Este estudio compara las diferencias de clima organizacional en los roles profesionales de hospitales públicos y privados. Nos hemos centrado en cómo los médicos, administrativos, personal sanitario y no sanitario, ya sea en público o en el privado perciben el entorno de trabajo, para cada dimensión clima organizacional. La información proviene de cuestionarios de clima aplicados en 2010 y 2012 para 19616 y 1276 empleados de salud en hospitales públicos y privados, respectivamente, de la Región Toscana. Se aplicó un análisis factorial exploratorio para verificar la validez y consistencia interna entre puntos del cuestionario y la prueba t, de un solo sentido el análisis de varianza para comparar significa percepciones respecto a las dimensiones a través de diferentes grupos de encuestados.
This study compares the organizational climate differences within professional roles in private and public hospitals. We focused on how physicians, administrative, healthcare and non-healthcare staff either in the public or in the private perceived their work environment and each organizational climate dimension. Data came from organizational-climate questionnaires administered in 2010 and 2012 to 19616 and 1276 health employees in public and private hospitals in the Tuscany Region respectively. We applied exploratory factoranalysis to verify the validity and internal consistency between items in the questionnaire and t-test, one-way analysis of variance to compare mean perceptions regarding to the dimensions across different groups of respondents. We measured four dimensions: “training opportunities”, “managerial tools”, “organization” and “management & leadership style” and overall job satisfaction. Hospital status in the professional roles was found significant in the staff's perceptions (p≤0.05).
It has been identified important elements for healthcare staff's commitment and loyalty toward the organization, examples of this elements are: continuing training and education (Spath, 2002), leadership style, project management, staff recognition, dedicated time, and resources for improvement projects (Thomson et al. 2003). But, organizational climate seems to depend also on the particular characteristics of the work environment (Tovey et al., 1999; Cumbey et al.,1998).
Organizational climate is defined as the shared perceptions of the work environment (Jones and James, 1979). This concept can be traced back to several studies, for example, Lewin et al. (1939) analyse the relationship between the leadership style and climate; Koffka (1935) focuses on “behaviour environment”; Lewin (1936) studies the “life space”; and Phillips (1996) investigated how women and men perceived the organizational climate. Some studies have shown the efforts made to better understand those factors which contribute to improve the work environment (or climate) and motivate all employees, regardless of their position, status and gender, to be committed and effective performers (Clark, 1997; Gershon, 2007; Nembhard, 2006)
In the present study we were able to analyze the hospital status (public or private) and professional roles with respect to organizational climate dimensions like training opportunities, managerial tools, organization and management & leadership style and job satisfaction inside twelve public general hospitals and eighteen accredited private hospitals. Our study included physicians, administrative staff, healthcare employees and non healthcare employees of the Tuscan healthcare system. There have been no recent studies of this phenomenon, and none have compared and contrasted organizational climate and professional roles at the hospital status. This paper is an attempt to address this gap in the literature.
The general hypotheses developed were whether public and private hospitals within professional role would differ significantly on how they perceived the organizational climate and job satisfaction. By studying a country like Italy with a particular health system we hope to give an insight to better understand the persistent barriers restricting the organizational climate in the professional roles at hospital status.
With regard to Italy, independently if public or private hospital is important the use of performance measurement to promote a more efficient and effective administration. With this premise, the Tuscany region with MeS laboratory in 2005 developed its own Performance Evaluation System valued as a particularly innovative and comprehensive system (Carinci 2011; Censis2008) it was implemented in order to follow up the regional objectives based on the needs of the Regional Health Councillor. The PES measured the quality of services provided and the ability to meet the needs of citizens in order to achieve better health and quality of life standards and to preserve financial stability. The 130 indicators are classified in six dimensions: Population health status; capacity to pursue regional strategies; clinical performance; patient satisfaction; organizationalclimate and finally efficiency and financial performance. (Nuti, 2011; Nuti, 2012).
Every year each public Health Authority receives its own report explaining if it was able to reach the objectives during the year and doing a benchmarking comparison. PES is compulsory for public institutions and optional-voluntary for private ones. In 2012 PES has been adopted by eighteen private hospitals as a decision support tool at managerial level. In 2012 was possible applied the organizational climate questionnaire to private institutions, getting interesting results to compare with the public context.
We reported a contribution on the debate of diversity in management of healthcare by highlighting the way in which staff perceived the organizational climate and the variation addressed in the professional roles and hospital status. The implications of this study can be useful to policy makers, managers and professionals understanding how the perception of the organizational climate fit aspredictor of good performance.
