
Psychophysiological arousal was observed in cancer patients during the application of relaxation techniques prior to a diagnostic scan (PET-CT). The aim of the study is twofold: firstly, it is sought to establish whether such techniques can minimize patient arousal before diagnostic screening begins, and secondly to measure which of them are most effective. The dependent variable is electrodermal activity, recording the attentional level and emotional response, and the independent variable comprises the relaxation techniques used, namely Jacobson, breathing and visualization. The 39 patients were split into experimental groups to whom the relaxation techniques (Jacobson, breathing exercises, and visualization) were applied before they went for the PET-CT. An activity-module procedure was applied to track electrodermal activity during the relaxation sessions, consisting of instructions, timeout; wait, task; relaxation and end of the recording session. The control group received no relaxation techniques before the PET-CT. Session-end results show that patients who perform relaxation techniques achieve greater attentional focus using Jacobson's technique (M=.212) and enhanced emotional containment using visualization (M=.206). It is concluded that relaxation techniques minimize the state of activation during the waiting period before a diagnostic scan.
Se registra la activación psicofisiológica en pacientes oncológicos durante la aplicación de técnicas de relajación antes de someterse a una prueba diagnóstica (TEP-TAC). Se plantea un doble objetivo: primero, comprobar si dichas técnicas minimizan el estado de activación de los pacientes antes de realizar pruebas diagnósticas, y en segundo lugar, medir cuáles de estas son más efectivas para relajarse. La variable dependiente es la actividad electrodérmica, registrando el nivel atencional y la respuesta emocional, y la variable independiente son las técnicas de relajación de Jacobson, de respiración y de visualización. Se distribuyen los pacientes (n=39) en 3 grupos experimentales y se les aplican las técnicas antes de realizar el TEP-TAC: Jacobson, respiración y visualización. Se utiliza un procedimiento para el registro de la actividad electrodérmica durante la relajación por módulos de actividad: instrucciones, tiempo muerto; espera, tarea; relajación, y fin del registro. El grupo control no recibe relajación antes del TEP-TAC. Los resultados indican que los pacientes que realizan relajación consiguen mayor focalización atencional con Jacobson (M=.212) y mayor contención emocional con la visualización (M=.206). Se concluye que las técnicas de relajación minimizan el estado de activación durante el periodo de espera antes de una prueba diagnóstica.
Cancer patients’ psychophysiological arousal levels were measured while they were exposed to relaxation techniques before undergoing diagnostic screening (PET-CT scan), using electrodermal activity (EDA) as a somatic indicator (Bechara, Damasio, Tranel, & Damasio, 2005; Meshulam, Winter, Ben-Shakhar, & Aharon, 2011). Relatively few studies have specifically addressed the association between anxiety and diagnostic neuroimaging procedures. However, the existing studies indicate a tendency on the part of cancer patients to display a state of considerable anxiety before the scan begins (Doménech et al., 2010; Pifarré et al., 2011). Anxiety was measured in existing studies using the State Trait Anxiety Inventory (STAI) but EDA (psychophysiological arousal) has not so far been measured before a neuroimaging procedure.
Numerous different clinical procedures carried out in the healthcare context raise reactive anxiety levels, and diagnostic cancer screening is generally considered a stressful life context for both patients and their families (Nápoles, Agüero, Díaz, & Espinoso, 2013; Pifarré et al., 2011). Relaxation techniques provide a therapeutic resource to reduce stress and achieve a state of composure which helps optimize biopsychosocial exploration of patients, especially in the case of diagnostic tests requiring significant exposure times (González, 2012).
The aim of this study is to establish the extent to which relaxation techniques actually minimize cancer patients’ states of psychophysiological arousal before they undergo diagnostic screening, and which are the most effective methods in this therapeutic context.
Electrodermal activityElectrodermal activity (EDA) has a strong track record as a psychophysiological measure in the field of psychology (Cacioppo, Tassinary, & Berntson, 2007), and it is also widely used in the social sciences in view of its sensitivity, reliability and ease of application (Smith & Ruíz, 2002). EDA is conceptualized in experimental research as a somatic marker (Bechara et al., 2005) to explain both individual and social behaviors (Aiger, Palacín, & Cornejo, 2013; Lajante, Drolers, Dondaine, & Amarantini, 2012).
Electrodermal activity provides an optimal measure of the autonomic nervous system, and it is one of the most widely used indices as a physio-psychological correlate given its association with emotion, arousal and attention. Variations in EDA may be understood as evidence of changes in a subject's state of attention and/or emotions (Smith & Ruíz, 2002). Activity is controlled basically via the sympathetic nervous system, which handles arousal processes and is free of parasympathetic interferences.
Stress and anxietyThis study uses the concepts of stress and anxiety – as applied in the field of Health Psychology – as reactive indices for biopsychosocial stressors. From the standpoint of Psychophysiology, the conceptualization of stress as a reaction or response pattern is linked to the condition referred to as anxiety in other disciplines (Knudsen, Berge, Skogen, Veddegjærde, & Wilhelmsen, 2015; Perpiñá, 2012).
However, stress and anxiety are read differently in the field of psychology. As a pathological process, stress refers to distress, while anxiety is a disorder that takes a variety of clinical forms (Regier, Narrow, Kuhl, & Kupfer, 2012). Studies have shown that around half of the patients diagnosed with cancer present with psychological disorders, most commonly anxiety and depression (Gil et al., 2008). This emotional deterioration can compromise cancer patients’ determination to press on with treatment, or even to go on living (Alvarado et al., 2011).
