




Healthy lifestyles are relevant to several diseases and to maintain individuals’ mental health. Exposure to epidemics and confinement have been consistently associated with psychological consequences, but changes on lifestyle behaviours remain under-researched.
Materials and MethodsAn online survey was conducted among the general population living in Spain during the COVID-19 home-isolation. In addition to demographic and clinical data, participants self-reported changes in seven lifestyle domains. The Short Multidimensional Inventory Lifestyle Evaluation was developed specifically to evaluate changes during the confinement (SMILE-C).
ResultsA total of 1254 individuals completed the survey over the first week of data collection. The internal consistency of the SMILE-C to assess lifestyles during confinement was shown (Cronbach's Alpha=0.747). Most participants reported substantial changes on outdoor time (93.6%) and physical activity (70.2%). Moreover, about one third of subjects reported significant changes on stress management, social support, and restorative sleep. Several demographic and clinical factors were associated to lifestyle scores. In the multivariate model, those independently associated with a healthier lifestyle included substantial changes on stress management (p<0.001), social support (p=0.001) and outdoor time (p<0.001), amongst others. In contrast, being an essential worker (p=0.001), worse self-rated health (p<0.001), a positive screening for depression/anxiety (p<0.001), and substantial changes on diet/nutrition (p<0.001) and sleep (p<0.001) were all associated with poorer lifestyles.
ConclusionsIn this study, sizable proportions of participants reported meaningful changes in lifestyle behaviours during the COVID-19 pandemic in Spain. Moreover, the SMILE-C was sensitive to detect these changes and presented good initial psychometric properties. Further follow-up studies should collect relevant data to promote healthy lifestyles in pandemic times.
Los estilos de vida saludables son relevantes para diversas enfermedades, así como para mantener la salud mental de los individuos. La exposición a epidemias y confinamientos se ha asociado de manera consistente a consecuencias psicológicas, pero los cambios en los comportamientos del estilo de vida siguen sin investigarse.
Materiales y métodosSe realizó una encuesta online entre la población general residente en España durante el confinamiento domiciliario debido a COVID-19. Además de los datos demográficos y clínicos, los participantes auto-reportaron los cambios producidos en siete dominios del estilo de vida. Se desarrolló específicamente Short Multidimensional Inventory Lifestyle Evaluation (SMILE-C) para evaluar los cambios durante el confinamiento.
ResultadosUn total de 1.254 individuos completaron la encuesta durante la primera semana de recabado de los datos. Se reflejó la consistencia interna de SMILE-C para evaluar los estilos de vida durante el confinamiento (alfa de Cronbach=0,747). La mayoría de los participantes reportó cambios sustanciales en cuanto al tiempo al aire libre (93,6%) y a la actividad física (70,2%). Además, alrededor de un tercio de los sujetos reportó cambios significativos en cuanto a gestión del estrés, respaldo social y sueño reparador. Algunos factores demográficos y clínicos se asociaron a las puntuaciones del estilo de vida. En el modelo multivariante, aquellos factores asociados de manera independiente a un estilo de vida más saludable incluyeron cambios sustanciales en cuanto a gestión del estrés (p<0,001), respaldo social (p=0,001) y tiempo al aire libre (p<0,001), entre otros. Por contra, los factores relacionados con ser un trabajador esencial (p=0,001), peor salud auto-calificada (p<0,001), cribado positivo de depresión/ansiedad (p<0,001) y cambios sustanciales en la dieta/nutrición (p<0,001) y sueño (p<0,001) estuvieron asociados a peores estilos de vida.
ConclusionesEn este estudio, proporciones considerables de participantes reportaron cambios significativos en los comportamientos del estilo de vida durante la pandemia por COVID-19 en España. Además, la escala SMILE-C fue sensible a la hora de detectar dichos cambios, y presentó buenas propiedades psicométricas iniciales. Los estudios de seguimiento futuros deberán recopilar datos relevantes para promover estilos de vida saludables en tiempos de pandemia.
Nutrition, physical activity, and restorative sleep are regarded as fundamental aspects of human health, as well as the three traditional pillars of lifestyle.1 Currently, lifestyle is seen as a multidimensional construct encompassing a wider range of behaviours, such as smoking, alcohol/substance misuse, stress management, social support, and screen time and digital technology usage.2,3 The key role of healthy lifestyles (HLs) to reduce all-cause mortality and to maintain individuals’ health and wellbeing has been consistently demonstrated.4 HLs are relevant for several non-communicable diseases (NCDs), such as cardiovascular diseases, type 2 diabetes, metabolic syndrome, and depression.5,6 Recent evidence supports that a lower degree of adherence to many HLs is associated with worse outcomes in several psychiatric disorders other than depression.7 Accordingly, promoting adherence to HLs and lifestyle-based interventions has been advocated for individuals with NCDs and psychiatric disorders, as well as the general population.8,9
In COVID-19 times, examining whether lifestyle behaviours significantly change under home isolation is clearly a relevant research question.10 Exposure to recent emergent infectious disease (EID) outbreaks (e.g. SARS, MERS, Ebola Virus Disease or EVD) has been associated with remarkable changes in daily life and health outcomes, which are thought to result mostly from physical-distancing policies, such as home isolation and quarantine.11 The bulk of the research on the effect that epidemics and confinement have on health focused on psychological issues, such as stress-related symptoms and disorders, and to a lesser degree social support and stress management. Exposure to epidemics and confinement have been consistently associated with substantial psychological consequences, especially among patients infected with EID and healthcare workers.12–14 In contrast, lifestyle issues during EID-related confinement, including dietary changes, restricted physical activity, as well the effect of increased indoor and screen time, remain under-researched.15
A handful of observational studies have examined lifestyles at the population level during either the COVID-19 pandemic or recent epidemics.16–20 However, these surveys assessed specific lifestyle behaviours and did not undertake a comprehensive approach.
