




The HADS is a questionnaire widely used to evaluate anxiety and depression, although its use in fibromyalgia patients has not yet been reported. The aim of this study is to know the usefulness of the HADS to evaluate the emotional aspects related to fibromyalgia patients.
MethodsThis paper studies a sample of 301 fibromyalgia patients. The scientific goodness of the questionnaire is analysed, and its structure is compared with other models by confirmatory factor analysis. Two external severity indices are used, number of tender points and patient's employment situation.
ResultsThe results show higher levels of anxiety than in other disorders, adequate reliability and a three-factor model with better statistical fit. Nevertheless, this structure was not shown more useful than the two-factor structure for the external criteria studied.
ConclusionsThe HADS has been shown to be a useful tool for exploring the presence of anxiety and depression in fibromyalgia patients and that the number of tender points does not seem to be related to the severity of the psychological aspects measured by the HADS in our sample, while there does seem to be a correspondence between psychological condition and absence from work.
El cuestionario HADS es ampliamente utilizado en la evaluación de la ansiedad y depresión, sin embargo no hay datos sobre su utilización en pacientes de fibromialgia. El objetivo de este estudio es conocer la utilidad del HADS para evaluar los aspectos emocionales presentes en los pacientes de fibromialgia.
MétodoSe estudia a una muestra de 301 pacientes de fibromialgia. Se analiza la bondad cientí-fica del cuestionario y su estructura que es comparada mediante análisis factorial confirmatorio con la obtenida en otras investigaciones. Se utilizan dos índices externos de severidad: número de puntos dolorosos y situación laboral.
ResultadosSe obtienen altos niveles de ansiedad, mayores que en otros trastornos. La fiabili-dad es adecuada y un modelo de 3 factores es el que mejor se ajusta a los datos, no obstante, dicha estructura no parece ser más útil que la de 2 factores, considerando los criterios externos utilizados.
ConclusiónEl HADS se ha mostrado útil para explorar la presencia de ansiedad y depresión en pacientes de fibromialgia. El número de puntos dolorosos no parece estar relacionado con la severidad de los aspectos psicológicos evaluados por el HADS, sin embargo sí parece haber una correspondencia entre estos y la situación laboral de las pacientes.
Fibromyalgia syndrome (FMS) is characterised by heterogeneous symptoms: generalised musculoskeletal pain,1 sleep disorders and various somatic symptoms,2,3 along with emotional disturbances4 that significantly affect the patient's family life overall, as well as their work and personal environments.5 The FMS diagnosis is based on present clinical manifestations in the patient and on the classification criteria6 used to homogenise the populations in clinical studies.
The significance of psychological coping with the illness as well as its emotional aspects have been widely recognised in this syndrome.7 In addition, the relevance of negative moods8 and the influence of these factors throughout the course of the illness have been highlighted. Among the various relevant emotional factors in fibromyalgia, anxiety and depression are the most prominent pathologies associated with the illness. Some authors9 have shown that 60% of fibromyalgia patients suffer from depression. Consequently, the possible presence of anxiety and depression in fibromyalgia patients should be assessed.
The Hospital Anxiety and Depression Scale (HADS)10,11 has been used widely to measure levels of anxiety and depression in samples of patients with arthritis or cancer, women with postpartum depression and patients with traumatic cerebral lesions, among others.12–16 In these samples, good psychometric properties have been observed.14,16,17 Although there are many questionnaires for evaluating depression and anxiety, the HADS is considered useful3 in assessing fibromyalgia. Given the existing overlap between medical and psychological symptoms of the illness, this questionnaire is more appropriate as it focuses on evaluating the cognitive aspects of anxiety and depression,18 thus accrediting its sensitivity as well.14 Despite its usefulness, no studies have been published to date that describe its use with patients with fibromyalgia.