The concept of stress can be viewed in a variety of different ways. Viewed as a stimulus, stress implies a significant change in conduct (Sierra, Ortega, & Zebeidat, 2003). As a response, however, stress is more closely linked to health and is conceptualized as the organism's general response to a stressor triggering a given pattern of physiological reactions (Spector et al., 2015). A third conceptualization treats stress as an interaction between the organism and its environment (Lazarus & Folkman, 1986). In this view, the emphasis lies on the subjective assessment of stressful events rather than the actual experience of such events. Hence, stress is understood as a process of (cognitive-emotional) evaluation, which activates personal resources for action. This approach ties in with the social conceptualization of stress, in which external conditions may generate stress and thereby impinge on health, quality of life and longevity (Pulgar, Alcalá, & Reyes del paso, 2015; Sandín, 2003). Hospital visits and the subjective experience of undergoing diagnostic screening (PET-CT) could be conceptualized as social stresses of this kind. Such situations can generate states of arousal insofar as they involve: (a) unfamiliar medical procedures, (b) feelings of defenselessness, and (c) the possibility of a positive or negative diagnosis, but they always imply expectations of bad news in the form of diagnostic confirmation of a malignant tumor. These expectations affect the processes of psychophysiological arousal picked up by EDA (Aiger et al., 2013).
Anxiety is a universal experience which causes a psychophysiological, behavioral and cognitive response characterized by a state of arousal or alert (Perpiñá, 2012; Sierra et al., 2003). In this light, it is necessary to recognize states of pathological anxiety emerging as a non-adaptive response based on the intensity, duration and frequency of symptoms affecting the individual's personal, social and professional sphere.
Relaxation techniquesRelaxation techniques offer an important preventive and therapeutic alternative, generating an optimum response in terms of psychophysiological and emotional stability in the face of reactive anxiety caused by the forthcoming diagnosis of the patient's condition (Blanco et al., 2014).
Relaxation techniques originate from the meditational practices developed by eastern religions over 5000 years ago. In the Western culture, these techniques have been employed as a means of control of psychophysiological and emotional arousal. Their use was pioneered in the field of mental health by Jacobson, who published his seminal “Progressive Relaxation” in 1929, and Schultz, whose book “Das Autogene Training” appeared in 1932. In turn, the use of relaxation techniques in clinical psychology is associated with Behaviorism (behavior modification) and the work of Wolpe (1958). His contribution is recognized in view of its implications for (a) the prevention and protection of the bodily organs against unnecessary deterioration (caused by stress-related disorders), (b) the treatment of stress in psychophysiological problems like idiopathic hypertension, tension headaches, insomnia, asthma, immune deficiencies, anxiety and other conditions addressed in the field of health psychology, and (c) a psychotherapeutic approach to positive cognitions.
Relaxation techniques influence improvements in health through physical and psychophysiological changes in the muscular, respiratory, cardiovascular, central and autonomic nervous, endocrine and immune systems (Soriano, 2012).
The following relaxation techniques were applied: (a) Jacobson's progressive relaxation, which is grounded on the existence of a direct relationship between the muscular system and the nervous system. Hence, the logic of the program is based on learning to identify tension/relaxation in the different parts of the body. A detailed, progressive path is followed to identify the different parts of the body and focus attention on each. In a final phase, the knowledge gleaned in this way is generalized to address any activity in daily life which results in the perception of tension (Payne, 2005). Some authors have criticized this method as being too time-consuming and complex for clinical use, and because of its self-training aspects (Vázquez, 2001). Wolpe himself addressed these criticisms and made some changes to the program. One of the most relevant changes was the inclusion of the role of the therapist to conduct training and provide verbal instructions in all sessions. This function does indeed succeed in reducing training time (Vázquez, 2001). Evidence exists to suggest that this type of relaxation technique is effective in cancer patients, reducing the intensity and duration of nausea and vomiting after chemotherapy (Molassiotis, Yung, Yam, Chan, & Mok, 2002), (b) the breathing technique is based on breath control to achieve a pattern of slow, regular inhalation and exhalation. Therapeutic processes usually employ deep breathing techniques to achieve changes in the organism depending on individual needs. The processes involved are inhalation – using the diaphragm to oxygenate the body and activate the vagus nerve – with effects at the parasympathetic level, and exhalation to expel the maximum volume of CO2. Constancy and concentration in the practice of this technique result in a general lowering of the body's state of arousal. The objective is to acquire voluntary breath control under optimum conditions, allowing spontaneous activity of the process in situations of stress, (c) visualization is defined by Achterberg as “the thought process invoked and used by the senses” (Payne, 2005, p. 225). This activity can involve all five senses in the absence of any external stimuli.
The therapeutic effect of visualization is to focus attention on multisensorial scenarios created and experienced by the subject. The effects described include psychological changes which encourage relaxation and diminish negative thoughts at times of stress. Thus, the technique helps reduce anxiety and stress (Payne, 2005).
Psychophysiological aspects of cancer patientsCancer is one of the leading health problems in western countries. Pifarré et al. (2011) found in their study that the number of people diagnosed with cancer will increase in the coming years, in part as a result of population aging. In light of the above, cancer is a most pressing health issue which warrants an approach from a range of medical and psychosocial standpoints.
As early as 1948, the World Health Organization (WHO) called for health to be conceptualized and defined as a complete state of physical, mental and social wellbeing, and not merely the absence of biomedical complaints. One of the most salient definitions of health was proposed by Milton Terris in 1980, who stressed the adaptive and functional components that are key to the development of oncological processes (Toro & Ochoa, 2012).