In order to bridge this research gap, we set forth to develop a multidimensional assessment of lifestyle behaviours at the population level. The aims of the present study are threefold: (1) to describe self-reported changes in lifestyle behaviours during the COVID-19 pandemic at the population level in Spain, (2) to evaluate the psychometric properties of the Short Multidimensional Inventory Lifestyle Evaluation (SMILE) during the COVID-19 pandemic, and (3) to evaluate factors associated to lifestyle scores during the COVID-19 self-isolation period.
Materials and methodsStudy designCross-sectional study through an online survey (websurvey) conducted between April 15, 2020 and May 15, 2020. Considering the estimated sample size, the present analysis included data from the first week of data collection. The online questionnaire was programmed in SurveyGizmo® (http://www.surveygizmo.com.br/) and included questions about lifestyle behaviours demographics, COVID-19 experience, self-rated health and previous diagnosed conditions.
Study populationThe study population included individuals from all over Spain, adults from both sexes who have access to the Internet and who agree to participate in the study after reading the informed consent form. To avoid duplicated responses, individuals who report having already previously completed the online questionnaire were excluded.
Sample size and recruitmentConsecutive, convenience sample including individual reached through Facebook,21 WhatsApp and Twitter. As there were no previous data to estimate the sample size, we defined for the present analysis that the sample should be large enough to detect an absolute difference of 5 points in the mean Short Multidimensional Inventory Lifestyle Evaluation – Confinement (SMILE-C; see below) score between individuals reporting to be self-isolated or not. Considering the total SMILE-C score (108), we estimated an equal standard deviation of 10 in the groups. With a 5% alfa and 95% beta, the sample size should be 126 (i.e., 63 participants in each group). As some previous websurveys22,23 reported an attrition rate of 30%, we multiplied the original estimate by 1.3 and our final sample size should be comprised by be at least 164 individuals presenting complete questionnaires.
OutcomeThe main outcome was the score of the SMILE-C scale. This scale was developed specifically to allow a multidimensional measure of lifestyle during the COVID-19 pandemic.
The original SMILE is a 43-item self-rated questionnaire comprised by 7-domains (Diet and Nutrition, Substance abuse, Physical activity, Stress management, Restorative sleep, Social support and Environmental exposures), as may be seen in Supplementary Material 1. It was developed to allow a multidimensional and comprehensive assessment of (healthy) lifestyle during the previous 30 days. An initial draft was created including 48 items divided into six lifestyle domains (Diet, Physical activity, Sleep, Interpersonal relationships, Work performance, Safety and access to health care). This draft was circulated to the research team to refine the instrument by means of amendments and suggestions. The domains “Work performance” and “Safety and access to health care” were excluded while others such as Substance abuse, Stress management and Environmental exposures (indoor/outdoor time) were included, based on other existing lifestyle questionnaires. The second draft consisted of 94 items with seven lifestyle related domains. It was circulated again between researchers and the best items to discriminate heathy and unhealthy patterns were defined reaching a version with 69 items. After careful revision, the research group removed 12 items and maintained the seven lifestyle domains. Then, two external experts on lifestyle provided feedback on the comprehensiveness, relevance and readability of the items. Reviewers suggested summarizing some domains, a 43-item version was generated and agreed upon by the research group. Response options are measured through a 4-point Likert scale and the final score is obtained by the sum of all questions (noting that some questions present reverse scores). The higher the score, the better (healthier) the lifestyle.
The original SMILE was used to collect data and refined to be appropriate during the pandemic self-isolation/confinement. Initially, questions presenting more than 2% frequency of ‘I prefer not to answer‘were removed because most of these questions were not appropriate during a social distance and home lockdown situations (for example, item 22: ‘Are you satisfied with the time it takes you to commute to work?’). Questions presenting less than 2% frequency of ‘I prefer not to answer’, were imputed as zero. Afterwards, principal component analysis and factorial analysis were performed to reach a 27-item version (Supplementary Material 2) presenting an overall Cronbach-a=0.75 and Kaiser–Meyer–Olkin Measure=0.77. Main results from principal component analysis and factorial analysis are available in Supplementary Material 3. At the time of writing, the SMILE questionnaire is available in three languages: English, Spanish and Portuguese.
Variables and measurementsDemographic information included sex, age, educational level, working status (if healthcare/essential service worker or working on the front line) and region of residence (dichotomized into Valencian Community and others). Social distancing/self-isolation was considered as dichotomous variable (yes/no).
The COVID-19 questions were related to diagnosis (yes/no) and lost of significant ones (yes/no).
Change in lifestyle behaviours during the COVID-19 pandemic as compared to habitual, previous ones was self-reported after each domain of the original SMILE using questions that read as ‘Did you change your (nutritional habits and diet) during the COVID-19 pandemic?’. Response options were measured using a 4-point Likert scale (Totally, Moderately, Mildly, Not at all) and aggregated into Totally/Moderately and Mildly/Not at all.