Psychological factors, such as anxiety and depression, should be compared with severity and syndrome development criteria. Objective criteria are not part of patient-completed questionnaires, making clarification of the comparison easier. Even though other authors have questioned the usefulness of considering the number of tender points, the scientific community19 widely accepts the use of this count. The second index is the patient's work situation; this index assesses the severity of the syndrome and shows how it affects the patient's social and personal life.
The objective of this study was to ascertain the usefulness of the HADS in evaluating emotional aspects related to patients with fibromyalgia.
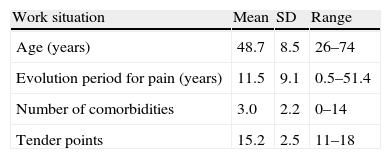
MethodsParticipantsThe sample consisted of a total of 301 patients, 10 males and 291 females, with a mean age of 48.7years. The patients lived in cities and had been diagnosed with fibromyalgia according to classification by the American College of Rheumatology (ACR).6 The sample was recruited from 15 rheumatology clinics across the country. Patients were excluded if they displayed severe functional limitations and cardiovascular or respiratory disorders that limited their aerobic capacity. Patients were also excluded if they suffered from uncontrolled psychiatric disorders, had a legal claim in process related to their illness or were participating in another clinical study at the time. After patients were accepted for the study, they signed an informed consent form to participate. The patients formed part of a broad study20 in which various different questionnaires were used, in addition to an exploratory examination of the symptoms of the illness. Demographic characteristics are presented in Table 1.
Main demographic characteristics found in the inclusion visit of the study in 301 patients with fibromyalgia.
| Work situation | Mean | SD | Range |
| Age (years) | 48.7 | 8.5 | 26–74 |
| Evolution period for pain (years) | 11.5 | 9.1 | 0.5–51.4 |
| Number of comorbidities | 3.0 | 2.2 | 0–14 |
| Tender points | 15.2 | 2.5 | 11–18 |
SD, standard deviation.
The clinical research ethics committee at the Gregorio Marañon Hospital (Madrid, Spain) approved the study protocol.
ProcedureThe study was carried out between January and April of 2007. Data were obtained in 2 stages. In the first, an interview was performed and the patient's clinical history was reviewed to determine their suitability for the study. They were then informed and asked to participate. In the second stage, they were given various different questionnaires and tests, as previously mentioned.
The variables to consider in this study were the HADS scores, the number of tender points—according to the ACR—and the patient's work situation: no occupational disability, temporary occupational disability and permanent occupational disability. The HADS used was the version by Tejero et al.21
Data were analysed with the SPSS program, version 16.0. A confirmatory factor analysis was performed using AMOS version 16 to verify the structure of the scale. The adjustment of data to various different models was studied, including the original 2-factor model proposed by Zigmond and Snaith11 and a series of 3-factor models: McCue et al.22 Dunbar et al.23 Cacci et al.24 and Friedman et al.25 In all the analyses, the goodness-of-fit test (GOF) was statistically significant (P<.001), which revealed that 1 part of the variance was not explained by the model. In addition, other indexes were considered, such as that proposed by Byrne,26 the GOF27,28 and Bentler's29 Comparative Fit Index (CFI) Values higher than 0.90 show a good fit on the CFI, Adjusted Goodness-of-Fit Index (AGFI), Normalised Fit Index (NFI) and CFI indexes.30–32 A value lower than Akaike's Information Criterion (AIC), Root Mean Square Error of Approximation (RMSEA) and Consistent AIC (CAIC) showed good adjustment to the model.32–34
In an effort to study the differences between HADS scores related to the number of tender points and work situation, a t-test analysis was used. A regression analysis was also used to explain the relationship between those variables.