Health professionals need to base their work on a holistic and comprehensive conceptualization of the patent throughout the therapeutic process, whether in diagnosis, treatment, rehabilitation or palliative care. An approach based on Social Health Psychology (Rodríguez-Marín & Neipp, 2008) implies the application of biopsychosocial methods by the triadic patient–family–professional intervention unit to further the process of adaptation to the disease (Pemberton & Wainwright, 2014; Pozo, Bretones, Martos, Alonso, & Cid, 2015).
Healthcare cannot be separated from perceived social support, which has a significant influence on improving quality of life (Norman et al., 2012; Villarroel, 2009) and on the process of adaptation to cancer from the moment of its diagnosis (Sánchez, Montes, Romera, & Álvarez, 2014).
Twenty to forty percentage of cancer patients display psychiatric comorbidity involving emotional disorders which require psychiatric and/or psychological intervention. The important psychological dimension of cancer is noteworthy, thereby stressing the need for multidisciplinary teams of cancer specialists to provide support and meet the emotional needs of oncology patients (Söllner et al., 2001). It refers to the need to strengthen doctor–patient help relations in the communication of bad news, and lasting throughout the course of the illness. A key element of this relationship is to keep the patient abreast of developments in order to minimize uncertainty and reduce anxiety. According to Pifarré et al. (2011), ca. 67% of cancer patients taking a PET-CT scan suffered some anxiety. These figures underscore the importance of protecting the patients’ mental health, reflecting the need for psychological intervention at an early stage in the diagnostic process to minimize stress caused by failing health. This emotional deterioration can compromise cancer patients’ commitment to their treatment and even will to live. Once cancer has been diagnosed, a patient has to face up to a raft of structural, functional and emotional situations brought on by biopsychosocial changes requiring temporary and permanent adjustments to life plans and life cycle in a process that demands careful management and support where necessary (Palacín & Aiger, 2011; Rico, Ristreto, & Molina, 2005).
MethodParticipantsThe sample consisted of 39 adult subjects aged 20–82 years (M=50.48; SD=17.19), of whom 48.71% were men (M=52.42 and SD=16.98) 51.28% were women (M=48.65 and SD=17.67). The subjects were selected randomly from among patients requiring PET-CT diagnostic cancer tests, whose names were provided by the Nuclear Medicine Department at Vall d’Hebron Hospital in Barcelona. Over half of them (60%) displayed a state of anxiety (SA) without having any prior history of anxiety or of earlier psychological interventions. Meanwhile, 76.93% were taking medication (20% psychiatric drugs to treat symptoms of anxiety and depression; 36.6% painkillers; and 30% anti-inflammatory medicines). No instruments were included in the study to measure anxiety as a dependent variable, as this was not the purpose of the exercise, but it was considered as a descriptive variable which was indicative of the subjects’ state via their clinical records.
MeasuresEDA was recorded using Sociograph psychophysiological instrumentation (Aiger et al., 2013) and measured in terms of skin resistance. The unit of measurement was kilohms (kΩ) employing the constant current method. A cadence of 20 signals per second was used. The amplification range was 500kΩ in channel 1 (EDL) and 10kΩ in channel 2 – EDR – (Aiger et al., 2013). Both components of EDA were recorded: (a) the electrodermal level (EDL) describes tonic activity related with attention processes, and (b) the electrodermal response (EDR) measures phasic activity defined as the orientation reflex (OR) related with emotional responses. Accordingly, the EDA data reflect the attentional and emotional arousal levels of subjects to whom the different relaxation techniques were applied (muscular relaxation, breathing and visualization).
Recording EDA in terms of skin resistance has implications for the interpretation of the results obtained. A drop in resistance in EDL values implies a focalization of attention, while an increase is associated with a loss of concentration. In the EDR results, meanwhile, only the amplitude of the signal associated with greater or lesser emotional reactivity in the presence of a stimulus is considered.
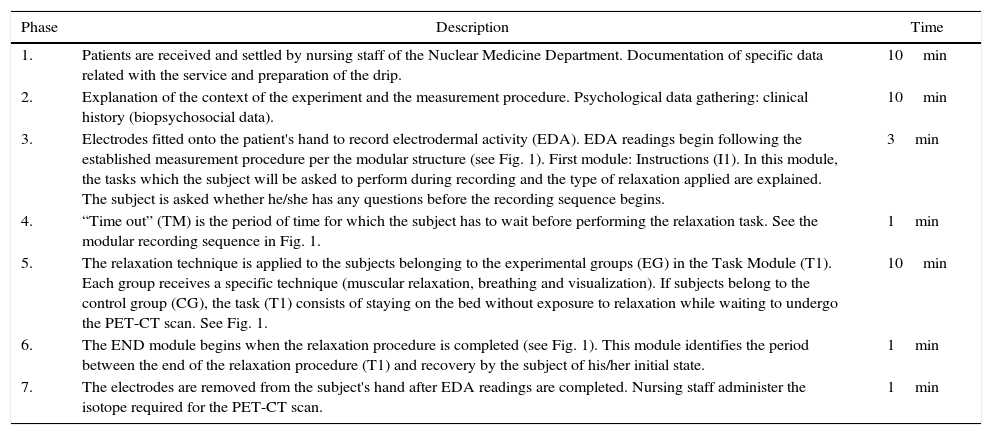
ProcedureA protocol (see Table 1) was established to standardize the measurement procedure over a period of 36min from the moment the patient is received until the start of the diagnostic PET-CT scan. Such research meets the approval of the Ethics Committee of the health institution and signed informed consent.
