


Most Spanish prisons provide specialised treatment for incarcerated sex offenders, both rapists and child molesters. This treatment is a cognitive-behavioural intervention that has shown relative effectiveness in previous research. With regard to offenders’ rehabilitation, recidivism assessments are necessary as a final measure of treatment effectiveness. However, the evaluation of recidivism by itself does not provide sufficient information on the treatment process and the specific effects that treated subjects could undergo. This paper aims to analyse the therapeutic effectiveness of psychological treatment provided to rapists (in general, males sentenced for committing a sexual offence against women). To this aim, a group of treated rapists (N=153) serving a sentence in prison was analysed. Using a specially designed scale (PASSO), the global therapeutic change and ten specific variables (including assertiveness, readiness to change, cognitive distortions, impulsivity, etc.) were assessed. The within-subjects comparison showed that treated sex offenders improved, in therapeutic terms, globally as well as in most of the specific variables assessed (improvements not experimented by the control group). Also, different therapeutic subscales showed relevant associations between them. The findings regarding treatment effectiveness are discussed.
La mayoría de los centros penitenciarios españoles ofrecen un programa de tratamiento psicológico especializado para agresores sexuales, tanto para violadores como para abusadores de menores. Se trata de un programa de orientación cognitivo-conductual, que en algunas evaluaciones ya realizadas ha evidenciado una eficacia terapéutica relativa en términos de reducción de las tasas de reincidencia. Aunque la evaluación de la reincidencia delictiva sea una medida necesaria para ponderar la eficacia final del tratamiento de los agresores sexuales, dicha medida no permite conocer con precisión las mejoras específicas que los sujetos pueden experimentar. Este artículo dirige su atención precisamente a evaluar con detalle la eficacia terapéutica del tratamiento de los agresores sexuales de mujeres adultas. Con esta finalidad, se analiza una muestra de agresores sexuales tratados (N=153) que cumplen condena en prisión por un delito contra una mujer adulta. Para ello se evalúa mediante una escala diseñada al efecto (EPAS) el cambio terapéutico global de los sujetos tras el tratamiento y también su evolución en diez variables terapéuticas específicas (como asertividad, disposición al cambio personal, distorsiones cognitivas, etc.). La comparación intra-sujetos indicó que los agresores tratados mejoran, en términos terapéuticos, tanto globalmente como en la mayoría de las variables específicas evaluadas (mejoras que no se produjeron en el grupo control). Así mismo, se encontraron asociaciones significativas relevantes entre diversas variables terapéuticas. Finalmente, se comentan críticamente los resultados obtenidos y algunos de los retos existentes en el campo de la evaluación del tratamiento psicológico de los agresores sexuales.
Official data about sexual offences show that the prevalence of sex crimes is relatively low among criminal behaviours. For example, reported sex crimes accounted for only 0.94% of all the serious crimes committed in Spain in 2014 (Dirección General de Instituciones Penitenciarias, 2014). Nonetheless, the number of sex offences not officially reported by victims may be substantially higher (Abrahams et al., 2014).
However, sex offences are among the most serious crimes because of their severe damage to the victims, usually women and children (Echeburúa & Guerricaechevarría, 2011; European Agency for Fundamental Rights, 2014; Fergusson, McLeod, & Horwood, 2013; Lopez-Castroman et al., 2013; Wößner, 2016). Also, sexual offences carry a huge social stigma and, justifiably, arouse intense feelings of personal insecurity. Particularly, the crimes committed by sex offenders released after serving their sentences generate public concern and alarm.
For all these reasons, it is important to analyse and enhance our scientific understanding of sexual offending behaviour in order to improve prevention and to apply more effective treatment with convicted offenders. This paper focuses specifically on the effectiveness of the psychological treatment administered to rapists or sex offenders serving prison sentences in Spain for sexual assaults on adult women1.