The contextThe Italian health care system is a National Health Service (Beveridge-like model) accessible to the full population providing preventive and curative services (Beveridge 1942). The system is organized at three levels: national, regional and local. The national level is responsible for ensuring the general objectives and fundamental principles of the National Health Service. The regional governments are responsible for ensuring the delivery of the health care through a network of population-based healthcare organizations (health authorities).
In Italy during the past two decades, the strong decentralization policy, in the line with “New-Public-Management” (NPM) philosophy (Kettl, 2000; Pollit, 1995) which aims is that public organizations should import managerial processes and behaviour from the private sector (Box, 1999; Boyne, 2002). With this argument the government have gradually transferred several important administrative and organizational responsibilities from the state to the 21 Italian regions with the aim of making regions more sensitive to the community needs, to control expenditure, promote efficiency, quality, and citizen satisfaction but specially it has started to focus on more effective management (Mouritsen et al., 2005).
This model provided regions with significant autonomy in organizing healthcare services, allocating financial resources to their Local Health Authorities (LHAs), monitoring and assessing performance (Nuti 2008, Antonini 2009). Whereas, the central government retains overall responsibility for ensuring that services, care and assistance are equitably distributed to citizens across the country.
The Tuscany region have 3.7 beds for each 1000 inhabitants of which 95% correspond to public beds and only 5% are privates. The healthcare system works through a network of seventeen public health authorities of which five are teaching hospitals (THs) and twelve are Local Health Authorities (LHAs) and eighteen private hospitals with accreditation.
In 1999, the Region of Tuscany began the accreditation system (LR 8/1999, LR 51/2009). Institutional accreditation is the recognition by the Region of hospitals that are authorized to provide and develop health services according to the National Health Service (NHS). Accreditation is compulsory for public institutions and optional-voluntary for private ones, but if private institutions does not have the accreditation cannot provide benefits on behalf of the NHS. However, obtain accreditation, does not allow to perform services on behalf of the NHS, is compulsory an agreement between subject and accredited Local Health Authorities that specific times, costs, terms and amounts of benefits payable in agreement with the NHS (Lenzi, 2012).
Data and MethodsIn 2010 the Laboratory of Management e Sanità (MeS) with Tuscany region administered the organizational climate survey to health care professionals in 16 Tuscan Health Authorities (12 General Hospitals1 and 4 Teaching Hospitals), with a total population of 2407 managers and 47903 staff. In 2012 the survey was administered to healthcare professionals in 18 private hospitals with accreditation.
The organizational climate is part of the six dimension within Performance Evaluation System (PES). Regarding to the procedures for compiling and sending the survey; we provided the questionnaires on-line using the Computer Assisted Web Interviewing (CAWI) system; each employee had a login and password that allowed him/her access to the web platform for collecting data. Secure connection guaranteed the anonymity of responses and safety of data transmitted. (Pizzini and Furlan, 2011).
Independently from the questionnaire, all questions had a 5-point likert scale format, ranging from 1 extremely unsatisfied to 5 extremely satisfied. The analysis extracted information on the survey sample, job satisfaction and organizational climate dimensions like management & leadership style, managerial tools (i.e. budget), hospital organization and training opportunities. We tasted and validated both questionnaires and we assure the validity and reliability of the instrument.
We applied Factor Analysis to questionnaires to obtain the perception of managers and employees in terms of the dimensions mentioned above. We performed descriptive statistics, factor analysis, and two-tailed test to examine gender differences in the General hospitals. We used STATA software for statistical analyses (Version12, Stata Corp, College Station, TX).
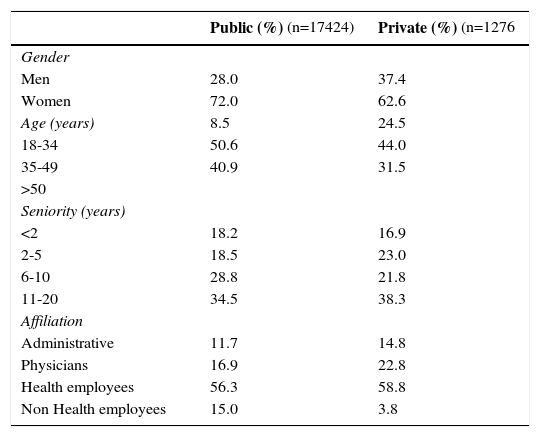
AnalysisRespondents’ characteristicsTable 1 shows descriptive statistic. In public hospitals 17424 of the 34686 staff (50.2%) returned the questionnaire while in private hospitals only 1276 employees returned it.