Experimental protocol.
| Phase | Description | Time |
|---|---|---|
| 1. | Patients are received and settled by nursing staff of the Nuclear Medicine Department. Documentation of specific data related with the service and preparation of the drip. | 10min |
| 2. | Explanation of the context of the experiment and the measurement procedure. Psychological data gathering: clinical history (biopsychosocial data). | 10min |
| 3. | Electrodes fitted onto the patient's hand to record electrodermal activity (EDA). EDA readings begin following the established measurement procedure per the modular structure (see Fig. 1). First module: Instructions (I1). In this module, the tasks which the subject will be asked to perform during recording and the type of relaxation applied are explained. The subject is asked whether he/she has any questions before the recording sequence begins. | 3min |
| 4. | “Time out” (TM) is the period of time for which the subject has to wait before performing the relaxation task. See the modular recording sequence in Fig. 1. | 1min |
| 5. | The relaxation technique is applied to the subjects belonging to the experimental groups (EG) in the Task Module (T1). Each group receives a specific technique (muscular relaxation, breathing and visualization). If subjects belong to the control group (CG), the task (T1) consists of staying on the bed without exposure to relaxation while waiting to undergo the PET-CT scan. See Fig. 1. | 10min |
| 6. | The END module begins when the relaxation procedure is completed (see Fig. 1). This module identifies the period between the end of the relaxation procedure (T1) and recovery by the subject of his/her initial state. | 1min |
| 7. | The electrodes are removed from the subject's hand after EDA readings are completed. Nursing staff administer the isotope required for the PET-CT scan. | 1min |
Note: Subjects were informed about the type of relaxation technique and provided with instructions in the third phase of the procedure, performing the task (T1) assisted by nursing staff in the fifth phase. See Appendix 1 for a description of the visualization technique and the protocol employed in the respiration technique. Exercise 2 (pp. 207) and Jacobson (pp. 213–215) were conducted following the protocol outlined in Tables 7–21 (Labrador, 2008).
EDA was measured as a continuous signal over time, applying a methodology structured in activity modules (Aiger et al., 2013). The modular structure of the measurement procedure is shown in Table 2. This approach implies assigning one module to each activity in order to control for signal activation levels in the different stimulus contexts from the start through to the end of the measurement process.
Experimental designThe general objective was to measure the extent to which the different relaxation techniques reduced cancer patients’ states of reactive anxiety before undergoing diagnostic screening (PET-CT). Meanwhile, specific aims consisted of (a) seeking differences in arousal levels between subjects who received relaxation techniques and those who did not before the PET-CT scan, and (b) observing what type of relaxation (muscular, breathing or visualization) did the most to reduce levels of arousal (higher focus of attention and lower emotional reactivity) before the start of the diagnostic PET-CT scan.
The dependent variable consists of the electrodermal activity (EDA) recorded, reflecting attentional and emotional arousal as a somatic psychophysiological marker. The signal obtained was processed to extract the tonic signal (EDL) and the phasic signal (EDR). Meanwhile, the independent variable consisted of the three types of relaxation technique, namely: (a) muscular relaxation (Jacobson), (b) breathing and (c) visualization.
The initial working hypothesis was that subjects performing relaxation techniques (experimental group) before undergoing the PET-CT scan would display lower levels of emotional response (EDR) and enhanced attention focus (EDL) compared to the control group subjects, who were not exposed to relaxation techniques before the PET-CT procedure.
A repeated measures design was used. The sample (N=39 subjects) was distributed into four groups consisting of (a) a control group (CG) with nine subjects, to whom no relaxation techniques of any kind were applied, and (b) three experimental groups (EG), who were exposed to relaxation techniques before undergoing the diagnostic PET-CT scan as follows: (1) EG1, application of Jacobson's muscular relaxation technique to 10 subjects; (2) EG2, application of the breathing technique to 10 subjects; and (3) EG3, application of the visualization technique to 10 subjects.
Statistical analysesEDA was recorded in kilohms and transformed to Z scores with mean 0 and a standard deviation of 1. These standard measures allow comparison of oscillations in the signal (EDL–EDR) via overall scores (mean and standard deviation) applying the Analysis of Variance or ANOVA parametric statistical test (Lajante et al., 2012) to the modular sequence recorded (see Fig. 1). A total of 902624 readings were obtained with a cadence of 20 readings per second.