Causes and Correlates of Sex OffencesThe initiation and development of human sexuality from puberty generally involves a range of appropriate prosocial experiences which normally include sexual self-satisfaction and voluntary sexual interaction with peers. As a result of these sexual experiences, during adolescence individuals usually learn prosocial sexual repertoires and also acquire the necessary sexual controls, inhibitions, and taboos, in particular with regard to avoiding forced sex. However, juveniles who have suffered serious traumatic experiences in childhood (psychological or sexual abuse, inconsistent rearing in the family, and so on) may have special difficulty in developing these indispensable sexual controls and inhibitions, and as a result show more risk of sexual offending (Becker & Johnson, 2001; Hamby, Finkelhor, & Turner, 2012; Marshall, Laws, & Barbaree, 2013; Marshall, Marshall, Serran, & Fernandez, 2006; Redondo & Martinez, 2012; Zurbriggen, Gobin, & Freyd, 2010). In this respect, a significant proportion of sex offenders have more varied and atypical sexual experiences at an early age than is the norm, including the use of violent pornography (Barbaree & Langton, 2006; Becker & Hunter, 1997; Cale, Smallbone, Rayment-McHugh, & Dowling, 2016; Seto & Eke, 2015) or actual childhood experiences of physical or sexual abuse (Fergusson et al., 2013; Gunby & Woodhams, 2010; Mancini, Reckdenwald, & Beauregard, 2012; Seto, 2008). These experiences of victimisation may stimulate a deviant sexual arousal and a preference for violent sex.
Rapists may also have suffered traumatic family abandonment, affective rejection, negligent parents, erratic styles of upbringing, and so on during childhood (Maniglio, 2012). These traumatic early experiences tend to be related to severe emotional and communicative deficits, relationship problems, and social isolation (Ford & Linney, 1995; Hendriks & Bijleveld, 2004; Hulme & Middleton, 2013; Katz, 1990; Porter, Newman, Tansey, & Quayle, 2015; Van Wijk, 1999). To solve or compensate these problems, individuals may use inappropriate coping mechanisms such as a hyper-sexualisation of their emotionality and conduct, including deviant fantasies and masturbation (Mancini et al., 2012; Marshall & Marshall, 2014).
On the other hand, rapists usually show numerous “cognitive distortions”, that is, erroneous thoughts about women in general, their victims in particular, and the feasibility of the use of violence in social interactions. Such thoughts hamper their capacity to properly interpret and recognise the emotions, needs, desires, and intentions of others and in particular of their victims (Abel, Becker, & Cunningham-Rathner, 1984; Craig, Browne, Beech, & Stringer, 2006; Hempel, Buck, van Vugt, & van Marle, 2015; Marshall, Marshall, & Kingston, 2011; Merdian, Curtis, Thakker, Wilson, & Boer, 2014; Whitaker et al., 2008). In some individuals, cognitive distortions about sexual interactions have a leading aetiological role in their sexual offending, while in other cases cognitive distortions operate mainly not as aetiological factors but as post hoc rationalisations for justifying their actions (Maruna & Mann, 2006; Ward, Hudson, Johnston, & Marshall, 1997).
Many rapists also show severe deficits in empathy and social skills. They tend to exhibit a marked egocentrism and severe difficulties in imagining and figuring out realistically what others, and particularly their victims, might think, want, and feel (Cohen & Strayer, 1996; Fernandez & Marshall, 2003; Geng, Xia, & Qin, 2012). Several studies have found a direct relationship between individuals’ early sexual victimisation and exposure to pornography and the lack of empathy shown later by sex offenders (Becker & Johnson, 2001; Fergusson et al., 2013; Hempel et al., 2015; Mann & Barnett, 2013; Marshall, Marshall, Serran, & O’Brien, 2009). These empathic deficiencies may also undermine the rapists’ ability to establish meaningful and appropriate interpersonal relationships, including interactions at school and at work, and the establishment of affective bonds (Agnew, 2014; Beavin, 2015).