ResultsOn the HADS anxiety scale, patients achieved a mean score of 12.68 with a standard deviation (SD) of 4.35. On the depression scale, the mean score was 10.12 (SD=4.96). Regarding their work situation, a total of 171 patients had not lost their job (56%), 36 were on leave (12%) and the rest were mostly homemakers. Finally, regarding the number of tender points, the mean was 15.23 (SD=2.55, range 11–18). Applying the cut-off values proposed by Snaith and Zigmond10 for anxiety scores, 240 patients (79.7%) showed possibly clinically relevant levels of anxiety (scores of 8 or higher) and 172 (57.1%) showed probably clinically relevant levels of anxiety (score of 11 or higher). Regarding the depression scores, applying the same cut-off points, 169 patients (55.8%) showed possibly clinically relevant levels of depression and 105 (34.9%) showed probably clinically relevant levels of depression.
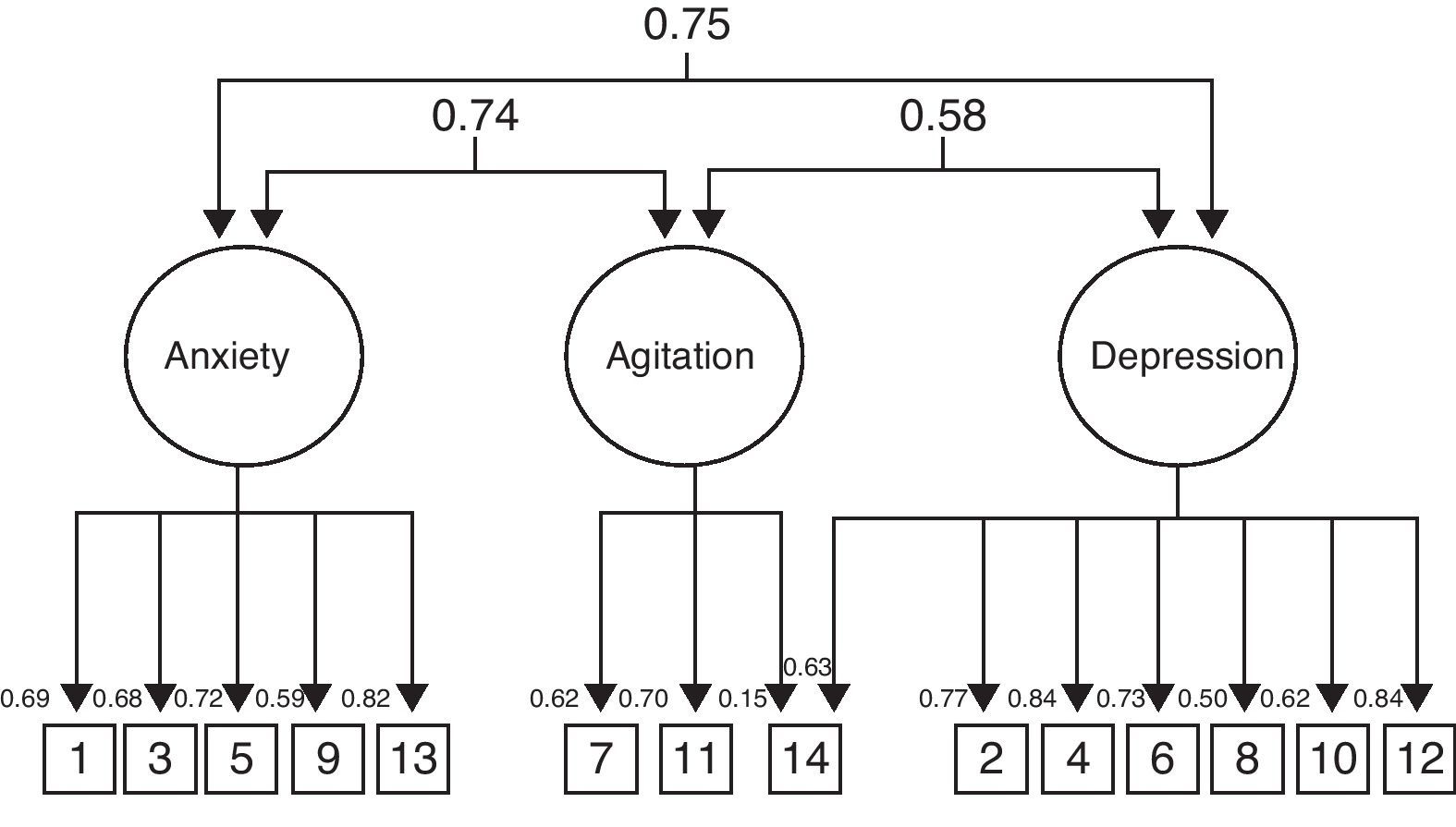
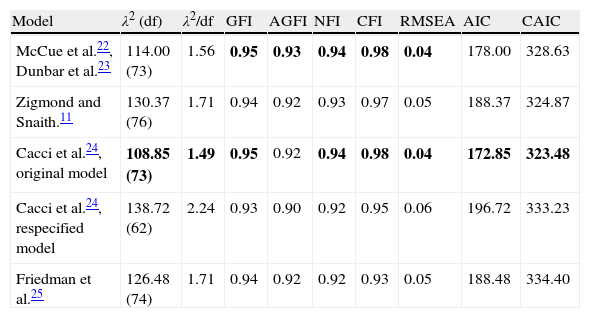
According to the results of the confirmatory factor analysis, shown in Table 2, the model that was best adapted to the data from our study was that proposed by Cacci et al.24 given that it complied with the largest number of goodness-of-fit criteria. This model accounted for the existence of 3 factors designated as anxiety (items 1, 5, 9 and 13), agitation (7, 11 and 14) and depression (2, 4, 6, 8, 10, 12 and 14). The resulting model is presented in Fig. 1.
Structure of the factors from the HADS, determined using fit tests on the models derived from previous factor analysis. All λ2 analyses were statistically significant with a value of P<.001, degrees of freedom in parentheses. The fit indexes of the model are indicated in bold.
