the correct way of analysing data of this type, where the variability of ECT parameters in a single patient is less than the variability between patients. This analysis makes it possible to admit accept that one characteristic of the data (the patient himself) explains some of the observed variability.
In the model the patient amounts to a random effect, given that there is no interest in comparing the participating patients to each other, but rather in adjusting the model to extract the variability that is explained by the patient from the residual variability, as is described in the bibliography.21
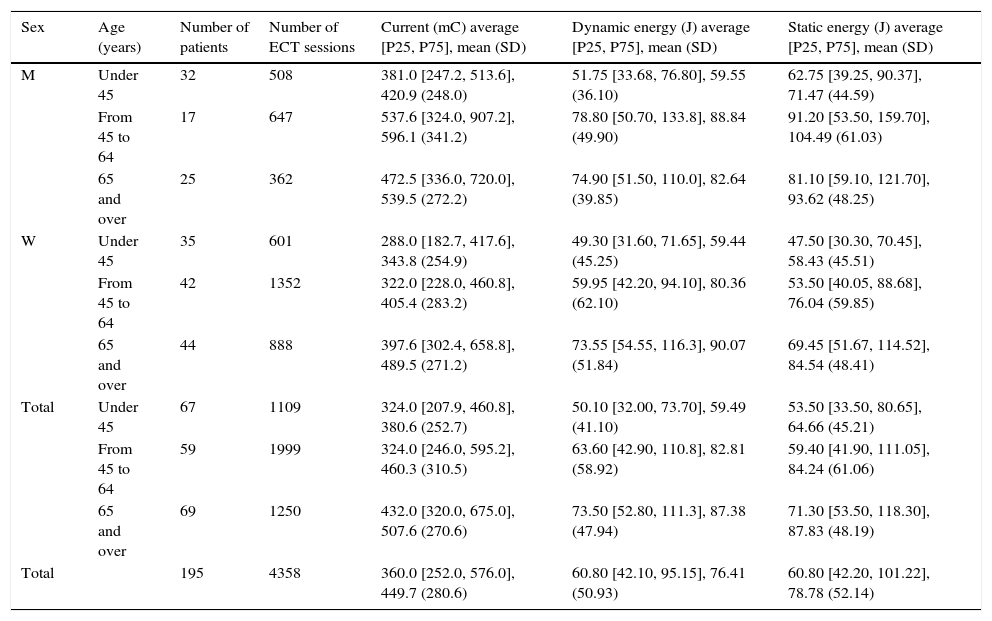
ResultsDescription of the sampleThe database contains 4337 ECT sessions and includes 187 patients (116 women and 71 men). The average follow-up time was 28 days (16 days for the first quartile and 343 days for the third quartile). The participants were aged from 17 to 88 years old, with an average age of 54.63 years old and a standard deviation of 18.37. The average current received in the total sample had a mean of 360.0mC (with 25 and 75 percentiles of 252.0 and 576.0, respectively) (Table 1).
Description of current, static energy and dynamic energy values according to sex and 3 simplified age groups.
| Sex | Age (years) | Number of patients | Number of ECT sessions | Current (mC) average [P25, P75], mean (SD) | Dynamic energy (J) average [P25, P75], mean (SD) | Static energy (J) average [P25, P75], mean (SD) |
|---|---|---|---|---|---|---|
| M | Under 45 | 32 | 508 | 381.0 [247.2, 513.6], 420.9 (248.0) | 51.75 [33.68, 76.80], 59.55 (36.10) | 62.75 [39.25, 90.37], 71.47 (44.59) |
| From 45 to 64 | 17 | 647 | 537.6 [324.0, 907.2], 596.1 (341.2) | 78.80 [50.70, 133.8], 88.84 (49.90) | 91.20 [53.50, 159.70], 104.49 (61.03) | |
| 65 and over | 25 | 362 | 472.5 [336.0, 720.0], 539.5 (272.2) | 74.90 [51.50, 110.0], 82.64 (39.85) | 81.10 [59.10, 121.70], 93.62 (48.25) | |
| W | Under 45 | 35 | 601 | 288.0 [182.7, 417.6], 343.8 (254.9) | 49.30 [31.60, 71.65], 59.44 (45.25) | 47.50 [30.30, 70.45], 58.43 (45.51) |
| From 45 to 64 | 42 | 1352 | 322.0 [228.0, 460.8], 405.4 (283.2) | 59.95 [42.20, 94.10], 80.36 (62.10) | 53.50 [40.05, 88.68], 76.04 (59.85) | |
| 65 and over | 44 | 888 | 397.6 [302.4, 658.8], 489.5 (271.2) | 73.55 [54.55, 116.3], 90.07 (51.84) | 69.45 [51.67, 114.52], 84.54 (48.41) | |
| Total | Under 45 | 67 | 1109 | 324.0 [207.9, 460.8], 380.6 (252.7) | 50.10 [32.00, 73.70], 59.49 (41.10) | 53.50 [33.50, 80.65], 64.66 (45.21) |
| From 45 to 64 | 59 | 1999 | 324.0 [246.0, 595.2], 460.3 (310.5) | 63.60 [42.90, 110.8], 82.81 (58.92) | 59.40 [41.90, 111.05], 84.24 (61.06) | |
| 65 and over | 69 | 1250 | 432.0 [320.0, 675.0], 507.6 (270.6) | 73.50 [52.80, 111.3], 87.38 (47.94) | 71.30 [53.50, 118.30], 87.83 (48.19) | |
| Total | 195 | 4358 | 360.0 [252.0, 576.0], 449.7 (280.6) | 60.80 [42.10, 95.15], 76.41 (50.93) | 60.80 [42.20, 101.22], 78.78 (52.14) |
SD: standard deviation; M: men; W: women; P25: 25 percentile; P75: 75 percentile; ECT: electroconvulsive therapy.