Self-rated health (SRH) was measured using the question ‘How would you rate your health in general?’, with possible answer choices of ‘Very bad’, ‘Bad,’ ‘Neither good nor bad’, ‘Good’ and ‘Very good’.24–26 Response options were aggregated into Very good/Good and Neither good nor bad/Bad/Very bad.
Previously diagnosed conditions were self-reported using the question ‘In the last 12 months, have you been diagnosed by a medical doctor or health professional, or received treatment for any of the following conditions?’. Possible health problems investigated include diabetes, heart disease, hypertension, stroke, anaemia, asthma, depression, anxiety, bipolar disorder, schizophrenia, anorexia/bulimia, HIV/AIDS, cancer, tuberculosis, cirrhosis, renal disease, and others (Bastos et al., 2017; IBGE, 2013).
Current depression was screened using Patient Health Questionnaire-2 (PHQ-2)27 using a cut-off =3, and current anxiety was screened using the Generalized Anxiety Disorder 7-item (GAD-7)28 using a cut-off =10. Two dichotomous variables were created ‘Positive Depression‘and ‘Positive Anxiety’. Then, a composite variable was created using the aforementioned variables with the following categories: No positive screening, Positive screening for Depression only, Positive screening for Anxiety only, and Positive screening for both. Screening for alcohol abuse was performed using the AUDIT-C29 and cut-off was =3.
Statistical analysisMean and standard deviation of the SMILE-C scores were calculated for all variables, and statistically significant differences between categories were evaluated using the Student t test (for dichotomous variables) or ANOVA (for variables presenting more than two response categories). Bivariate associations between age and the number of people living in the household with the SMILE-C score were evaluated using the Pearson and Spearman correlation tests, respectively.
Multivariate linear regression models were performed to evaluate the effect of independent factors on the SMILE-C score. The initial model included variables associated with SMILE-C at p<0.20 in the bivariate analysis. Sex, age, working status and self-isolation were defined to be included a priori and kept in the model due to their importance in the literature and in the pandemic. A final model was reached using a manual stepwise removal of each non-statistically significant variable and evaluating changes in the remaining B (except those included a priori).
Ethical aspectsThe study was approved by the Ethics Committee at the Hospital Universitari i Politècnic La Fe, in Valencia, Spain. The survey was anonymous (no identification -name, city or IP address was collected) and participants read the consent form and confirmed their interest on participating in the first screen of the online questionnaire. In addition, as direct benefit, after answering each domain questions, participants could read some information regarding ways to maintain a healthy lifestyle during the pandemic.
ResultsThe online survey was conducted between April 15 and April 22, 2020. Overall, 1337 questionnaires were initiated, and all those individuals provided informed consent. However, 80 were not eligible for the study (n=57 had already participated in the survey, n=16 were not living in Spain, and n=7 were younger than 18 years). Additionally, three individuals preferred not to answer if they were self-isolated or not and were excluded. Thus, our final sample included 1254 individuals.
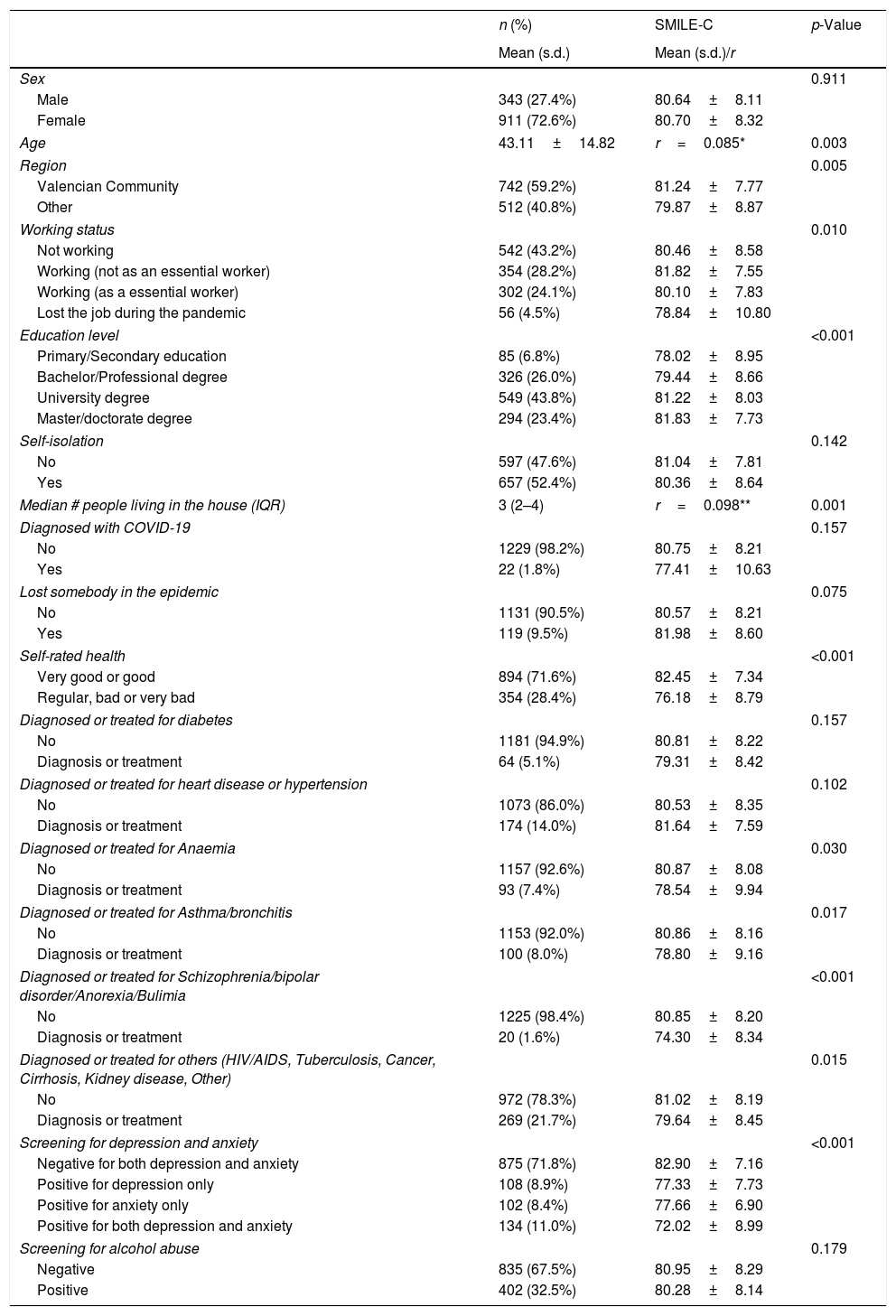