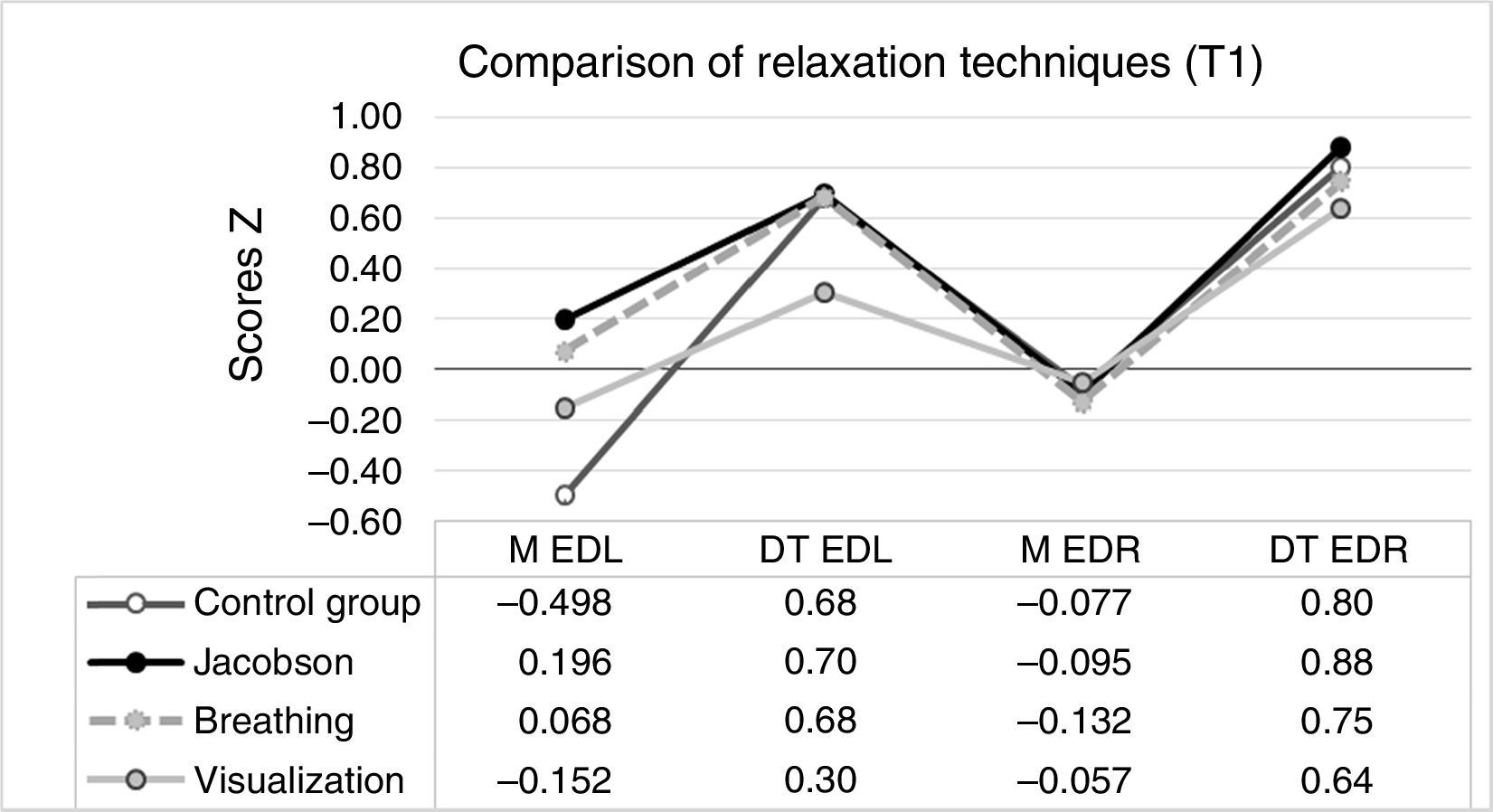
 and phasic (EDR) signal of relaxation techniques. Note: The subjects performed the task in the T1 activity module. In the experimental group, the task consisted of relaxation using one of the three techniques (Jacobson")
Scores. Mean and standard deviation of the tonic (EDL) and phasic (EDR) signal of relaxation techniques. Note: The subjects performed the task in the T1 activity module. In the experimental group, the task consisted of relaxation using one of the three techniques (Jacobson's progressive muscular relaxation, breathing and visualization). There was no relaxation in T1 in the control group. The readings taken under the different experimental conditions during T1 were as follows: control group (72.681), Jacobson's muscular relaxation (83.100), breathing (70.783) and visualization (69.059).
Fig. 1 presents the data for the experimental group (EG) subjects exposed to the different relaxation techniques (EG1; Jacobson muscular relaxation, EG2; breathing and EG3; visualization) in activity Module T1 compared to the control group (CG) subjects, to whom no relaxation techniques were applied before diagnostic screening. The results obtained indicate significant differences between the relaxation techniques in Module T1 (EG) in terms of oscillatory trends in EDA (VD) both for EDL F(3, 5595.619)=4497.17, p<.01 and for EDR F (3, 295.619)=117.36, p<.01. The mean scores and standard deviations in EDA are shown in Fig. 1.