Descriptive statistics within hospital status.
| Public (%) (n=17424) | Private (%) (n=1276 | |
|---|---|---|
| Gender | ||
| Men | 28.0 | 37.4 |
| Women | 72.0 | 62.6 |
| Age (years) | 8.5 | 24.5 |
| 18-34 | 50.6 | 44.0 |
| 35-49 | 40.9 | 31.5 |
| >50 | ||
| Seniority (years) | ||
| <2 | 18.2 | 16.9 |
| 2-5 | 18.5 | 23.0 |
| 6-10 | 28.8 | 21.8 |
| 11-20 | 34.5 | 38.3 |
| Affiliation | ||
| Administrative | 11.7 | 14.8 |
| Physicians | 16.9 | 22.8 |
| Health employees | 56.3 | 58.8 |
| Non Health employees | 15.0 | 3.8 |
Applying factor analysis to the data we obtained overall job satisfaction and four organizational climate dimensions:
- 1.
Satisfaction with managerial tools was measure by four items (α=0.94). Testing the manager performance concerning to the budget responsibilities and control system.
- 2.
Satisfaction with training opportunities was measure by four items (α=0.86). Testing the correspondence between training needs of employees and hospitals’ structure, it means the effectiveness of the performed training and the diffusion of information related to educational opportunities offered by hospitals.
- 3.
Satisfaction with the organization was measure by seven items (α=0.89). Testing the hospital organization and structure.
- 4.
Satisfaction with management & leadership style by fifteen items (α=0.95). Testing the managerial abilities of the CEO, seniors and managers.
Overall job satisfaction dimension: Measure how content an individual is with his or her job.
Factors were obtained using Principal Components Factor Analysis, with varimax rotation of the orthogonal axes and in both cases the percentage of explained variance was about 65%. We calculated for each dimension Cronbach's α reliability coefficient above 0.8 confirming the validity and internal consistency between items on the scale of each factor.
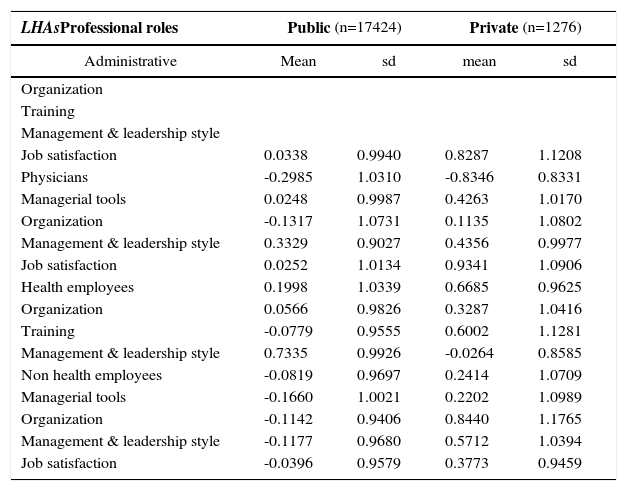
Professional roles in public and private hospitals in the perception of Organizational Climate FactorsSubsequently we used t-test to compare mean perceptions regarding to the dimensions obtained across different groups of respondents. The probability level for all hypothesis tests was set at p<=0.05.
Table 2 shows the significant dimensions of organizational climate in public and private hospitals analyzing professional roles. It was noted that the dimensions of organizational climate are important depending on the professional role; for example for the administrative staff is only significant the managerial tools and this is understandable because their priority is the budget. However, climate perception at hospital status reveals significant differences among physicians than the rest of employees.
Public vs. Private differences at professional roles of perceived climate and job satisfaction.