The mean and standard deviation for the SMILE-C scale was 80.68±8.26 considering the total sample. Table 1 describes the sociodemographic and clinical characteristics of the sample, the respective SMILE-C means and their bivariate association. We found that lower SMILE-C scores (unhealthier lifestyles) were associated with: younger age (p=0.003), not living in Valencia (p=0.005), working status (p=0.010), lower educational level (p<0.001), lower number of people living in the house (p=0.001), regular, bad or very bad Self-Rated Health (p<0.001), having a positive screening for depression/anxiety (p<0.001), and being diagnosed or treated for several conditions, including anaemia (p=0.030), asthma/bronchitis (p=0.017), psychiatric disorders (schizophrenia/bipolar disorder/anorexia/bulimia) (p=0.001), and others (HIV/AIDS, tuberculosis, cancer, cirrhosis, kidney disease, other) (p=0.015) (see Table 1).
Sociodemographic, clinical characteristics and the mean SMILE-C score among 1254 participants. Spain, April-15–22, 2020.
| n (%) | SMILE-C | p-Value | |
|---|---|---|---|
| Mean (s.d.) | Mean (s.d.)/r | ||
| Sex | 0.911 | ||
| Male | 343 (27.4%) | 80.64±8.11 | |
| Female | 911 (72.6%) | 80.70±8.32 | |
| Age | 43.11±14.82 | r=0.085* | 0.003 |
| Region | 0.005 | ||
| Valencian Community | 742 (59.2%) | 81.24±7.77 | |
| Other | 512 (40.8%) | 79.87±8.87 | |
| Working status | 0.010 | ||
| Not working | 542 (43.2%) | 80.46±8.58 | |
| Working (not as an essential worker) | 354 (28.2%) | 81.82±7.55 | |
| Working (as a essential worker) | 302 (24.1%) | 80.10±7.83 | |
| Lost the job during the pandemic | 56 (4.5%) | 78.84±10.80 | |
| Education level | <0.001 | ||
| Primary/Secondary education | 85 (6.8%) | 78.02±8.95 | |
| Bachelor/Professional degree | 326 (26.0%) | 79.44±8.66 | |
| University degree | 549 (43.8%) | 81.22±8.03 | |
| Master/doctorate degree | 294 (23.4%) | 81.83±7.73 | |
| Self-isolation | 0.142 | ||
| No | 597 (47.6%) | 81.04±7.81 | |
| Yes | 657 (52.4%) | 80.36±8.64 | |
| Median # people living in the house (IQR) | 3 (2–4) | r=0.098** | 0.001 |
| Diagnosed with COVID-19 | 0.157 | ||
| No | 1229 (98.2%) | 80.75±8.21 | |
| Yes | 22 (1.8%) | 77.41±10.63 | |
| Lost somebody in the epidemic | 0.075 | ||
| No | 1131 (90.5%) | 80.57±8.21 | |
| Yes | 119 (9.5%) | 81.98±8.60 | |
| Self-rated health | <0.001 | ||
| Very good or good | 894 (71.6%) | 82.45±7.34 | |
| Regular, bad or very bad | 354 (28.4%) | 76.18±8.79 | |
| Diagnosed or treated for diabetes | 0.157 | ||
| No | 1181 (94.9%) | 80.81±8.22 | |
| Diagnosis or treatment | 64 (5.1%) | 79.31±8.42 | |
| Diagnosed or treated for heart disease or hypertension | 0.102 | ||
| No | 1073 (86.0%) | 80.53±8.35 | |
| Diagnosis or treatment | 174 (14.0%) | 81.64±7.59 | |
| Diagnosed or treated for Anaemia | 0.030 | ||
| No | 1157 (92.6%) | 80.87±8.08 | |
| Diagnosis or treatment | 93 (7.4%) | 78.54±9.94 | |
| Diagnosed or treated for Asthma/bronchitis | 0.017 | ||
| No | 1153 (92.0%) | 80.86±8.16 | |
| Diagnosis or treatment | 100 (8.0%) | 78.80±9.16 | |
| Diagnosed or treated for Schizophrenia/bipolar disorder/Anorexia/Bulimia | <0.001 | ||
| No | 1225 (98.4%) | 80.85±8.20 | |
| Diagnosis or treatment | 20 (1.6%) | 74.30±8.34 | |
| Diagnosed or treated for others (HIV/AIDS, Tuberculosis, Cancer, Cirrhosis, Kidney disease, Other) | 0.015 | ||
| No | 972 (78.3%) | 81.02±8.19 | |
| Diagnosis or treatment | 269 (21.7%) | 79.64±8.45 | |
| Screening for depression and anxiety | <0.001 | ||
| Negative for both depression and anxiety | 875 (71.8%) | 82.90±7.16 | |
| Positive for depression only | 108 (8.9%) | 77.33±7.73 | |
| Positive for anxiety only | 102 (8.4%) | 77.66±6.90 | |
| Positive for both depression and anxiety | 134 (11.0%) | 72.02±8.99 | |
| Screening for alcohol abuse | 0.179 | ||
| Negative | 835 (67.5%) | 80.95±8.29 | |
| Positive | 402 (32.5%) | 80.28±8.14 | |
SMILE-C: Short Multidimensional Inventory Lifestyle Evaluation – Confinement; s.d.: Standard Deviation; r=correlation coefficient of the *Pearson or **Spearman; IQR: Interquartile Range; HIV: Human Immunodeficiency Virus/AIDS: Acquired immunodeficiency syndrome.