| Model | λ2 (df) | λ2/df | GFI | AGFI | NFI | CFI | RMSEA | AIC | CAIC |
| McCue et al.22, Dunbar et al.23 | 114.00 (73) | 1.56 | 0.95 | 0.93 | 0.94 | 0.98 | 0.04 | 178.00 | 328.63 |
| Zigmond and Snaith.11 | 130.37 (76) | 1.71 | 0.94 | 0.92 | 0.93 | 0.97 | 0.05 | 188.37 | 324.87 |
| Cacci et al.24, original model | 108.85 (73) | 1.49 | 0.95 | 0.92 | 0.94 | 0.98 | 0.04 | 172.85 | 323.48 |
| Cacci et al.24, respecified model | 138.72 (62) | 2.24 | 0.93 | 0.90 | 0.92 | 0.95 | 0.06 | 196.72 | 333.23 |
| Friedman et al.25 | 126.48 (74) | 1.71 | 0.94 | 0.92 | 0.92 | 0.93 | 0.05 | 188.48 | 334.40 |

The Cacci et al.24 model was the one best adjusted to the fibromyalgia data.
Reliability was studied with the use of Cronbach's alpha coefficient. A value of 0.83 was obtained for the anxiety subscale and 0.87 for the depression subscale. On the anxiety scale with Cacci et al.’s24 model, a value of 0.79 was obtained for anxiety and 0.63 for agitation. All of the anxiety items showed significant correlations with the complete scale. The depression items also presented a significant correlation with the complete scale. All were positive correlations. The correlation between the anxiety scale and the depression scale was 0.65 (P<.01). On the 3-factor scale, the correlations were 0.63 (P<.01) for the anxiety and agitation scales, 0.65 (P<.01) for the depression and anxiety scales and 0.71 (P<.01) for the depression and agitation scales. The correlation between the anxiety scale with the 2-factor solution and the anxiety and agitation factors was 0.94 (P<.01) and 0.76 (P<.01), respectively.