| LHAsProfessional roles | Public (n=17424) | Private (n=1276) | ||
|---|---|---|---|---|
| Administrative | Mean | sd | mean | sd |
| Organization | ||||
| Training | ||||
| Management & leadership style | ||||
| Job satisfaction | 0.0338 | 0.9940 | 0.8287 | 1.1208 |
| Physicians | -0.2985 | 1.0310 | -0.8346 | 0.8331 |
| Managerial tools | 0.0248 | 0.9987 | 0.4263 | 1.0170 |
| Organization | -0.1317 | 1.0731 | 0.1135 | 1.0802 |
| Management & leadership style | 0.3329 | 0.9027 | 0.4356 | 0.9977 |
| Job satisfaction | 0.0252 | 1.0134 | 0.9341 | 1.0906 |
| Health employees | 0.1998 | 1.0339 | 0.6685 | 0.9625 |
| Organization | 0.0566 | 0.9826 | 0.3287 | 1.0416 |
| Training | -0.0779 | 0.9555 | 0.6002 | 1.1281 |
| Management & leadership style | 0.7335 | 0.9926 | -0.0264 | 0.8585 |
| Non health employees | -0.0819 | 0.9697 | 0.2414 | 1.0709 |
| Managerial tools | -0.1660 | 1.0021 | 0.2202 | 1.0989 |
| Organization | -0.1142 | 0.9406 | 0.8440 | 1.1765 |
| Management & leadership style | -0.1177 | 0.9680 | 0.5712 | 1.0394 |
| Job satisfaction | -0.0396 | 0.9579 | 0.3773 | 0.9459 |
p>0.05
In general, staffs working in private hospitals are more likely than those working in public hospitals. Management & leadership style and organization are significant in all professional roles regardless of the hospital status, but private hospitals staff are more satisfy with both of them.
Satisfaction with the organization is the most significantly factor in private hospitals, but at the same time the most critical one because of the higher gap between two hospital status. Differences between public and private organizations have been discussed broadly. The first difference is that private organizations are owned by private partners while the nation is the owner of public organizations. Public sector organizations are controlled mainly by the political forces, not market forces. For this reason the main constraints are imposed by the political system, while in private organizations, the owners have a direct monetary incentive to motivate managers to provide better performance. Similarly, the managers themselves are likely to benefit from improved performance, because their payment is linked with the profit.
The literature pointed out that there are several external aspects that make different managing public organizations (Boyne, 2002; Arrow 1974; Angelopoulou, 1998; Bhatia, 2004). Public hospitals are complex organizations; Metcalfe (1993) argues that ‘government operates through networks of interdependent organizations rather than through independent organizations which simply pursue their own objectives’. Moreover, in the public sector there is more bureaucracy compared to the private one, also political conditions impacts the policy makers changing the short-term outlook and pressing to achieve results so fast, results that can help only for political purposes, whereas private organizations should pursue the goal of profit.
The results with respect to Managerial & leadership style are significant in all professional roles. Literature has shown that managerial & leadership style differ significantly between private and public organizations, managers in private organizations are motivated more by their economic well-being (Khojasteh, 1993) and public managers are more object-oriented and they have a desire to serve the public interest and strongly oriented towards the ‘common good’. Nevertheless, these results support some studies that have found that public sector employees are less satisfied with their work (Buchanan, 1974; Lachman, 1985).
Highly specialized staff responded more positively all items. Physicians and administrative employees were more positive about how they perceived their hospital, particularly the question about the adequacy of infrastructure and physical environment.
Training opportunities is significantly less effective in private hospitals. Moreover employees perceived that career opportunities are not equally guaranteed for all and there is a lack of information about training opportunities provided by the hospital. It seemed to be the most critical issue to be taken up.
We found the existence of a discreet difference in the perception of the managerial tools among physicians and a large difference among non health employees. The higher gap between professional roles concerned to the existence of a professional hierarchy in healthcare well established in the literature.
ConclusionsThe results of the present study support the hypothesis that there are differences in how the organizational climate is perceived by employees within professional roles and hospital status in the Tuscan healthcare organizations (General hospitals).
The analysis showed that the Tuscan organizational climate questionnaire is a reliable instrument used as a measurement tool for evaluating working conditions and determining the factors which satisfies and motivates employees in the healthcare sector. The four dimensions detected showed high variability and different significance along diverse organizational structures, professional roles and hospital status.
This study shows that there are major differences between public and private hospitals in terms of how they perceive the internal climate where the employees in private hospitals are more satisfied than employees in public ones. On the other hand, our results suggest that in terms of job satisfaction physicians in private institutions are in general more satisfied.
Training processes, however, within these organizations, are loosely coupled with the rest of the organizational processes and often depend on the employee's ability and willing to ask for targeted training courses.
Finally the use of an organizational climate survey can help management to identify the critical points in the factor dimensions and communicate more effectively within the structures improving the effectiveness of total quality management programmes.
In fact, a valid internal climate survey can be a useful tool in supporting the management to make effective innovation process. Moreover, in order to assure its effectiveness it is important to share and discuss the results of the internal climate survey with all the professionals being this the most important prerequisite to support the organizational changes and it is what the Tuscan health managers are used to do not only with regards to the internal climate results but also to all the performance measures.