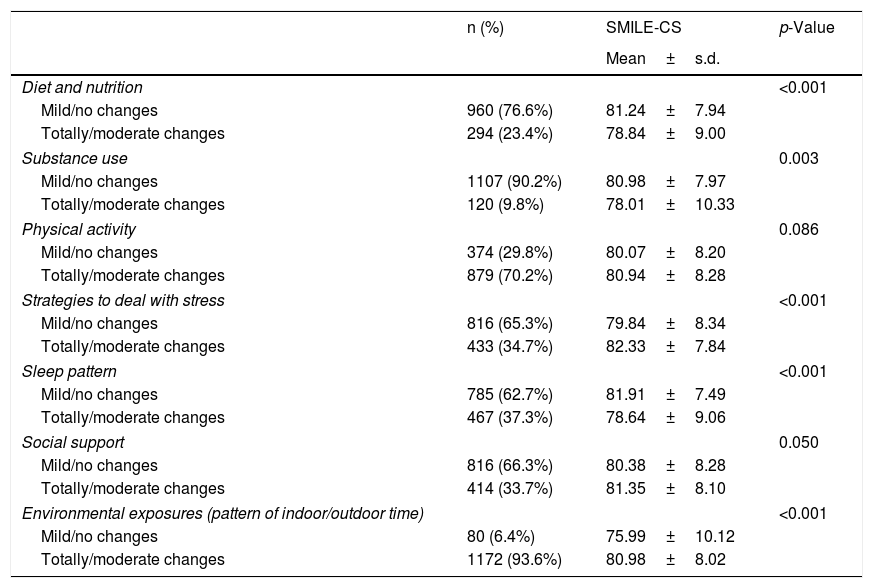
Table 2 shows the self-reported changes on lifestyle behaviours during the COVID-19 pandemic. As expected, the greatest self-reported changes were observed for the environmental exposures, where 93.6% of our sample described a substantial (total or moderate) change during the pandemic. Apart from that, 70.2% (n=879) reported totally/moderate change on physical activity, 34.7% (n=433) on stress management, 33.7% (n=414) on social support, 37.3% (n=467) on sleep pattern, 23.4% (n=294) on diet and nutrition, and 9.8% (n=120) on substance use. In addition, we found significantly lower SMILE-C scores (unhealthier lifestyles) among individuals who reported totally/moderate change on dietary and nutritional habits (p<0.001), substance use habits (p=0.003), and on sleep pattern (p<0.001) during the COVID-19 pandemic, as compared to individuals who reported mild/no changes. On the other hand, we found higher SMILE-C scores (healthier lifestyles) among individuals who reported totally/moderate changes on strategies to deal with stress (p<0.001), on social support (p = 0.050), and on the pattern of indoor/outdoor time (p<0.001) during the COVID-19 pandemic, as compared to individuals who reported mild/no changes.
Self-reported changes on lifestyle habits during the COVID-19 pandemic and the mean SMILE-C score among 1254 participants. Spain, April-15–22, 2020.
| n (%) | SMILE-CS | p-Value | |
|---|---|---|---|
| Mean±s.d. | |||
| Diet and nutrition | <0.001 | ||
| Mild/no changes | 960 (76.6%) | 81.24±7.94 | |
| Totally/moderate changes | 294 (23.4%) | 78.84±9.00 | |
| Substance use | 0.003 | ||
| Mild/no changes | 1107 (90.2%) | 80.98±7.97 | |
| Totally/moderate changes | 120 (9.8%) | 78.01±10.33 | |
| Physical activity | 0.086 | ||
| Mild/no changes | 374 (29.8%) | 80.07±8.20 | |
| Totally/moderate changes | 879 (70.2%) | 80.94±8.28 | |
| Strategies to deal with stress | <0.001 | ||
| Mild/no changes | 816 (65.3%) | 79.84±8.34 | |
| Totally/moderate changes | 433 (34.7%) | 82.33±7.84 | |
| Sleep pattern | <0.001 | ||
| Mild/no changes | 785 (62.7%) | 81.91±7.49 | |
| Totally/moderate changes | 467 (37.3%) | 78.64±9.06 | |
| Social support | 0.050 | ||
| Mild/no changes | 816 (66.3%) | 80.38±8.28 | |
| Totally/moderate changes | 414 (33.7%) | 81.35±8.10 | |
| Environmental exposures (pattern of indoor/outdoor time) | <0.001 | ||
| Mild/no changes | 80 (6.4%) | 75.99±10.12 | |
| Totally/moderate changes | 1172 (93.6%) | 80.98±8.02 | |
SMILE-C: Short Multidimensional Inventory Lifestyle Evaluation – Confinement; s.d.: Standard Deviation.