Some rapists are versatile offenders, in the sense that their criminal behaviour is not restricted to sexual offences but may extend to theft, physical assault, and so on. This versatility may contribute to consolidating and stabilising the rapist's criminal career, since sexual and nonsexual crimes may interact reciprocally as a part of a more general, chronically deviant life style (Lussier, 2005; Piquero, Farrington, Jennings, Diamond, & Craig, 2012; Seto & Lalumière, 2010; Sewall, Krupp, & Lalumière, 2013; Sigre-leirós et al., 2016).
Criminogenic Needs and TreatmentAs can be seen, many sex offenders display numerous personal and social deficits and risk factors (including feelings, attitudes, values, and behaviours) often associated with their criminal conduct (Beech & Mann, 2002; Marshall et al., 2013; Marshall & Marshall, 2014). In order for sex offenders to desist from crime, favourable changes in all of these risk factors are required (Brown, 2015; Day, Casey, Ward, Howells, & Vess, 2010). Thus, the main objective of the current psychological interventions with sex offenders (which are generally applied within the prison setting) is to promote individuals’ internal changes. This includes a more realistic interpretation of their crimes and behavioural consequences, as well as the improvement of empathy, self-esteem, assertiveness, and so on.
Current theories surrounding sex offenders’ rehabilitation propose to focus interventions on the abovementioned deficits and risk factors in order to reduce recidivism risk (Abbey, Jacques-Tiura, & LeBreton, 2011; Andrews, Bonta, & Wormith, 2011; Beech, Mandeville-Norden, & Goodwill, 2012; Echeburúa & Amor, 2010; Marshall et al., 2013; Rich, 2009). Particularly, it needs to be focussed on the change of dynamic risk factors or criminogenic needs, which are those modifiable variables commonly associated with an increased offending risk (Andrews & Bonta, 2016; Andrews & Dowden, 2007). Different meta-analyses have concluded that therapeutic effectiveness with offenders increases as many criminogenic needs (and fewer non-criminogenic needs) are addressed (Hanson, Bourgon, Helmus, & Hodgson, 2009a; Martínez-Catena, Redondo, Frerich, & Beech, 2016; Mcgrath, Cumming, Burchard, Zeoli, & Ellerby, 2009).
The criminogenic needs most commonly associated with sexual recidivism and also addressed in sex offender treatments are: intimacy deficits, hostility towards women, emotion regulation problems, social isolation or rejection, impulsivity, poor cognitive problem-solving skills, and sexual deviation (Hanson et al., 2009a; Hanson & Morton-Bourgon, 2004; Lussier, 2005; Yates, 2009).
Other factors, despite their lower direct empirical relationship with sexual recidivism, are included in sex offenders’ treatment as long as they could enhance treatment responsivity and participants self-efficacy (Mcgrath et al., 2009). They are factors like denial or minimization, low self-esteem, lack of empathy, general psychological problems, etc.
For instance, McGrath et al. (2009) highlighted that 90% of sex offender programs include a victim empathy component, despite research indicating that a lack of victim empathy is not firmly related to recidivism (Mann, Hanson, & Thornton, 2010). Nevertheless, empathy could be useful as a treatment objective, as it is strongly correlated with self-esteem, shame, and cognitive distortions, possibly influencing each other in treatment improvement (Marshall et al., 2009). In this way, changes in self-esteem as a result of treatment are highly correlated with changes in empathy over the course of treatment (Marshall, Anderson, & Champagne, 1997). Also, Webster and Beech (2000) found that offenders’ empathy deficits in relation to their victims were strongly related to measures of cognitive distortions.