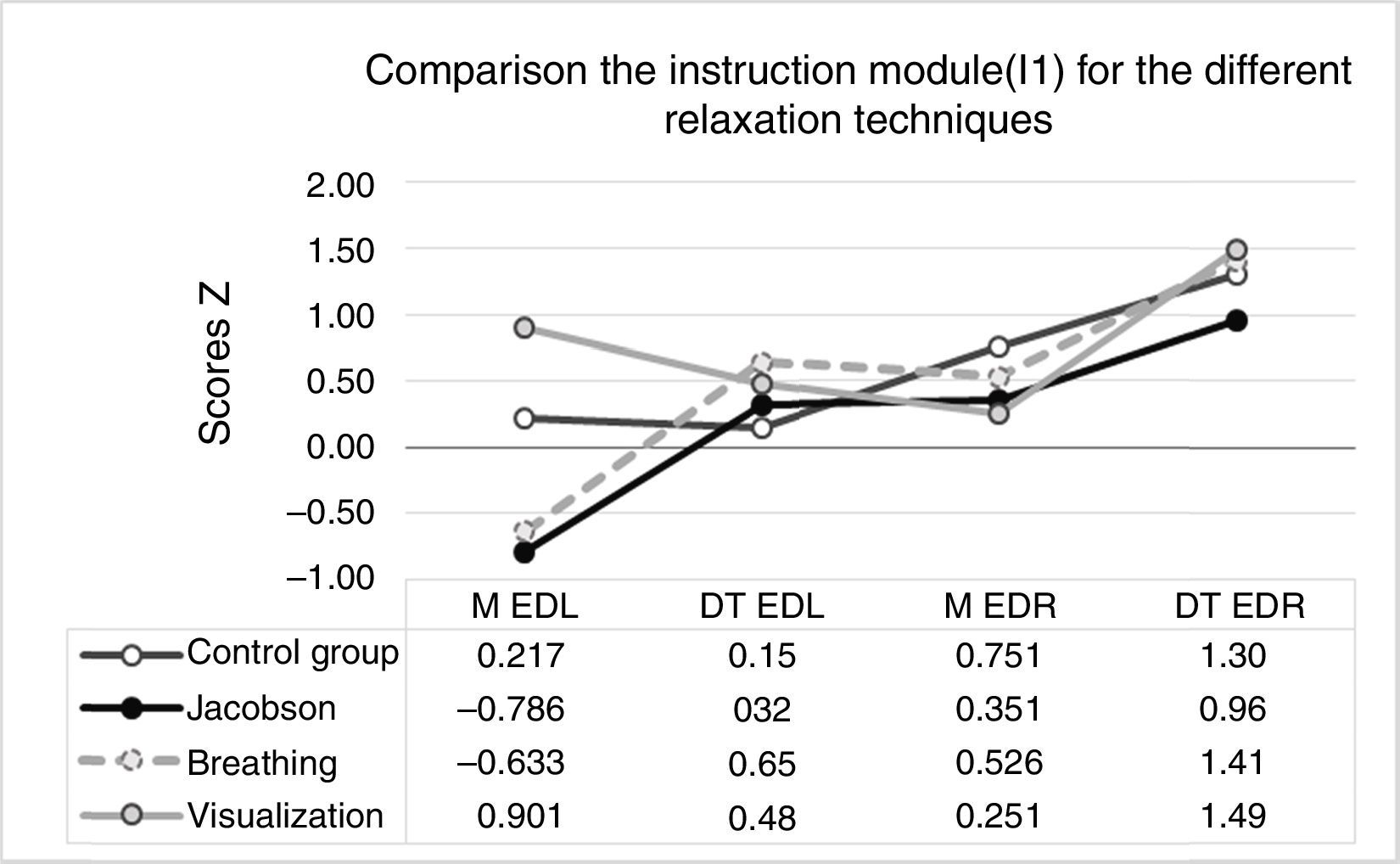
There are significant differences between mean EDA in the Instructions Module (I1) in the four experimental situations (Jacobson, breathing, visualization and control group). EDL displays a value of F(3, 42407)=31463.14 and EDR a value of F(3, 32147)=261.62, both with a significance level of p<.01. The mean scores are shown in Fig. 2.
 and phasic (EDR) signal during the instruction phase (I1).")
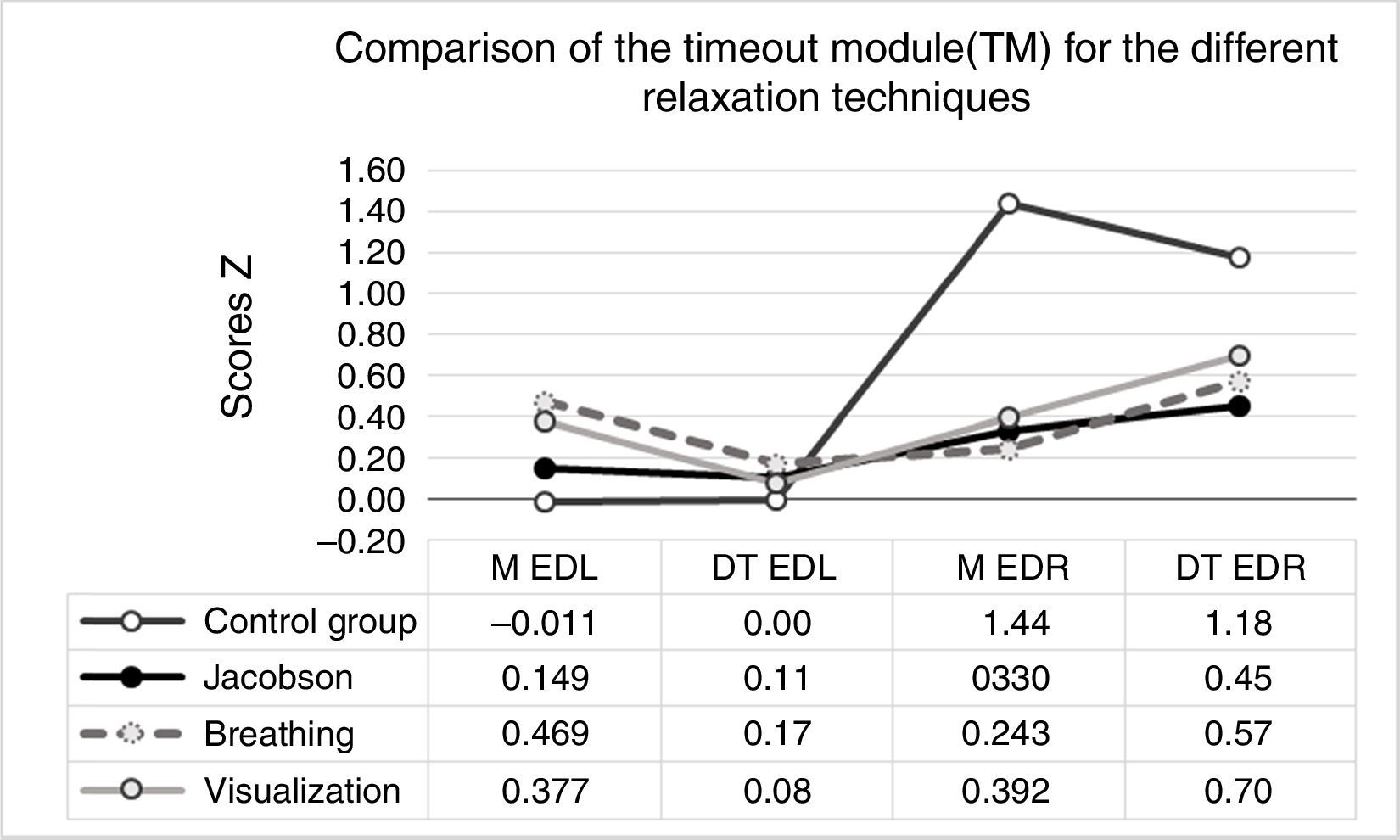
The modular sequence (see Table 2) continues with the presentation of the total mean scores and standard deviation for EDA in the “Time out” Module – TM – (see Fig. 3). Significant differences were also found in this case between mean values both for EDL F(3, 22516)=10357.95 and EDR F(3, 22516)=952.38 with a significance level of p<.01.