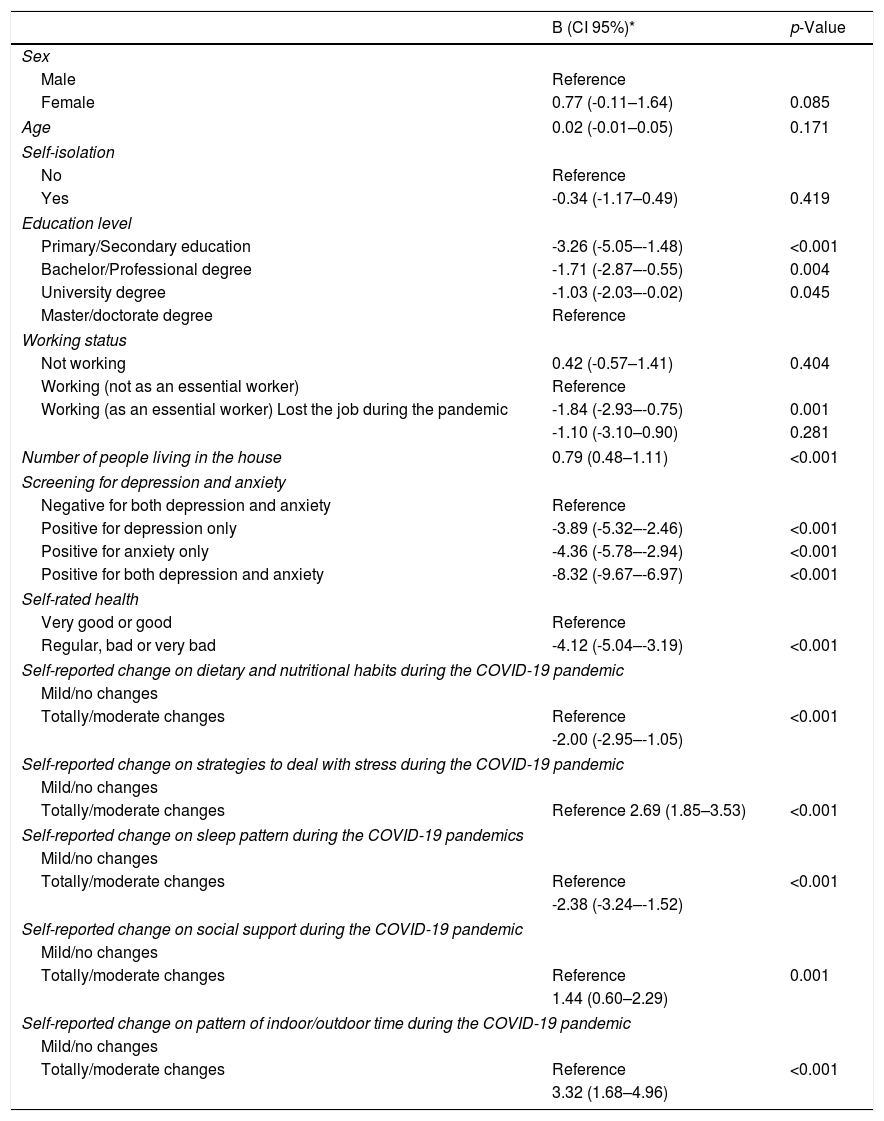
Table 3 shows the final multivariate model. The variables that remained independently associated with a healthier lifestyle (i.e., higher SMILE-C scores) were a higher number of people living in the household and totally/moderate changes on dealing with stress, to be on social support and on time spend indoors/outdoors. Lower education, being an essential worker, worse self-rated health, positive screening for depression/anxiety, and totally/moderate changes on dietary and nutritional habits and on sleep patterns were associated with unhealthier lifestyle (i.e., lower SMILE-C scores).
Factors associated with better SMILE-C scores among n=1191 participants. Spain, April-15–22, 2020.