Similarly, cognitive distortions are strongly related to the aetiology of sexual offence behaviour, but their relationship with treatment efficacy is complex. In terms of treatment, cognitive distortions are assessed and treated both as crime precipitant and maintaining factor (Hudson, Wales, Bakker, & Ward, 2002). Nonetheless, a recent meta-analytic review showed a significant association between the improvement of attitudes (one of the possible processes involved in cognitive distortions) and the reduction of sexual recidivism (Helmus, Hanson, Babchishin, & Mann, 2013). Furthermore, it has been found that cognitive distortions can be tied back to emotions which are treated through the self-management component in sex offenders’ rehabilitation processes (Abracen & Looman, 2016). So, teaching participants to recognize and differentiate emotions from each other (in particular sadness, anxiety, anger, hostility, loneliness, and shame) could help to reduce cognitive distortions about violence.
Taking into account this close relationship between several criminogenic needs, it is expected that simultaneously addressing each variable in treatment would help improve participant's other personal and social difficulties that are not directly included in the intervention program.
The Effectiveness of Treatment in Sex OffendersAt present, the most frequently applied and most effective sex offenders’ treatments are the cognitive-behavioural programmes based on the Risk-Needs-Responsivity (RNR) model (Andrews & Bonta, 2016; Prentky, Righthand, & Lamade, 2016; Prentky & Schwartz, 2006). A pioneering treatment programme for sex offenders was initially developed in Canada by Marshall and his team (Barbaree & Langton, 2006; Barbaree & Marshall, 2006; Brown, 2015; Marshall, Marshall, Serran, & O’Brien, 2011), which has become the foundation of most subsequent sex offender programmes in different countries. For instance, in the UK the Home Office Prison Service designed specific versions for sex offender treatment (Brown, 2015; Hollin & Palmer, 2006): the Sex Offender Treatment Programme, SOTP core, whose central therapeutic aim is the confrontation and restructuring of cognitive distortions and crime justifications; the SOTP Adapted Programme for sex offenders with intellectual disabilities; the Better Lives Booster SOTP Programme, a follow-up treatment for higher risk individuals; a treatment format for lower risk offenders; a more modern intervention for internet sexual offenders; interventions for sex offenders in the community, and so on. Other European countries that also offer specialised programmes for sex offenders at prisons or in the community are Sweden2, Norway3, Denmark, Finland4, Holland, and Belgium.
As far as treatment effectiveness is concerned, the interventions applied with sex offenders in different countries in general show positive results. The recidivism rate of treated sex offenders ranged between 9% to 11%, compared with a rate of around 17% for untreated sex offenders (Hanson et al., 2009a; Hanson, Bourgon, Helmus, & Hodgson, 2009b; Hanson, Gordon, & Harris, 2002; Hanson & Morton-Bourgon, 2004; Lösel & Schmucker, 2005; Marshall & Marshall, 2014).
In Spain, the first specific programme for sex offenders was created by Garrido and Beneyto (1996, 1997) based on the programmes applied in other countries and aiming to meet the specific therapeutic needs of imprisoned sex offenders. The Sexual Offending Control Programme (SOCP) is a cognitive-behavioural intervention based on the RNR model, similar to the programmes applied with sex offenders in Canada, the US, and the UK (Marshall, Marshall, & Kingston, 2011; Marshall, Marshall, Serran et al., 2011; Olver & Wong, 2013). The SOCP was applied for the first time in 1996 in two prisons in Barcelona and its use subsequently extended to other Spanish prisons. A revised version of the programme (Ministerio del Interior, 2006) is currently administered in more than 40 Spanish prisons. Some of the results of these trials are analysed in this paper.
The SOCP lasts for one to two years. It is group-based, administered to both rapists and child molesters, and delivered twice weekly in sessions lasting about two and half hours. The treatment focuses on the following intervention elements: 1) relaxation training; 2) analysis of history and personal development of each subject; 3) cognitive distortions; 4) emotional regulation; 5) violent behaviour; 6) coping techniques; 7) empathy with victims; 8) training for a positive way of life; 9) sex and health education; 10) change of sexual impulse; and 11) relapse prevention.