 and phasic (EDR) signal during the Timeout Module (TM).")
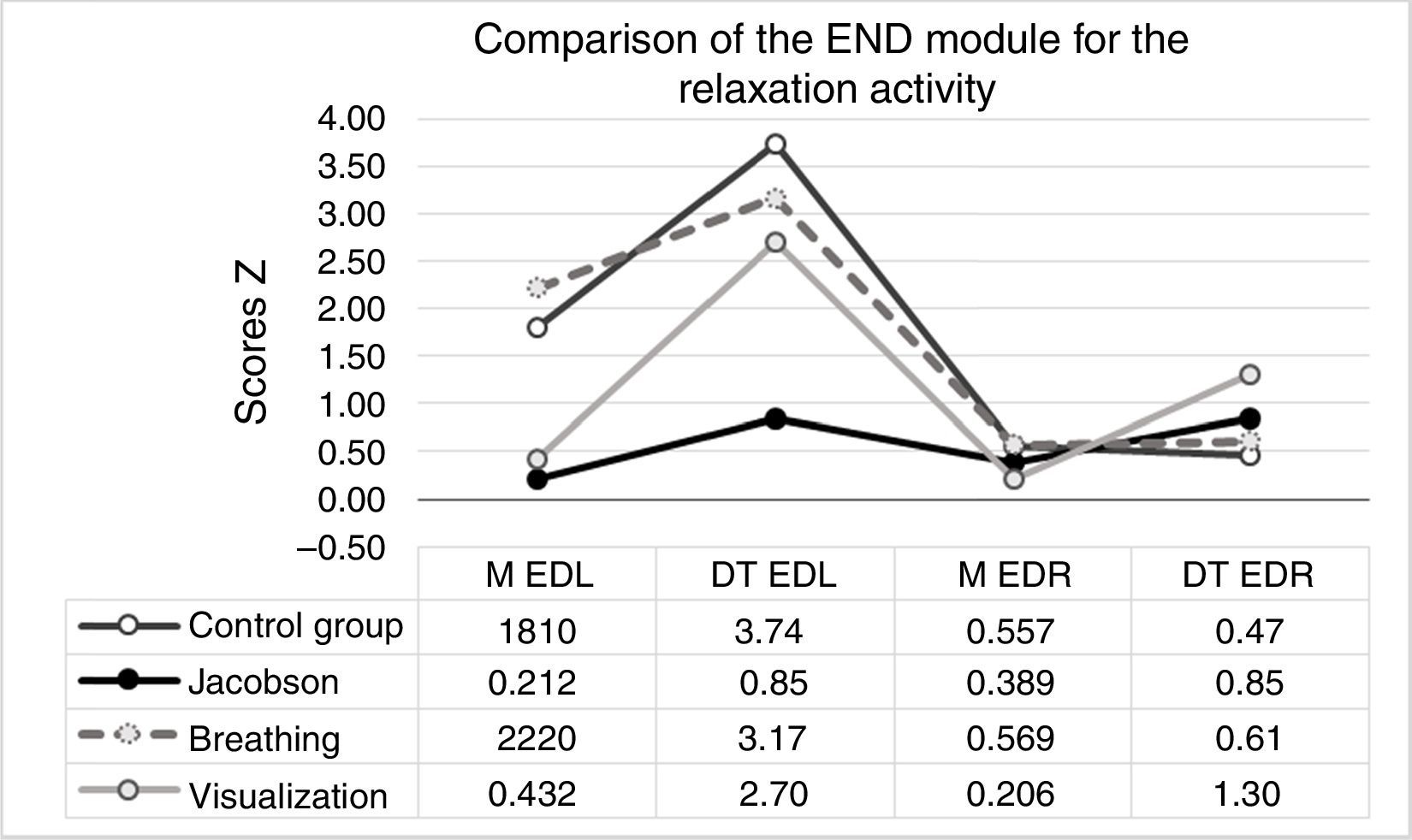
END, the last module of the recording sequence (see Table 2), is shown in Fig. 4, reflecting overall scores for EDA (mean and standard deviation). Significant differences in results were found in the distribution of arousal for both EDL (F(3, 23068)=981.94; p<.01) and EDR (F(3, 23068)=156.18; p<.01).