Tender pointsThe sample was analysed using the number of tender points as a criterion for characterising the syndrome. The distribution of the sample according to this variable was spread out (kurtosis g2=−1.26, which indicates a platykurtic distribution). It was thought that dividing the sample according to the number of tender points would contribute to its segmentation by using a criterion relevant to its own definition as an illness. Three groups were used, corresponding to the 3 quartiles on the distribution of the number of tender points. The first quartile included patients with 15 points or less and the third quartile included patients with 18 points.
2-factor solutionBelow the first quartile, the mean was 12.34 (SD=4.58) on the anxiety scale and 9 (SD=4.79) on the depression scale. On the third quartile, the mean was 12.68 (SD=4.35) for the anxiety scale and 10 (SD=4.96) for the depression scale. The t-test did not identify any statistically significant differences.
In a multiple regression analysis with tender points as a dependent variable and anxiety and HADS depression scores as the independent variables, a model was obtained that included depression but explained a small percentage of variance: R2=0.26, adj. R2=0.22 with a beta of 0.85, t=2.803, P<.005 (CI 95%, 0.025–0.145).
3-factor solutionBelow the first quartile, the mean was 9.1 (SD=3.38) for anxiety and 4.67 (SD=4.1) for agitation. On the third quartile, the mean was 9.3 (SD=1.77) for anxiety and 4.87 (SD=1.97) for agitation. The depression scores were the same as in the 2-factor solution. The t-test did not identify any statistically significant differences.
In a multiple regression analysis with tender points as a dependent variable and HADS scores for anxiety, agitation and depression as independent variables, a model was obtained that included agitation: R2=0.43, adj. R2=0.39 with a beta of 0.274, t=3.648, P<.000 (CI 95%, 0.126–0.422).
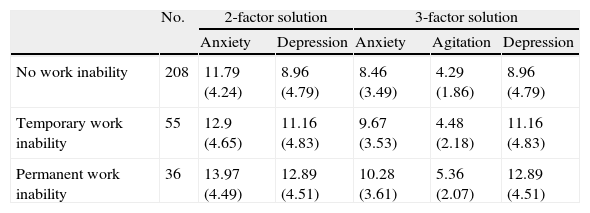
Work situationThe sample was also analysed regarding the patients’ work situations. The descriptive data are presented in Table 3.
HADS scores, mean (standard deviation) according to work situation and factor structure.
| No. | 2-factor solution | 3-factor solution | ||||
| Anxiety | Depression | Anxiety | Agitation | Depression | ||
| No work inability | 208 | 11.79 (4.24) | 8.96 (4.79) | 8.46 (3.49) | 4.29 (1.86) | 8.96 (4.79) |
| Temporary work inability | 55 | 12.9 (4.65) | 11.16 (4.83) | 9.67 (3.53) | 4.48 (2.18) | 11.16 (4.83) |
| Permanent work inability | 36 | 13.97 (4.49) | 12.89 (4.51) | 10.28 (3.61) | 5.36 (2.07) | 12.89 (4.51) |
In the t-test, statistically significant differences were observed regarding depression between no occupational disability and temporary occupational disability (t=−2.694, P<.008, CI 95% −3.803 to −0.589). There were also significant differences between no occupational disability and permanent occupational disability regarding anxiety (t=−2.839, P<.005, CI 95% −3.691 to −0.666) and depression (t=−4.633, P<.000, CI 95% −5.599 to −2.257).
3-factor solutionThere were also significant differences between no occupational disability and temporary occupational disability regarding depression (t=−2.041, P<.008, CI 95% −3.803 to −0.589) and anxiety (t=−2.041, P<.042, CI 95% −1.213 to −0.594). Likewise, there were significant differences between no occupational disability and permanent occupational disability regarding anxiety (t=−2.914, P<.004, CI 95% −1.828 to 0.627), depression (t=−4.633, P<.000, CI 95% −5.599 to −2.257) and agitation (t=−3.157, P<.002, CI 95% −1.073 to 0.340).
The multivariate logistic analysis showed that only depression was associated with work situation: temporary occupational disability (odds ratio 1.16, CI 95% 1.03–1.30) and permanent occupational disability (odds ratio 1.2, CI 95% 1.08–1.33).
DiscussionThis study revealed the usefulness of the HADS questionnaire in its application to patients with fibromyalgia. The confirmatory factor analysis showed that the 3-model factor by Cacci et al.24 gave the best statistical adaptation. This model modified the anxiety scale, identifying the anxiety and agitation scales instead. However, its high correlation with the original scale, as well as its inability to differentiate patients with fibromyalgia brought the usefulness of the structure into question. The Dunbar et al.23 model, based on patients with chronic fatigue, did not add anything to the variables being studied, either. It may thus be more sensible to maintain the 2 original subscales.10,11
The reliability observed according to Cronbach's alpha coefficient was considered appropriate and similar to that observed in other studies.35 The correlations observed between the anxiety and depression scales were also congruent with those indicated in the references,16 all of which verified the usefulness of the HADS in patients with fibromyalgia.
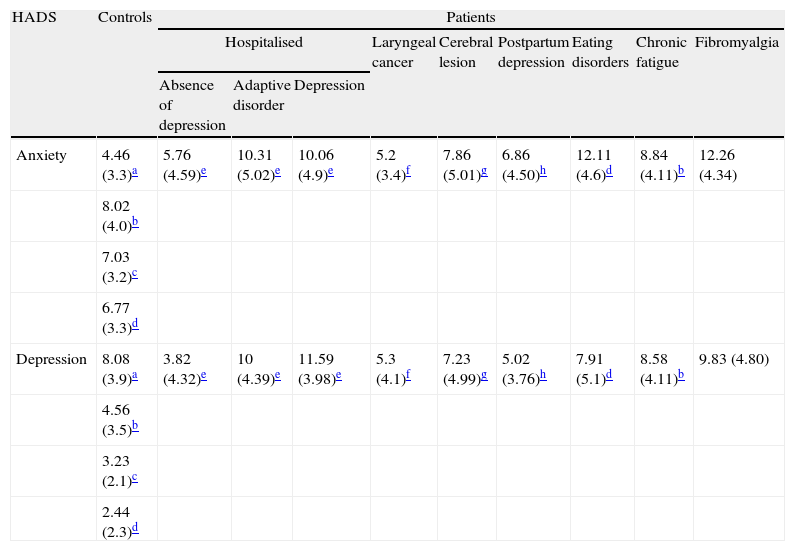
As shown in Table 4, comparing the results in descriptive terms, there were higher levels of anxiety and depression in patients with fibromyalgia compared to the normal population (adults and students). It was even more notable that, in the cases of a physical condition (patients with traumatic cerebral lesions or laryngeal cancer), the levels of anxiety and depression were lower than in patients with fibromyalgia. Still more surprising was the observation that patients with a psychiatric diagnosis (adaptive disorder or depression) presented lower levels of anxiety than patients with fibromyalgia. This was especially interesting because of its practical repercussions for the clinician, as it confirmed the need to assess the psychological aspects of the illness (anxiety and depression), given the high levels in these patients compared to those in other samples.
Mean (standard deviation) of the scores from the anxiety and depression scales on the HADS in published studies with different samples and observed mean in this study of patients with fibromyalgia.
| HADS | Controls | Patients | ||||||||
| Hospitalised | Laryngeal cancer | Cerebral lesion | Postpartum depression | Eating disorders | Chronic fatigue | Fibromyalgia | ||||
| Absence of depression | Adaptive disorder | Depression | ||||||||
| Anxiety | 4.46 (3.3)a | 5.76 (4.59)e | 10.31 (5.02)e | 10.06 (4.9)e | 5.2 (3.4)f | 7.86 (5.01)g | 6.86 (4.50)h | 12.11 (4.6)d | 8.84 (4.11)b | 12.26 (4.34) |
| 8.02 (4.0)b | ||||||||||
| 7.03 (3.2)c | ||||||||||
| 6.77 (3.3)d | ||||||||||
| Depression | 8.08 (3.9)a | 3.82 (4.32)e | 10 (4.39)e | 11.59 (3.98)e | 5.3 (4.1)f | 7.23 (4.99)g | 5.02 (3.76)h | 7.91 (5.1)d | 8.58 (4.11)b | 9.83 (4.80) |
| 4.56 (3.5)b | ||||||||||
| 3.23 (2.1)c | ||||||||||
| 2.44 (2.3)d | ||||||||||
The mean anxiety score was higher than that observed in other studies. Of all those reviewed, only 1 study36—performed with eating disorder patients—showed a similar figure: 12.11 (4.69) compared to 12.26 (4.34) in our study. It should also be considered that our study included a patient population consisting of practically all females. This could be a factor to consider, since other authors24 have observed higher scores in females (8.57) compared to males (6.74), with a statistically significant difference. Consequently, can not only the type of illness be relevant (fibromyalgia or eating disorders) but also the sex of the patient.
The data obtained regarding depression were in accordance with those from other authors. McCue et al.22 observed similar scores in their study of patients with chronic fatigue, in that 55% of the patients presented possibly clinically relevant levels of depression and 32% presented probably clinically relevant levels of depression, compared with the 55.8% and 34.9% observed in our study. The depression scale seemed to be more stable and less subject to influence of the patient's sex (see Ref.24).
The usefulness of the HADS in clarifying the complexity of fibromyalgia syndrome depends on the state of emotional factors in this syndrome. In our study, significant differences were not observed regarding anxiety and depression when the number of tender points was used as a criterion. The regression analysis accounted for all subjects, not just those in the outermost quartiles. This analysis revealed a relationship between tender points and depression (2-factor solution), as well as depression, anxiety and agitation (3-factor solution). In this case, dividing the original anxiety scale could help clarify the relationship between emotional state and work situation.
This showed that the number of tender points truly corresponds to the patient's emotional state in the terms assessed by the questionnaire, although the relationship is weak. In line with those indicated in the Thieme et al.37 study, our data seemed to suggest that anxiety and depression in fibromyalgia were relatively independent of other physical factors associated with the syndrome.
Other studies, such as that of McCracken et al.38 have observed a relationship between disability and specific measurements of anxiety and fear of pain. However, the disability scores obtained by McCracken were based on the patients’ self-assessments. In our study, the determination of tender points was an objective procedure. Axford et al.12 observed that measurements of anxiety and depression with the HADS were not good predictors of arthritis severity determined by a radiological score. However, the Western Ontario and McMaster Universities Osteoarthritis (WOMAC) Index showed that anxiety and depression had a weak association with disability, which was measured by self-assessments. In our study, we obtained a weak relationship, and this relationship was stronger when the HADS anxiety scale was completed, differentiating the specific components of anxiety and agitation.
Nonetheless, an interesting result relevant to the patients’ work situations was that the lack of work assistance correlated with the presence of anxiety and depression. It seemed that in this case, the more serious the work situation, the higher the levels of anxiety and depression measured by the HADS. The presence of depression in fibromyalgia seemed to be explained by learning principles: the loss of reinforcements produced by the difficulties in leading a normal life and the anticipation of pain can cause behavioural inhibition. This, in turn, leads to a loss of reinforcements.
Another question of interest is the consideration of the HADS structure. Some authors argue that the 3-dimensional structure, which corresponds to Clark and Watson's39 3-part model is better. Surely, from a statistical point of view, the confirmatory factor analysis provides better adjustment for the 3-factor model. However, these indexes cannot be considered determinant, since they themselves show inconsistencies, such as the χ2, for example. It may be necessary to compare the usefulness of the 3-factor HADS with external criteria. In our study, the 3 exploratory factors were a bit more useful than the 2 conventional factors in differentiating the number of tender points or the patients’ work situations. The 3-factor model may be more useful, as shown in McCue et al.22 but this should be justified by data. Meanwhile, the application of the 2 classical factors may be more prudent. Another reason to maintain this orthodox position is the existing empirical support for the 2-factor structure and its extensive use.15–17,36,40–42
The sample was recruited in different public and private hospitals throughout Spain. The objective was to make it representative of the country's population of patients with fibromyalgia. There is a broad representation of public hospitals (see the ICAF [Combined Index of Severity of Fibromyalgia] group in the declaration of interests and acknowledgments paragraph), but it is possible that this sample was not representative of all patients with fibromyalgia.
Another aspect that requires more research is the role and possible influence of the patient's sex on anxiety. It would be necessary to determine to what extent these high scores are due to the patients’ suffering from fibromyalgia. The influence of sex—not only in mean scores but also in the scale structure itself—should also be determined. At the same time, the high anxiety scores show that the emotional impact of the illness should be acknowledged.
The sample in this study was formed by 291 females and 10 males. This proportion reflects that which normally exists between men and women in the patient population with fibromyalgia syndrome.
This study showed the usefulness of the HADS in evaluating patients with fibromyalgia, but was not designed to validate this instrument. The HADS has been validated in the Spanish population.17 The objective of this study was to ascertain its usefulness in evaluating emotional aspects relevant to patients with fibromyalgia.
ConclusionsIn short, it is possible to conclude, firstly that the HADS is a sensitive instrument for explaining the presence of anxiety and depression in patients that suffer from fibromyalgia. Secondly, the number of tender points did not seem to be related to the severity of the psychological aspects measured with the HADS in our sample. However, there certainly seemed to be a correspondence between the patients’ psychological states and the lack of work assistance.
Ethical disclosuresHuman and animal protection. The authors declare that the procedures followed conformed to the ethical norms of the human experimentation committee and were in accordance with the World Medical Association and the Declaration of Helsinki.
Data confidentiality. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
FundingThis research was funded by a grant from Pfizer Laboratory and the Health Research Fund (FIS in Spanish) PI 07/0202.
Conflict of interestsThe authors have no conflict of interests to declare.
We wish to thank Milena Gobbo, the group members from the ICAF study and the Spanish Rheumatology Foundation Research Unit, for their technical help.
Members of the ICAF study group: C. Alegre (Vall de Hebrón Hospital, Barcelona), M. Alperi (Asturias General Hospital, Oviedo), F.J. Ballina (Asturias General Hospital, Oviedo), R. Belenguer (October 9 Hospital, Valencia), M. Belmonte (Castellón General Hospital, Castellón), J. Beltrán (Castellón General Hospital, Castellón), J. Blanch (IMAS Hospital, Barcelona), A. Collado (Clinical Hospital, Barcelona), P. Fernández-Dapica (October 12 Hospital, Madrid), F.M. Hernández (Dr. Negrín Hospital, Gran Canaria), A. García-Monforte (Gregorio Marañón Hospital, Madrid), T. González-Hernández (IPR, Madrid), J. González-Polo (La Paz Hospital, Madrid), C. Hidalgo (Rheumatology Centre, Salamanca), J. Mundo (Clinical Hospital, Barcelona), P. Muñoz-Carreño (General Hospital, Guadalajara), R. Queiró (Asturias General Hospital, Oviedo), N. Riestra (Asturias General Hospital, Oviedo), M. Salido (CLINISAS Clinic, Madrid), I. Vallejo (Clinical Hospital, Barcelona), J. Vidal (General Hospital, Guadalajara).
Please cite this article as: Vallejo MA, et al. Uso del cuestionario Hospital Anxiety and Depression Scale (HADS) para evaluar la ansiedad y la depresión en pacientes con fibromialgia. Rev Psiquiatr Salud Ment (Barc.). 2012;5:107–14.