| B (CI 95%)* | p-Value | |
|---|---|---|
| Sex | ||
| Male | Reference | |
| Female | 0.77 (-0.11–1.64) | 0.085 |
| Age | 0.02 (-0.01–0.05) | 0.171 |
| Self-isolation | ||
| No | Reference | |
| Yes | -0.34 (-1.17–0.49) | 0.419 |
| Education level | ||
| Primary/Secondary education | -3.26 (-5.05–-1.48) | <0.001 |
| Bachelor/Professional degree | -1.71 (-2.87–-0.55) | 0.004 |
| University degree | -1.03 (-2.03–-0.02) | 0.045 |
| Master/doctorate degree | Reference | |
| Working status | ||
| Not working | 0.42 (-0.57–1.41) | 0.404 |
| Working (not as an essential worker) | Reference | |
| Working (as an essential worker) Lost the job during the pandemic | -1.84 (-2.93–-0.75) | 0.001 |
| -1.10 (-3.10–0.90) | 0.281 | |
| Number of people living in the house | 0.79 (0.48–1.11) | <0.001 |
| Screening for depression and anxiety | ||
| Negative for both depression and anxiety | Reference | |
| Positive for depression only | -3.89 (-5.32–-2.46) | <0.001 |
| Positive for anxiety only | -4.36 (-5.78–-2.94) | <0.001 |
| Positive for both depression and anxiety | -8.32 (-9.67–-6.97) | <0.001 |
| Self-rated health | ||
| Very good or good | Reference | |
| Regular, bad or very bad | -4.12 (-5.04–-3.19) | <0.001 |
| Self-reported change on dietary and nutritional habits during the COVID-19 pandemic | ||
| Mild/no changes | ||
| Totally/moderate changes | Reference | <0.001 |
| -2.00 (-2.95–-1.05) | ||
| Self-reported change on strategies to deal with stress during the COVID-19 pandemic | ||
| Mild/no changes | ||
| Totally/moderate changes | Reference 2.69 (1.85–3.53) | <0.001 |
| Self-reported change on sleep pattern during the COVID-19 pandemics | ||
| Mild/no changes | ||
| Totally/moderate changes | Reference | <0.001 |
| -2.38 (-3.24–-1.52) | ||
| Self-reported change on social support during the COVID-19 pandemic | ||
| Mild/no changes | ||
| Totally/moderate changes | Reference | 0.001 |
| 1.44 (0.60–2.29) | ||
| Self-reported change on pattern of indoor/outdoor time during the COVID-19 pandemic | ||
| Mild/no changes | ||
| Totally/moderate changes | Reference | <0.001 |
| 3.32 (1.68–4.96) | ||
SMILE-C: Short Multidimensional Inventory Lifestyle Evaluation – Confinement; B: regression coefficient; *Positive B indicates a better (higher) SMILE-C score.
The present study showed the internal consistency of the SMILE-C to assess lifestyle behaviours adopted during the COVID-19 pandemic-related confinement. Similar studies had previously examined fewer aspects of lifestyle, such as social support, sleep pattern, and diet/nutrition.16–20,30 To our knowledge, the present report is the first observational survey that examined a wide range of lifestyle changes during home self-isolation. The SMILE-C aligns with contemporary, official definitions of lifestyle as a multidimensional construct.2,3 The present survey was initiated one month after lockdown was issued in Spain due to the COVID-19 pandemic. Here, results refer to the first week of data collection, including 1254 adults living in Spain who volunteered to participate. The sample was predominantly composed of middle-aged, highly educated women. Most participants were still working, and 25% worked on essential services. Less than 2% of respondents reported to be infected with COVID-19, and nearly 10% had lost a significant one during the pandemic. Moreover, almost three out of four participants considered themselves to be in very good or good health.
The first aim of this study was to describe self-reported lifestyle changes during the COVID-19 confinement. Environmental exposures (indoor versus outdoor time) and physical activity were the domains most sensitive to the effects of confinement. Indeed, the majority of survey participants reported to have experienced substantial changes in both domains during the pandemic. These results were expected and may be explained by the restrictions imposed by home isolation itself.11 As recently reported, the major consequence of mandatory self-isolation has been the reduction of outdoor activities, which in turn affects most types of physical activity.31 Moreover, about one third of the participants reported significant changes in other lifestyle behaviours, namely stress management, social support, and restorative sleep.
Previous studies have examined lifestyle changes during recent outbreaks in Asia.20,32,33 Sizable proportions of survey participants reported favourable changes on support from both relatives and friends as well as on time spent to rest, to relax and to exercise during the SARS epidemic in Hong Kong32 and the COVID-19 pandemic in a Chinese province.20 Studies conducted during or after situations of crisis, not specifically under confinement, showed increased frequencies of sleeping problems, smoking and drinking.33–35 At the ending phase of the SARS epidemic in Hong Kong, about 37% of the sample perceived that their levels of stress related with work and family settings had increased, whereas about 20% reported sleep problems during the epidemic.33 Increased substance use has been described following disasters other than EID outbreaks, such as the September 11, 2001, terrorist attacks in the United States.34,35 For instance, 28.8% of the sample reported an increase in use of any of three substances (alcohol, tobacco and marijuana) 5–8 weeks after the September 11 attacks.34 Taken together, the present results converge with those of previous observational studies consistently showing that confinement is associated with disruptions in patterns of usual behaviours.20
After adjusting for confounders, substantial changes in behaviours during confinement were associated with global lifestyle scores. Participants who reported significant variations in their dietary/nutritional and sleep showed significantly poorer lifestyles than those with mild or no changes. Of note, these are two classic pillars of lifestyle with a more biological or medical tradition. Due to uncertainty about food supply during the first weeks of lockdown, community members tend to purchase ultra-processed, unhealthy food instead of fresh food.31 In addition, comfort food may be used as self-medication to alleviate confinement-related stress.36 In the present study, we showed substantial changes in sleep patterns during the pandemic, which is consistent with findings from Italian and Chinese studies.18,19 These may be also explained by restrictions imposed by home isolation as recently suggested.31 Interestingly, self-reported changes in substance use pattern were not associated with lifestyle in our study. These findings suggest that variations in diet and sleep might negatively impact on overall lifestyle, but prospective studies are necessary to further examine this hypothesis.