Discussion and phasic (EDR) signal during the end module of the relaxation activity (FIN).")
The type of relaxation which achieves the greatest focalization of attention (EDL) and the smallest oscillation in emotional response during application (T1) is the visualization technique. Subjects are most concentrated in this technique and their emotional responses are more contained than in the other two forms of relaxation (Jacobson and breathing). In view of the similarity of effects between subjects, visualization appears as the most consistent technique in terms of both attentional and emotional arousal. The results indicate that the least effective technique is Jacobson's muscular relaxation, in which subjects experience most difficultly focusing attention, while its effects are the most variable during application. However, these findings change when the recording sequence module observed is END (see Table 2). Comparing the different relaxation techniques in this module, the subjects exposed to Jacobson's muscular relaxation achieved the highest level of attentional focus (EDL), although it was not evenly spread among them all, and the lowest levels of emotional reactivity (EDR) together with the visualization technique. Nonetheless, in this case the results were more dispersed (see Fig. 4). In light of the foregoing, we may conclude that the two most effective relaxation techniques are visualization and Jacobson's muscular relaxation depending on timing. The former produces a quicker relaxation effect, whilst the latter takes somewhat longer to help the subjects concentrate at similar levels of emotional response. Meanwhile, the effect of visualization is more evenly spread. Time-related effectiveness has already been mentioned in critiques of Jacobson's progressive relaxation method as modified by Wolpe (Vázquez, 2001) to include a therapist to direct the process.
The breathing technique does not achieve appreciable effects either on attentional focus or emotional containment in patients compared to Jacobson relaxation and visualization (see Fig. 1). In fact, it only has any effect during the instruction period (see Fig. 2). This is because it is the only one of the three in which the patient is asked to rehearse the technique during the explanation of the relaxation procedure in order to ensure that the breathe in/out instructions are well understood. Therefore, it is a good technique to focus subjects’ attention quickly.
Applying relaxation techniques (T1) helps patients to focus their attention (EDL) but it does not have a significant influence on emotional containment. In fact, the only significant difference was found in the “Time out” module of the sequence (see Table 2). The subjects exposed to relaxation (EG) displayed a more contained emotional response during the wait prior to the application of the technique than did those who did not perform the procedure. Expectation in relation to the task (T1; perform relaxation) in the experimental group helped them contain their emotional response, and this effect was more evenly spread among the group than the emotional responses of the subjects who were not exposed to any relaxation – CG – (see Fig. 3).
Previous studies suggest that cancer patients attending a diagnostic PET-CT screening tend to be anxious (Doménech et al., 2010; Pifarré et al., 2011). In this study, the difference between applying or not applying relaxation techniques is evidenced in the emotional responses of patients who are told that they will perform relaxation techniques before undergoing the PET-CT procedure (“Time out” module of the sequence, see Table 2 and Fig. 3). These patients display lower levels of emotional reactivity while they are waiting to begin the relaxation procedure (time out) than those waiting without any exposure to relaxation before the diagnostic scan. In this light, we recommend that patients should play an active role in the diagnostic process, so as to focus their attention on a particular task. Focusing attention through the use of relaxation techniques helps generate a state of emotional containment which was not found among the control group patients – the latter were asked to wait without relaxation. This approach fits well with Milton's definition of health, in that it underscores the necessarily adaptive and functional role of cancer patients during the therapeutic process (Toro & Ochoa, 2012). Finally, it is preferable – in short waiting periods – to apply a technique with more immediate effects like visualization than a more elaborate technique like muscular relaxation, which requires more time to take effect. This technique may be more suitable for use in the periods associated with treatment (chemo- and radiotherapy). In fact, Jacobson's technique does not begin to have an effect after about half an hour of progressive muscular relaxation.
Thanks are due to the Nuclear Medicine Department of Vall d’Hebrón Hospital in Barcelona for their kind assistance with this study. We are especially grateful to Dr. Simon for his advice and attentiveness, to Dr Pifarré for her suggestions regarding the measurement methodology, and to the nursing team for their work in recording data at the same time as carrying out their ordinary tasks. Finally, we would like to thank Rosalía Irvernom and Sara Fernández for their daily assistance in the experimental phase of the study.
Patients are requested to close their eyes and concentrate on the points of contact between different parts of their bodies and the bed. The subject is guided from the back of the head downwards to the shoulders, arms, back and hips, and is then asked to focus on the weight of their legs on the surface of the bed and, finally, to the position of their feet. The subject is then instructed to visualize a path leading to a beach, and to try to perceive sights and sounds as clearly as possible, while feeling the different sensations on their skin. We begin the walk. It is a sunny day, and you have decided to take a stroll on the beach. You gradually put the noise and stresses of daily life behind you, eventually coming to the beach path. It is a warm day, and the sun pleasantly bathes your skin. A soothing breeze starts up, gently cooling your face. From the path you survey the horizon where the deep blue of the sea meets the lighter blue of the sky. There are no clouds and the sea is calm. You decide to go down onto the beach, your feet sinking into the warm sand. You sit and watch the waves break on the shore, feeling refreshing drops of cold water splash onto your feet. You lie back in the inviting sand, focusing on the grainy warmth on your back. For a few seconds you concentrate on the sound of the waves and the silence around about. There is nobody else on the beach. At last it is time to go home, so you get up and take one last look at the sea. Before you open your eyes and stand up, I am going to count to three: (1) slowly move your feet and legs; (2) now your arms and torso; and (3) your neck and head. Open you eyes and get up slowly.