As the random effect, the patient explains 66% of current variability, given that there is a relationship between the measurements corresponding to a single individual and greater differences between individuals.
 according to sex and 6 age groups throughout follow-up (average).")
Sex would explain changes in the average current (P=.014); women would require an average of 87.3mC less than men. The average current for the latter is 71.2% higher than it is for the women of the same age.
Age would explain changes in the average current (P=.031 for years of age), so that the current needed would increase with age (this increase not being lineally proportional).
When the effects of age and sex are examined in the same model, both are significant (P=.0041 for sex and P=.0080 for years of age), so that at the same age, women need 99.0mC less current than men; and in both sexes the current increases with age (2.3mC per year of age), although the model fits better when the interaction between sex and age group is taken into account.
DiscussionThe analysis of ECT databases makes it possible to discover the degree to which age and sex influence the electrical current used. Nevertheless, this is a heterogeneous sample with confusion factors that may restrict the interpretation of the results.
The current required to obtain an effective convulsion increases with age, and this is explained by the fact that the convulsive threshold rises with physiological age.2 Sex may also explain changes in the average current, given that men have a higher convulsive threshold than women of the same age.2
When the effects of age and sex are included in the same model both of them are significant; thus at the same age women require a lower current than men; and in both sexes the current increases with age. It can therefore be said that sex modifies the effect of age on the current.
The literature mainly contains studies that centre on the convulsive threshold, with fewer on the average current used, as is the case for us.22 One meta-analysis2 describes how sex is the factor that most influences variations in the initial convulsive threshold (70% higher for men than it is for women).2,4 This datum agrees with our study, where the average current used for men was 71.2% higher than it was for women of the same age. On the other hand, age had a more moderate effect on changes to the convulsive threshold.2,4
Although the convulsive threshold varies substantially from one individual to another, the said meta-analysis2 describes a narrow range of distribution of the average convulsive threshold. In the majority of patients the convulsive threshold would stand at from a 50 to 200mC dose of current.2 Theoretically, adjusting this range of current for 2 or 3 patient characteristics (age, sex, concomitant treatment, the position of the electrodes, etc.) could make it possible to precisely determine dose above the threshold for each person. In our sample the current dose is above the values described in this meta-analysis; we consider that several confusion factors have increased the convulsive threshold.
The sample size would stand out as the strong point of the study (n=4337). This is an ecological study, and studies of this type are useful for evaluating interventions in populations such as health promotion strategies, given their simplicity, efficiency and swift data acquisition.
Respecting the weak points of the study, the sample includes patients with a range of diseases and their psychiatric and medical treatments. The different diagnoses and treatments may modify the convulsive threshold.2,23 Although the anaesthesia was homogeneous, the dose varied depending on the patient, and this may modify the convulsive threshold. Likewise, patients were included who received ECT while admitted as well as others who received maintenance ECT: this is a limitation.
To conclude, analysing the ECT database shows that the effect of age on the current dose is even more significant when patient sex is taken into account. Sex is therefore decisive in explaining the current dose that is necessary to produce an optimum convulsion, and it should be considered to be one of the main variables that influence the convulsive threshold.5
ECT is an effective treatment; however, little attention has been paid to it in clinical or more technical research.24 Information on ECT administration should be analysed to evaluate practical clinical questions. Better understanding of ECT mechanisms could lead to more rationally designed dosing strategies that could potentially be more effective, reducing side effects and the variability of clinical results between individuals.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed are in accordance with the ethical norms of the committee for responsible human experimentation and the World Medical Association and the Helsinki Declaration.
Confidentiality of dataThe authors declare that they followed the protocols of their centre of work on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this paper.
FinancingThis study was undertaken thanks to several contributions: JSS received a post-internship grant from IRB Lleida. MMA is the chief researcher in a grant from the Carlos III Healthcare Institute (PI11/01956). MJPM has received financing from the Spanish Government Ministry of Science and Innovation and the Carlos III Healthcare Institute through a Miguel Servet research contract (CP10-00393), the National Research Plan (State R+D+I Plan 2013–2016), co-financed by the European Regional Development Fund (FEDER).
Conflict of interestsEVP has received research grants and has worked as a consultant, advisor or representative for the following companies: Almirall, AstraZeneca, Bristol-Myers Squibb, Elan, Eli Lilly, el Instituto de Investigaciones Forestales, Gedeon Richter, GlaxoSmithKline, Janssen-Cilag, Jazz, Lundbeck, Merck, Novartis, Organon, Otsuka, Pfizer, Roche, Sanofi-Aventis, Servier, Solvay, Schering-Plough, Shire, Sunovion, Takeda, United BioSource Corporation and Wyeth. He has also received financing for research from the Spanish Government Ministry of Science and Innovation, the Stanley Medical Research Institute and the Seventh European Union Framework Program. The other authors have no conflict of interests to declare.
We would like to thank the Psychiatric and Anaesthesia Departments of Santa Maria Hospital, Lleida, and in particular the Psychiatry interns trained in this hospital; and we would also like to thank the patients who kindly took part in this study.
Please cite this article as: Salvador Sánchez J, David MD, Torrent Setó A, Martínez Alonso M, Portella Moll MJ, Pifarré Paredero J, et al. Base de datos clínica de terapia electroconvulsiva: influencia de edad y género en la carga eléctrica. Rev Psiquiatr Salud Ment (Barc). 2017;10:143–148.