Of note, additional factors associated with lower SMILE-C scores were to be an essential worker and to have positive screenings for depression and anxiety. Essential workers are likely to be submitted to increased work demands and face more directly the risk of infecting their significant ones and face infection themselves. Health workers are particularly exposed to extended working hours and the inherent risks related to work with affected individuals.37 In this same vein, previous studies showed that epidemics and confinement have already been consistently associated with psychological consequences among healthcare workers.12,13 Our results suggest that participants presenting positive screening for common mental health disorders (anxiety and depression) showed poorer lifestyles than those without, which concurs with previous evidence showing that psychiatric disorders in general are associated with worse lifestyle behaviours.7 Anxiety and especially depression have been associated with worse lifestyles in clinical samples.7 For instance, individuals with higher levels of anxiety showed pronounced changes in sleep quality during the current COVID-19 pandemic.16 The present results expand this relationship to lifestyle as a multidimensional construct, although no definitive answer regarding causality may be stablished, due to the cross-sectional nature of data collection. In addition, it is important to highlight that increased levels of anxiety and depressive symptoms are expected during crisis situations, and the instruments’ cut-off were not validated for people under these circumstances.
Reporting substantial changes on environmental exposures, social support and strategies to cope with stress, on the other hand, were related with a healthier lifestyle. Despite evidence on the role of environmental exposures is still sparse, increased screen time has been recently described during lockdown in Italy.18 Our findings are consistent with the key role of social support as a protective factor during the COVID-19 pandemic16,38 and EVD.17 Beyond social support, stress management is a core lifestyle dimension. Stress is not only directly associated with states of health and disease, but also indirectly associated with other lifestyle behaviours that support wellbeing, such as sleep and physical activity.39 Strong associations have been found between increased stress/impaired sleep quality and lower levels of physical activity and exercise.39,40
In the present study, none of the medical or psychiatric diagnosis was significantly associated with lifestyle after the multivariate analysis. This negative finding may be seen as at odds with the consistent relationship between healthy lifestyles and several NCDs and psychiatric disorders.5–7 However, relationships between chronic conditions and regular lifestyles may differ from their association with lifestyles changes during confinement. Moreover, these inconsistent results may be explained by differences in study design, self-reported versus objective (as per clinical report) diagnoses, and the relatively small sample size of participants reporting previous diagnosis in this survey.
Some additional limitations, beyond those described above, include the non-probabilistic nature of the sample which precludes generalizability of the results to the entire Spanish population. So far, this is a major limitation of all websurveys, and additional research are needed to advance this field of research. In addition, the analysis of lifestyle changes relied on self-reported perception, which is subject to social desirability and memory bias. New technologies, such as personal health trackers, may be useful to overcome these limitations in the future, but under confinement these are difficult to implement. Finally, as any cross-sectional study, inverse causality may not be excluded, and associations must be interpreted with caution.
Despite these limitations, the present study showed most participants reported changes in lifestyle behaviours during the COVID-19 pandemic in Spain. In addition, the Short Multidimensional Inventory Lifestyle Evaluation-Confinement (SMILE-C), was sensitive to detect these changes and presented good psychometric properties. We also highlighted the importance of demographic and clinical factors associated to lifestyle during the COVID-19 self-isolation period. Accordingly, more attention should be paid to changes in lifestyle behaviours during pandemic. The results of this and future studies can be used to fine-tune public health recommendations issued to maintain or adopt healthy lifestyles. Based on the present results, the adoption of high-quality diets and restorative sleep should be emphasized. Moreover, psychological strategies such as social support and home-based stress management should be delivered to the general public under confinement. Finally, campaigns addressed to improve essential workers’ wellbeing must consider lifestyle issues. However, these hypotheses await confirmation by longitudinal studies. Follow-up surveys of the impact of lifestyle changes during pandemic are warranted and clinical trials should examine the efficacy of lifestyle-based interventions to improve citizens’ wellbeing. From our perspective, the present results are timely, strategic, and innovative in the context of current pressure to collect relevant health data under the COVID-19 pandemic.10
Role of the funding sourceThe authors received no financial support from public agencies, private companies or non-profit entities for the research, authorship, and/or publication of this manuscript.
Declaration of transparencyThe corresponding author declares that this manuscript is an honest, accurate and transparent report of the present study, that no relevant aspect of the study has been omitted, and that the differences from the pre-planned study have been explained (and registered, if relevant).
Conflict of interestVBM has been a consultant, advisor or Continuing Medical Education (CME) speaker over the last 3 years for the following companies: Angelini; Ferrer; Lundbeck; Nutrición Médica; and Otsuka. The other authors declare no conflict of interest.
VBM acknowledges the support from Instituto de Salud Carlos III (PI16/1770, PROBILIFE Study). RBDB is grateful for the long term funding from the National Council for Scientific and Technological Development – CNPq (grant # 310541/2017-4) and Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro – FAPERJ (grant # E-26/203.154/2017).
The authors thank Dr Alan C. Logan and Susan Prescott for their valuable contribution as external reviewers of the SMILE questionnaire. We are also thankful to Gabriel Madeira for programming the questionnaire and thoughtful insights in this matter. The authors also thank Dr. Jose Cervera, Dr. Jeferson Goularte and Mrs. Silvia Serafim for their participation in the SMILE project.
FK acknowledges the support from the Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul – FAPERGS (grant #2012551-0000250.0).
The following are the supplementary data to this article: