



The purpose of this study was to compare the methods of Willems et al. (WI and WII) in estimating the forensic age in Venezuelan children.
Material and methodsA retrospective and observational study was performed on 516 orthopantomographs of individuals of both genders (6–18 years) in order to evaluate the stages of dental maturation described by Demirjian et al. Using the dental age (DA) in the seven left inferior teeth, DA was calculated using the WI and WII methods. The mean difference between the chronological age (CA) and DA was calculated using a paired-sample t-test.
ResultsThe under-estimation of age by both methods (0.17±1.75 years) was observed, with the CA–DA difference being statistically significant (p=.04). Considering all age groups, WII showed the smallest difference between CA–DA (0.05±1.40 years) in girls, while a smaller difference was found for WI (0.04±0.54 years) for boys. In a subsample up to the age of 16, there was an under-estimation of age in females for WI (0.03±1.23 years) and an over-estimation for WII (−0.18±1.24 years). In the males both methods over-estimated the age (W1=−0.21±1.17 years, WII=−0.06±1.20 years).
ConclusionsThe accuracy of the methods varied according to gender and age group: however, both were applicable to the studied sample.
El presente trabajo tuvo como objetivo comparar los métodos de Willems et al. (WI y WII) en la estimación forense de la edad en niños venezolanos.
Material y métodosEsta investigación fue de tipo retrospectiva y observacional. Se emplearon 516 ortopantomografías de individuos de ambos sexos (6-18 años), se asignaron los estadios de maduración dental descritos por Demirjian et al. en los 7 dientes inferiores izquierdos, para luego determinar la edad dental (ED) mediante WI y WII. Se calculó la diferencia de media entre la edad cronológica (EC) y la ED estimada mediante una prueba «t» de Student para muestras relacionadas.
ResultadosPara el total de la muestra se observó la subestimación de la edad por ambos métodos (0,17±1,75 años), siendo la diferencia EC-ED estadísticamente significativa (p=0,04). Considerando todos los grupos de edad, WII mostró la menor diferencia EC-ED (0,05 años±1,40) en el sexo femenino, mientras que para el masculino se encontró menor diferencia para WI (0,04±0,54 años). En una submuestra hasta los 16 años se evidenció una subestimación de la edad en el sexo femenino para WI (0,03±1,23 años) y una sobreestimación para WII (−0,18±1,24 años), en el sexo masculino ambos métodos sobreestimaron la edad (W1=−0,21±1,17; WII=−0,06±1,20 años).
ConclusionesLa precisión de los métodos varió de acuerdo al sexo y grupo de edad, sin embargo, ambos resultaron aplicables a la muestra estudiada.
Dental age (DA) calculated by radiographic assessment of the development of teeth is considered to be a reliable marker of chronological age (CA)1–4 due to dental maturation presenting a predictable course, being strongly controlled by genetics and being less impacted by local and systemic factors.3,5–8 DA has been used in paediatric endocrinology, archaeology, and is of particular interest in paediatric dentistry and dentistry occlusion development management and its relationship with craniofacial growth. In the forensic sciences DA is used to calculate age in children and teenagers without any valid identification documents or who are deceased, or who are involved in civil, criminal or administrative processes.1,2,4,9–17
Most methods proposed for the calculation of DA aimed at a radiomorphological focus assess the changes which occur in the tooth bud of the permanent tooth, from the formation of the bony crypt to the apical closure. These changes are divided into stages or phases of maturation, which are sequential and observable in individuals of both sexes.5,9,18 The Demirjian et al.5 method has been extensively applied, with an over and under estimation of age being found. This has resulted in the suggestion for its population adaptation to improve the accurateness of estimation.4,8,10,12,16,19 This method shows 8 stages of maturation ranging for letters A to H, which represent the formation of 7 left inferior teeth, excluding the third molar. Each stage is given a score and these scores are added up for the result which is called the dental maturation index, transformed into DA using reference tables for each gender.5
In 2001 Willems et al.20 (WI) adapted the Demirjian et al.5 method to a sample of Belgian origin, although his proposal maintained the Demirjian et al.5 maturation stages. However, a weighed variance analysis was applied which enabled conversion tables to be constructed from stages to scores which provided values expressed directly in years, and these had to be added together to obtain the DA; as a result the calculation of the DA is simplified due to the fact no additional tables are required to transform the dental maturation index to DA, as in the Demirjian et al.5 method. The authors published a new reference table for 2010 (WII), taking into consideration both sexes together, suggesting that this could be used when the sex of the individual was unknown.21 The Willems et al.20,21 method has been validated in many countries (Saudi Arabia,22 Bosnia,23 Braxil,24,25 China,12 Egypt,26 France,10 India,1,7,11,13,27–31 England,1 Italy,6 Kenia,14 Korea,32 Kosovo,15 Macedonia,3 Malasia,2,33,34 Serbia,35,36 Somalia,16 South Africa,8,37 Thailand,19 Turkey17,38,39 and Venezuela40). In a recent meta-analysis a consistent underestimation of age within a range of −.04 to −.02 years4 was reported.
Considering that there is very little information on the applicability of the methods of Willems et al.20,21 in Latin American, the aim of this study was to compare the WI20 and WII21 methods for age estimation in a sample of individuals from Maracaibo, Zulia state, Venezuela, for forensic purposes.
Material and methodsThe following study was retrospective and observational. It was undertaken in the Area of Forensic Dentistry of the Institute of Research, at the Dentistry Faculty of the University of Zulia, Maracaibo, Venezuela. A non-probability and intentional sample of 516 orthopantomographs of individuals of both sexes (273 female and 243 males) was used for this study. They were aged chronologically between 6 and 18 years, and belonged to patients who had presented at the Comprehensive Facility for Childhood Care and were selected from the file in the dentistry area, with the following inclusion criteria. Absence of systemic diseases; height and weight in keeping with the CA in accordance with the person's medical history; contrast imaging with appropriate density and minimal distortion; the presence of the 7 lower left permanent teeth, or when teeth were missing the opposite side of the mouth was considered; absence of extended diseases and anomalies of number, shape, size or position which could alter the odontogenesis.
The orthopantomographs were indicated for clinical reasons, so that there was no additional exposure of the subject to ionizing radiation for this study, in accordance with the directives of the declaration of Helsinski41 for the study of human beings, and the anonymity of the subjects was guaranteed. Also, the parents or representatives of the individuals signed an informed consent form on data use contained in medical files and additional tests, for teaching or research purposes.
For statistical purposes, the age groups contained at least 10 individuals with differences of 11 months in each group with the result that the group aged 6, for example, comprised individual from 6 years to 6 years and 11 months. Real age was determined by subtracting the birth date from the date when the radiography was obtained and expressed in years and decimals of years. The selected radiographies in the Comprehensive Facility for Childhood Care were digitalized by a camera (Sony Cyber-shot DSC-W650, Sony Corporation, Tokyo, Japan) with a resolution of 300dpi. The images were stored on a computer and were transformed to a scale of greys for analysis. The orthopantomographs selected from the file of the area of forensic dentistry were physically available for evaluation.
The digital images were observed using Adobe Photoshop software, version CS6 (Adobe System Incorporated, San José, CA, USA) and the assessor was provided with resources on shine, contrast and magnification. The standard orthopantomographs were placed on a desktop X-ray viewer, with a matt black mask for improving observation, in a tenuous light and the observer was able to use a magnifying glass with magnification of 2×. Due to the Demirjian et al.5 method being morphological, no adjustment was required to standardize both types of images.
Both digital and standard orthopantomographs were assessed by 2 observers who had both been trained and who only knew the sex of the individual, so that when discrepancies arose in the assignation of the stages, they could reach an agreement and the final DA was calculated, for which it was not necessary to estimate the inter or intraobserver reliability.
The maturation of the 7 teeth studies was assessed using the stages of maturation proposed by Demirjian et al.,5 and then applying the reference tables of the WI20 and WII21 methods to transform the stages in scores and add them together to obtain the respective dental ages.
Statistical analysis of the data was performed through the software SPSS, version 15.0 (Statistical Package for the Social Science, SPSS Inc., Chicago, IL, USA). Descriptive statistics were calculated (mean and standard deviation) of the CA and the estimated dental ages, for the total of the sample and the age groups in both sexes. The mean differences between the CA and the dental ages were calculated by the Student's t-test for related samples in the total sample and the age groups. The differences between the sexes relating to the DA estimated by the methods, was calculated using the Student's t-test for separate samples. In this study a negative symbol then denoted an overestimation of age and a positive symbol denoted an underestimate of age. The accepted level of significance was p<.05.
ResultsThe CA mean for the total sample was 12.23 years (±3.43) and 12.05 years (±1.75) for estimated dental ages, both for the WI11 and WII12 methods. The mean differences between CA and ages calculated by the methods were .17 ±1.75), which was statistically significant. A positive and significant correlation was also found between these variables (WI20 .92 p=.000; WII21 .90 p=.000).
Considering the total children, the mean of the CA was 12.29 years (±3.36), a mean of the CA calculated by WI was observed of 12.01years (±2.82), and an underestimation of age was therefore shown, with the difference between the CA and the estimated CA (.28±1.38 year), which was statistically significant (p<.000). For WII21 an underestimation of age was observed (12.23±2.76), with the difference between the CA and the estimated DA (.05±1.40) not being significant (p=.489).
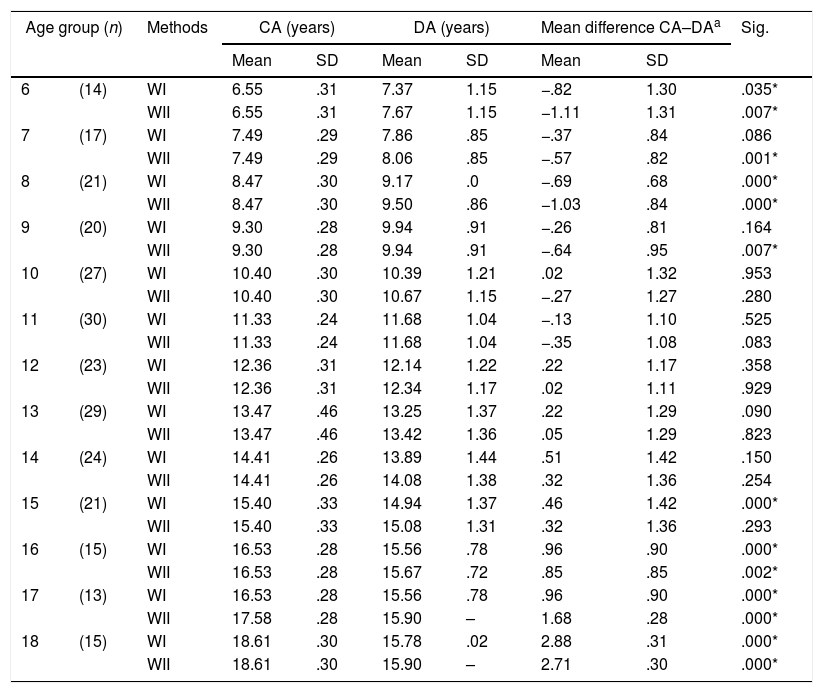
Table 1 presents the mean differences found between the CA and the DA calculated through WI20 and WII21 for women. It may be observed that for WI20 there was an overestimation of age in the youngest age groups (6–9 years), varying from −.26 to −.82 years, the difference between the CA and the DA was significant in the groups aged between 6 and 8 years. From 9 years of age upwards there was shown to be an underestimation of age, ranging from .015 to 2.8 years. Differences were significant from 16 years, with the exception of the group aged 11 years. Regarding WII21 an overestimation of age between 6 and 11 years was confirmed, varying between −.27 and −1.11 years, and with a statistically significant difference in the groups aged 6–9 years. From 12 years upwards underestimation of age was observed (.02–2.71 years) and from 16 years upwards the estimated difference between the CA and the DA was significant.
Comparison of chronological age and dental age estimated by the Willems I and Willems II methods by age, female sex.
| Age group (n) | Methods | CA (years) | DA (years) | Mean difference CA–DAa | Sig. | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||||
| 6 | (14) | WI | 6.55 | .31 | 7.37 | 1.15 | −.82 | 1.30 | .035* |
| WII | 6.55 | .31 | 7.67 | 1.15 | −1.11 | 1.31 | .007* | ||
| 7 | (17) | WI | 7.49 | .29 | 7.86 | .85 | −.37 | .84 | .086 |
| WII | 7.49 | .29 | 8.06 | .85 | −.57 | .82 | .001* | ||
| 8 | (21) | WI | 8.47 | .30 | 9.17 | .0 | −.69 | .68 | .000* |
| WII | 8.47 | .30 | 9.50 | .86 | −1.03 | .84 | .000* | ||
| 9 | (20) | WI | 9.30 | .28 | 9.94 | .91 | −.26 | .81 | .164 |
| WII | 9.30 | .28 | 9.94 | .91 | −.64 | .95 | .007* | ||
| 10 | (27) | WI | 10.40 | .30 | 10.39 | 1.21 | .02 | 1.32 | .953 |
| WII | 10.40 | .30 | 10.67 | 1.15 | −.27 | 1.27 | .280 | ||
| 11 | (30) | WI | 11.33 | .24 | 11.68 | 1.04 | −.13 | 1.10 | .525 |
| WII | 11.33 | .24 | 11.68 | 1.04 | −.35 | 1.08 | .083 | ||
| 12 | (23) | WI | 12.36 | .31 | 12.14 | 1.22 | .22 | 1.17 | .358 |
| WII | 12.36 | .31 | 12.34 | 1.17 | .02 | 1.11 | .929 | ||
| 13 | (29) | WI | 13.47 | .46 | 13.25 | 1.37 | .22 | 1.29 | .090 |
| WII | 13.47 | .46 | 13.42 | 1.36 | .05 | 1.29 | .823 | ||
| 14 | (24) | WI | 14.41 | .26 | 13.89 | 1.44 | .51 | 1.42 | .150 |
| WII | 14.41 | .26 | 14.08 | 1.38 | .32 | 1.36 | .254 | ||
| 15 | (21) | WI | 15.40 | .33 | 14.94 | 1.37 | .46 | 1.42 | .000* |
| WII | 15.40 | .33 | 15.08 | 1.31 | .32 | 1.36 | .293 | ||
| 16 | (15) | WI | 16.53 | .28 | 15.56 | .78 | .96 | .90 | .000* |
| WII | 16.53 | .28 | 15.67 | .72 | .85 | .85 | .002* | ||
| 17 | (13) | WI | 16.53 | .28 | 15.56 | .78 | .96 | .90 | .000* |
| WII | 17.58 | .28 | 15.90 | – | 1.68 | .28 | .000* | ||
| 18 | (15) | WI | 18.61 | .30 | 15.78 | .02 | 2.88 | .31 | .000* |
| WII | 18.61 | .30 | 15.90 | – | 2.71 | .30 | .000* | ||
SD: standard deviation; Sig.: significance (p≤.05).
Regarding males, a mean CA of 12.16 years (±3.51) was verified. The estimated DA mean by WI20 was 12.11 years (±2.97), showing an underestimation of age, with an estimated significant difference between CA and DA (.04±.57 years, p<.000). Regarding WII21 the mean of the DA was 11.85 years (±3.00), with the age underestimated, the difference found between CA and DA (.30±1.31 years) was significant (p<.000).
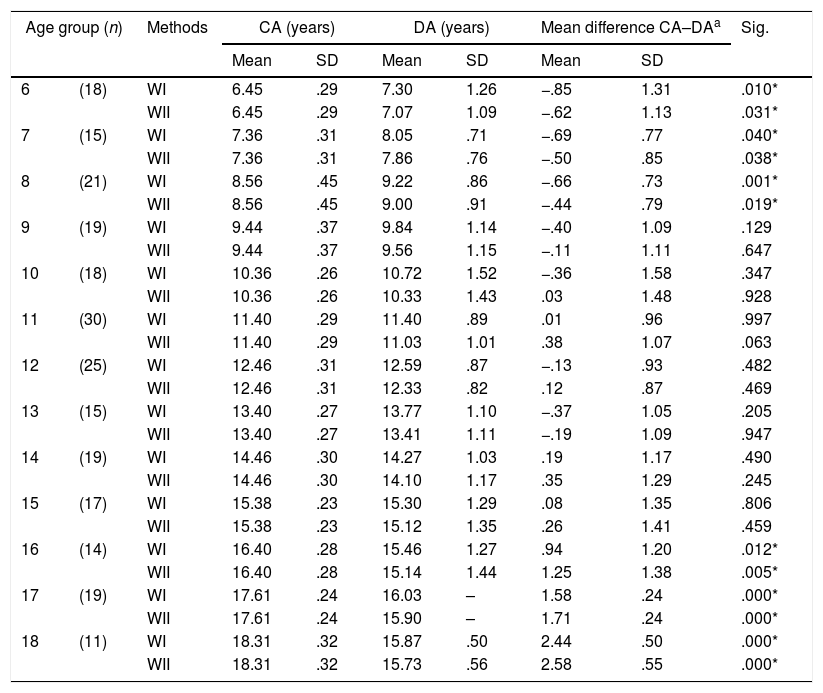
Observation of the results for WI20 in the age groups (Table 2) showed an overestimation between the ages of 6 and 13 years (−.37 to −.85 years), with the estimated difference between the CA and the ED being significant in the groups from 6 to 8 years. In general, an underestimation of the age from 14 years (.08–2.44 years) was observed. The mean different between CA and DA was significant from 16 years onwards.
Comparison of estimated chronological age and dental age by the Willems I (WI) and Willems II (WII) method by age, male sex.
| Age group (n) | Methods | CA (years) | DA (years) | Mean difference CA–DAa | Sig. | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||||
| 6 | (18) | WI | 6.45 | .29 | 7.30 | 1.26 | −.85 | 1.31 | .010* |
| WII | 6.45 | .29 | 7.07 | 1.09 | −.62 | 1.13 | .031* | ||
| 7 | (15) | WI | 7.36 | .31 | 8.05 | .71 | −.69 | .77 | .040* |
| WII | 7.36 | .31 | 7.86 | .76 | −.50 | .85 | .038* | ||
| 8 | (21) | WI | 8.56 | .45 | 9.22 | .86 | −.66 | .73 | .001* |
| WII | 8.56 | .45 | 9.00 | .91 | −.44 | .79 | .019* | ||
| 9 | (19) | WI | 9.44 | .37 | 9.84 | 1.14 | −.40 | 1.09 | .129 |
| WII | 9.44 | .37 | 9.56 | 1.15 | −.11 | 1.11 | .647 | ||
| 10 | (18) | WI | 10.36 | .26 | 10.72 | 1.52 | −.36 | 1.58 | .347 |
| WII | 10.36 | .26 | 10.33 | 1.43 | .03 | 1.48 | .928 | ||
| 11 | (30) | WI | 11.40 | .29 | 11.40 | .89 | .01 | .96 | .997 |
| WII | 11.40 | .29 | 11.03 | 1.01 | .38 | 1.07 | .063 | ||
| 12 | (25) | WI | 12.46 | .31 | 12.59 | .87 | −.13 | .93 | .482 |
| WII | 12.46 | .31 | 12.33 | .82 | .12 | .87 | .469 | ||
| 13 | (15) | WI | 13.40 | .27 | 13.77 | 1.10 | −.37 | 1.05 | .205 |
| WII | 13.40 | .27 | 13.41 | 1.11 | −.19 | 1.09 | .947 | ||
| 14 | (19) | WI | 14.46 | .30 | 14.27 | 1.03 | .19 | 1.17 | .490 |
| WII | 14.46 | .30 | 14.10 | 1.17 | .35 | 1.29 | .245 | ||
| 15 | (17) | WI | 15.38 | .23 | 15.30 | 1.29 | .08 | 1.35 | .806 |
| WII | 15.38 | .23 | 15.12 | 1.35 | .26 | 1.41 | .459 | ||
| 16 | (14) | WI | 16.40 | .28 | 15.46 | 1.27 | .94 | 1.20 | .012* |
| WII | 16.40 | .28 | 15.14 | 1.44 | 1.25 | 1.38 | .005* | ||
| 17 | (19) | WI | 17.61 | .24 | 16.03 | – | 1.58 | .24 | .000* |
| WII | 17.61 | .24 | 15.90 | – | 1.71 | .24 | .000* | ||
| 18 | (11) | WI | 18.31 | .32 | 15.87 | .50 | 2.44 | .50 | .000* |
| WII | 18.31 | .32 | 15.73 | .56 | 2.58 | .55 | .000* | ||
SD: standard deviation; Sig.: significance (p≤.05).
For WII21 overestimation of age between 6 and 9 years was observed (−.11 to −.62 years), which was statistically significant for the groups aged from 6 to 8 years. From 10 years onwards underestimation of age was verified (.03–2.58 years), with the exception of the group aged 13 years, since the differences between CA and DA estimated by the method were significant from 16 years upwards.
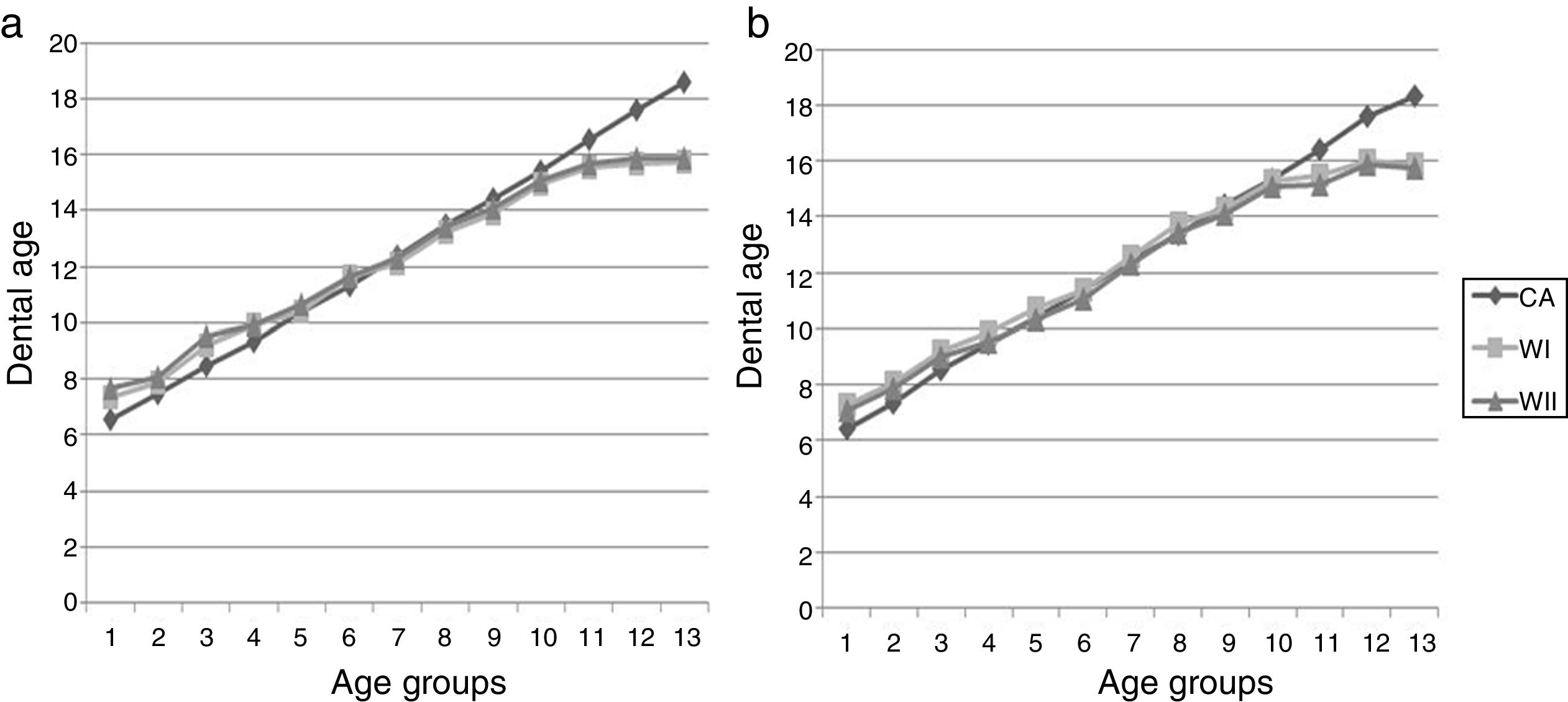
WI20 and WII21 estimated CA and DA ratios may be observed in Fig. 1. In both sexes WI20 and WII21 overestimate the age in the younger age groups, whilst in puberty the dental ages are close to CA. At around 15 years of age there is evidence of age underestimation.
 and dental ages estimated using the Willems et al. methods in their original version (WI) and the modified version (WII). (a) Female sex; (b) male sex.")
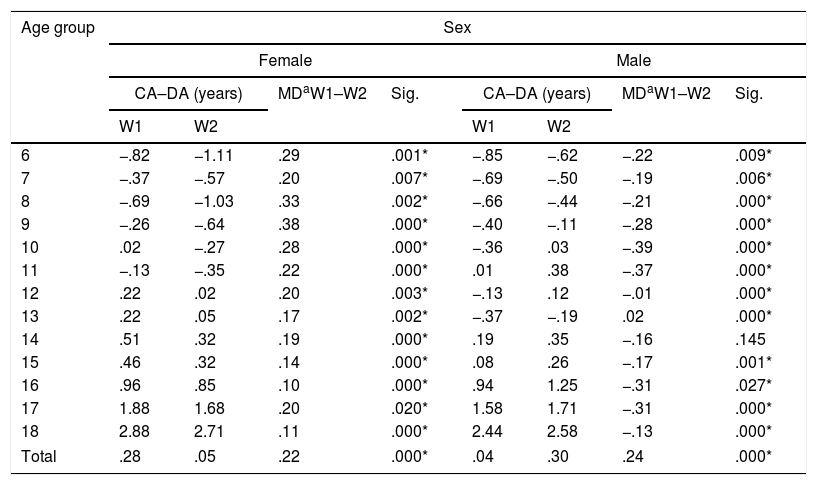
Studying the difference between the sexes with regard to estimated dental ages using WI20 and WII21, reveals that the ages estimated for females were higher than those for males, with statistically significant differences being shown for the age groups of 9, 11, 14, 17 and 18 years when WI20 was used and in the groups aged 16, 17 and 18 years when WII21 was applied.
Considering the total of females, both methods underestimated the age, with this underestimation being lower for WII21; for the males the underestimation observed was lower for WI20 (Table 3). All the differences between CA and DA obtained through WI20 and WII21 in the age groups of both sexes were statistically significant.
Inter method comparison of the mean difference between chronological age (CA) and dental age (DA) estimated using the Willems I (WI) and Willems II (WII) methods by sex and age group.
| Age group | Sex | |||||||
|---|---|---|---|---|---|---|---|---|
| Female | Male | |||||||
| CA–DA (years) | MDaW1–W2 | Sig. | CA–DA (years) | MDaW1–W2 | Sig. | |||
| W1 | W2 | W1 | W2 | |||||
| 6 | −.82 | −1.11 | .29 | .001* | −.85 | −.62 | −.22 | .009* |
| 7 | −.37 | −.57 | .20 | .007* | −.69 | −.50 | −.19 | .006* |
| 8 | −.69 | −1.03 | .33 | .002* | −.66 | −.44 | −.21 | .000* |
| 9 | −.26 | −.64 | .38 | .000* | −.40 | −.11 | −.28 | .000* |
| 10 | .02 | −.27 | .28 | .000* | −.36 | .03 | −.39 | .000* |
| 11 | −.13 | −.35 | .22 | .000* | .01 | .38 | −.37 | .000* |
| 12 | .22 | .02 | .20 | .003* | −.13 | .12 | −.01 | .000* |
| 13 | .22 | .05 | .17 | .002* | −.37 | −.19 | .02 | .000* |
| 14 | .51 | .32 | .19 | .000* | .19 | .35 | −.16 | .145 |
| 15 | .46 | .32 | .14 | .000* | .08 | .26 | −.17 | .001* |
| 16 | .96 | .85 | .10 | .000* | .94 | 1.25 | −.31 | .027* |
| 17 | 1.88 | 1.68 | .20 | .020* | 1.58 | 1.71 | −.31 | .000* |
| 18 | 2.88 | 2.71 | .11 | .000* | 2.44 | 2.58 | −.13 | .000* |
| Total | .28 | .05 | .22 | .000* | .04 | .30 | .24 | .000* |
MD: mean difference; Sig.: significance (p≤.05).
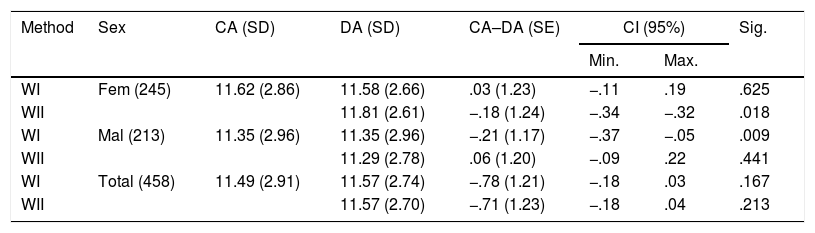
Due to the fact that the individuals of the 17 and 18 age groups reached 100% of dental maturation, a Student's t-test was performed for related samples, including the groups from 6 to 16 years (Table 4). An underestimation of age in the female sex was observed for WI20 and an overestimation for WII.21 In the latter the CA–DA difference was significant, and in the male sex both method overestimated age.
Means and difference of mean between chronological age and dental age estimated by the different methods studied, up to 16 years.
| Method | Sex | CA (SD) | DA (SD) | CA–DA (SE) | CI (95%) | Sig. | |
|---|---|---|---|---|---|---|---|
| Min. | Max. | ||||||
| WI | Fem (245) | 11.62 (2.86) | 11.58 (2.66) | .03 (1.23) | −.11 | .19 | .625 |
| WII | 11.81 (2.61) | −.18 (1.24) | −.34 | −.32 | .018 | ||
| WI | Mal (213) | 11.35 (2.96) | 11.35 (2.96) | −.21 (1.17) | −.37 | −.05 | .009 |
| WII | 11.29 (2.78) | .06 (1.20) | −.09 | .22 | .441 | ||
| WI | Total (458) | 11.49 (2.91) | 11.57 (2.74) | −.78 (1.21) | −.18 | .03 | .167 |
| WII | 11.57 (2.70) | −.71 (1.23) | −.18 | .04 | .213 | ||
CA: chronological age; DA: dental age; SD: standard deviation; Fem: female; CI: confidence interval; Mal: male; Max.: maximum; Min.: minimum; Sig.: significance (p<.05).
DA estimation is required for clinical and forensic purposes,1,2,4,9–17 and for the latter the precision of the method used is particularly essential, i.e. the extent to which the difference between the estimated age and real age of the individual is closest to 0.2,10 The more accurate the method, the better it would be considered applicable to individuals whose age is unknown. In practice a difference of ±.5 to ±1 year between these ages is considered an acceptable limit during age diagnosis procedures for individuals in growth stages of development.16
It has been reported that using the Willems et al.20,21 method in different populations shows a consistent overestimation of age,2,4,10,39 with the magnitude of difference between CA and DA being lower than that used by other methods such as the Demirjian et al.1,2,10,39 Furthermore, improvement in the precision of the Willems et al.20,21 method relating to the results obtained with that of Demirjian et al.5 was expected since the existence of a difference of almost 30 years between the French-Canadian sample used by standardization of the same and that of the Willems et al.,20,21 which seems to reflect the positive secular tendency in human growth and development.10,39
This study researched the applicability of the Willems et al.20,21 methods in estimation of DA for forensic purposes in a sample of Venezuelan origin from the North West of the country. Considering the total sample the age was subestimated by .17 years by both methods but in the results obtained in the subsample of individuals aged under or 16 years of age an overestimation of age was observed, and this is consistent with other reports in the literature.2,3,6,8,10,13,16,23,25,28
When the WI20 method was applied in girls the value of the CA–DA difference in the subsample was lower than that observed in subjects originating from China12 (.54 years), India7 (.69), Kosovo15 (.14 years) and Korea32 (.15 years) and similar to that reported by Maber1 in Bangladeshi and British Caucasian ethnic origin children (.05 years). In males the mean difference observed between CA and DA calculated through WI20 was lower than that reported in individuals in Brazil24 (−.38 years), Bosnia23 (−.42 years), India11,31 (−.49 years and −.7 years, respectively), Macedonia3 (−.52 years), Malasia2,33,34 (−.30 years; −.75 years, −.70 years respectively), similar to the values reported by De Souza et al.25 in Brazilians (.24 years) and Pinchi et al.6 in Italians (−.18 years) and higher than that verified in French subjects10 (−.14 years), Indians13,28 (−.09 years; −.15 years respectively), Serbians35 (−.16 years), Somalies16 (−.06 years) and South Africans8,37 (−.19 years, −.01 years respectively).
In both sexes it was found that in the younger age groups the precision of the methods was lower, which complies with that reported by Maber et al.1 and Nik-Hussein et al.2; for the intermediate age groups dental ages estimated were close to the CA of the subjects and above 16 years this was not applicable due to the fact that CA–DA differences were found to be greater than 12 months.
Regarding the WII21 method the study conducted by Hedge et al.30 reported an overestimation of age for the female sex (−.11 years) and an underestimation for the male sex (.06 years). The author reports that the method was more accurate in girls, in contrast to that observed in our study. However, the values were close and the differences were no greater than 10 months.
The differences found between the estimated DA and the CA of the study sample, compared with other populations, may be related to the difference genetic and environmental traits of each population, as well as the structure, size and selection of the sample, a non-standardized distribution in age groups, the research design, the nature of the sample by convenience and the unknown proportion of early, average or advanced maturing factors and the statistical approach employed.1,3,9,10,14,31 It is important to point out that simultaneous assessment of radiographs in this study could have systematized an over or under evaluation of the stages of maturation, with the judgement of one observer impacting the other.
With regard to the Venezuelan samples Medina and Blanco40 observed the overestimation of the age on applying WI20 in individuals coming from the metropolitan area of Caracas. In this sense the discrepancy in values found for the DA in a sample of the same country possibly reflect the impact of particular regional environmental, nutritional and cultural conditions on human development,7,40 and the proportionality factors of the different race mix built into the Venezuelan ethnicity.42 Future studies should consider expanding the sample and should take into account other maturation markers (bone age, height, weight, secondary sexual characteristics) which could add support to the estimation of forensic age.
ConclusionsIn this study the Willems et al.20,21 methods were compared in dental age estimation in a sample of Venezuelan origin. It was shown that WI20 and WII21 are applicable to the sample studied up to 16 years of age, but that precision varied in accordance with sex. Whilst WI20 demonstrated higher precision in the female sex WII21 was more accurate in the male sex. It is also important to point out that the diagnosis of forensic age has to be the result of DA evaluation combined with other markers such as bone age, height and weight, the presence of secondary sexual characteristics and the ruling out of diseases which could alter the course of development.
Conflict of interestThe authors have no conflict of interests to declare.
Please cite this article as: Ortega-Pertuz AI, Sil úPiña-D’Abreu M. Comparación de los métodos de Willems I y Willems II en la estimación forense de la edad en niños venezolanos. Rev Esp Med Legal. 2020;46:4–11.