The first effectiveness assessment of the SOCP was published in 2005 by Redondo and colleagues, who compared a group of 49 treated sex offenders with a similar group of 74 untreated peers. After a four-year follow-up, the official recidivism rate of treated sex offenders was 4.1% compared with 18.2% in the untreated group: a 14-point reduction (Redondo, 2006; Redondo, Navarro, Martínez, Luque, & Andrés-Pueyo, 2005).
A second evaluation of the SOCP, conducted independently in a prison in Madrid, obtained very similar results (Valencia, Andreu, Minguez, & Labrador, 2008). From a group of 22 treated sex offenders, 4.5% relapsed compared with a rate of 13% in the control group (n=21).
The evaluation of recidivism after treatment is an essential measure in a criminal matter as serious as sexual offending (Marshall & Marshall, 2014). But, at the same time, measuring recidivism alone is clearly insufficient in order to understand how the treatment works and to identify the personal changes that treatment promotes in offenders. For this reason, the Spanish Prison Management Service recently decided to complement the assessment of recidivism with the analysis of the individuals’ therapeutic change, or therapeutic efficacy. The Psychological Assessment Scale for Sex Offenders (PASSO) was designed for this evaluation (Redondo, Martínez, Ramírez-Pérez, & Martínez-Catena, 2016), whose main objective is to assess the specific therapeutic changes and improvements experienced by sex offenders as a result of their participation in the programme (Martínez-Catena et al., 2016; Redondo, Martínez-Catena, & Luque, 2014).
The present study describes this evaluation of the therapeutic efficacy of the SOCP, aiming above all to assess the possible therapeutic changes produced in rapists after participation.
As a general hypothesis, we expected participants in treatment to present overall improvements on the different psychological variables that are the therapeutic objectives of the programme. We also expected the various therapeutic variables assessed to improve after treatment, though not at the same rate.
MethodParticipantsThe sample comprised 153 adult men, incarcerated for sexual offences against an adult woman (hereinafter, rapists). The primary inclusion criterion was that the participants had completed the assessment instrument (described below) both before and after the initiation of sex offender's treatment.
MeasuresThe Psychological Assessment Scale for Sex Offenders (PASSO) (Redondo et al., 2016) used here was designed to assess individual change in different sex offenders’ therapeutic variables.
Several already published and validated scales were taken into account in the design of the PASSO. Items on these scales were translated and adapted, and new items were created to define a first broad version of the new scale. These items were assessed by means of a thorough methodological process, in order to prove their capacity and sensitivity (Martínez-Catena & Redondo, 2016). Following a process of progressive item elimination, three successive scale versions were generated.
The current scale (PASSO-3) is divided into two parts. The first one assesses most of the therapeutic variables considered here (with the exception of empathy, which is specifically evaluated in the second part). This first part contains 103 items, which respondents rate on a Likert-type scale of 0-3 points. The ten following therapeutic variables are evaluated: anxiety in normal/habitual sexual situations (13 items, α=.94), assertiveness (13 items, α=.54), readiness to change (7 items, α=.76), cognitive distortions justifying child abuse (10 items, α=.80), cognitive distortions about women and the use of violence in sexual interactions (10 items, α=.74), impulsivity (16 items, α=.84), aggressiveness (11 items, α=.80), social self-esteem (18 items, α=.84), feelings of loneliness and isolation (5 items, α=.76), and empathy (118 items, α=.81).
The second part is weighted separately due to the relevance and complexity of empathy assessment. Empathy – or individuals’ ability to feel emotionally concerned by the suffering of others – is evaluated here by means of the Rapist Empathy Scale (Fernandez & Marshall, 2003) which includes 118 items answered on a 4-point Likert scale. For this evaluation, the scale was translated and adapted to Spanish. Subjects were asked about their feelings in three imaginary scenarios in which a woman has suffered serious injury due to (1) an accident, (2) sexual aggression by another offender (not the respondent), and (3) sexual aggression by the respondent. In general, scores for the three scenarios and an overall empathy score are produced, but in the present study only the third scenario (sexual aggression by the respondent) was analysed.
The overall PASSO score (which reflects each individual's overall position in the therapeutic variables assessed) ranges in absolute terms between 0 and 384 points, with higher scores indicating better performance or improvement on the therapeutic variables evaluated (i.e., a decrease in risk factors for sexual offending). However, apart from absolute scores, in order to facilitate the interpretation and comparison, each specific PASSO subscale was assigned a score between 0 and 10 and the overall scale was assigned a score between 0 and 100.
In parallel to the use of PASSO, a sociodemographic and criminal record datasheet was also designed and applied in order to compile information on the subjects’ characteristics, health, family, education, work, criminal history, details of the sex crimes committed, and so on.
ProcedureHere we present the preliminary results of an ongoing Spanish study on the efficacy of treatment applied to rapists. The global study, underway since 2005, has a mixed within-subject, and in the near future between-group design, in which treated and control subjects are assessed before and after treatment. Subjects are recruited from 40 Spanish prisons that are currently applying the Sexual Offending Control Programme (SOCP). The treatment group consists of all subjects who voluntarily participate in treatment in any prison and accept to fill out the questionnaires included in the global study. The control group will be made up of sex offenders who are on the treatment waiting list. These subjects are not included in the current study, due to the ongoing evaluation process. All the information requested in this global study is strictly supervised and controlled by the technical and ethical services of the Spanish Prison Department, Ministry of Interior. Also according to the Spanish law, all the cases are anonymously coded in order to preserve the personal identity and rights of all the participants.
The assessment instruments (the PASSO and the sociodemographic and criminal datasheet) were applied pre- and post-treatment by members of the prison's therapeutic staff (usually psychologists, social workers, and educators). These experts received a 5-hour training session in the application of the assessment tools, led by the instrument designers.
For methodological reasons, cases for which more than 10% of items presented missing data were removed from analysis. For the remaining subjects, the estimation means (expectation-maximisation) method was used to replace any missing data.
Data AnalysisIn order to analyse the intra-subject differences between the two assessments, the t-test comparison of means for related groups was applied. The Bonferroni post-hoc correction test was applied to all the analyses performed (established at a bilateral p value < .004). Size effects were also computed for the intra-subject differences found using the free access GPower 3.1 software.
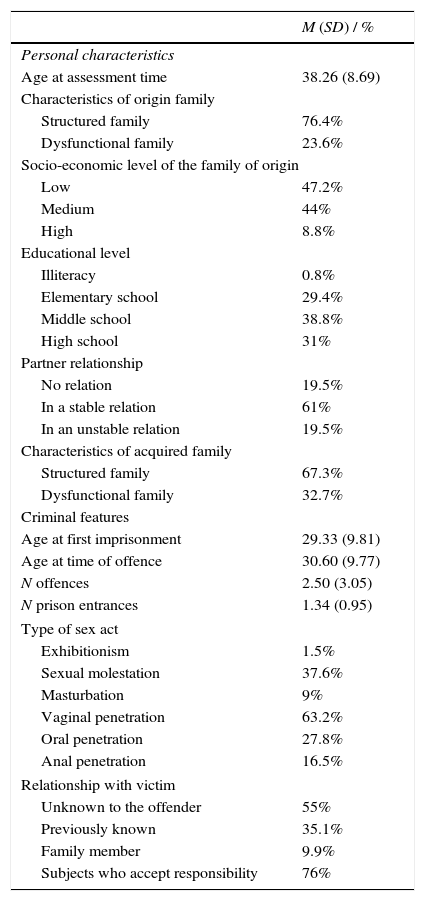
ResultsSample DescriptionTable 1 displays the personal and criminal characteristics of the sample. At the initial assessment period, the mean age of the participants was 38.26. Regarding personal characteristics, 23.6% of the participants come from an unstructured family with a low socioeconomic level (47.2%). Most of them had completed elementary (29.4%) or middle school (38.8%). A total of 61% of the sample was engaged in a partner relationship and had raised a structured family (67.3%). As for criminal features, the mean age at first imprisonment was 29.33, while the mean age at sexual offence commission was 30.60. The mean number of offences committed was 2.50, with most of the prisoners being first-time offenders (mean of 1.34 prison entrances). The majority of the sexual crimes were directed towards an unknown victim (55%) and included serious acts, such as vaginal penetration (63.2% of the cases), as well as less serious acts, such as exhibitionism (1.5%). Finally, the 76% of the participants accepted the responsibility for the crime.
Means and Proportions for the Descriptive Variables of the Sample.
| M (SD) / % | |
|---|---|
| Personal characteristics | |
| Age at assessment time | 38.26 (8.69) |
| Characteristics of origin family | |
| Structured family | 76.4% |
| Dysfunctional family | 23.6% |
| Socio-economic level of the family of origin | |
| Low | 47.2% |
| Medium | 44% |
| High | 8.8% |
| Educational level | |
| Illiteracy | 0.8% |
| Elementary school | 29.4% |
| Middle school | 38.8% |
| High school | 31% |
| Partner relationship | |
| No relation | 19.5% |
| In a stable relation | 61% |
| In an unstable relation | 19.5% |
| Characteristics of acquired family | |
| Structured family | 67.3% |
| Dysfunctional family | 32.7% |
| Criminal features | |
| Age at first imprisonment | 29.33 (9.81) |
| Age at time of offence | 30.60 (9.77) |
| N offences | 2.50 (3.05) |
| N prison entrances | 1.34 (0.95) |
| Type of sex act | |
| Exhibitionism | 1.5% |
| Sexual molestation | 37.6% |
| Masturbation | 9% |
| Vaginal penetration | 63.2% |
| Oral penetration | 27.8% |
| Anal penetration | 16.5% |
| Relationship with victim | |
| Unknown to the offender | 55% |
| Previously known | 35.1% |
| Family member | 9.9% |
| Subjects who accept responsibility | 76% |
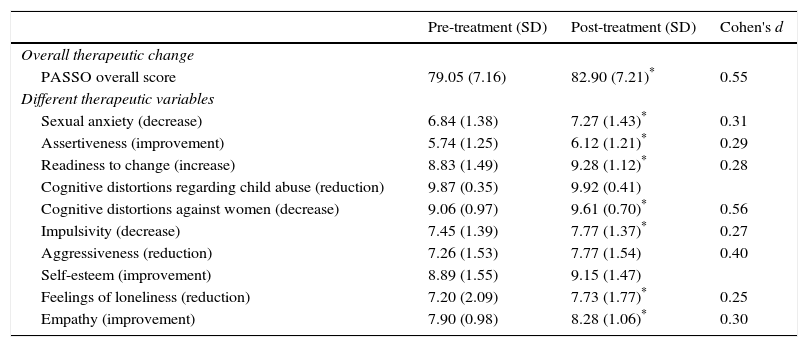
In this section, the overall PASSO score obtained by the treated rapists before and after treatment is analysed and a detailed evaluation of group performance on the different specific therapeutic variables is given. Table 2 shows the PASSO mean scores and standard deviations obtained by participants during the two assessment periods. Significant differences between the scores are indicated (the table also presents the Cohen's d effect size for each variable with a significant change).
Within-subject t-test Comparisons for all PASSO Therapeutic Variables.
| Pre-treatment (SD) | Post-treatment (SD) | Cohen's d | |
|---|---|---|---|
| Overall therapeutic change | |||
| PASSO overall score | 79.05 (7.16) | 82.90 (7.21)* | 0.55 |
| Different therapeutic variables | |||
| Sexual anxiety (decrease) | 6.84 (1.38) | 7.27 (1.43)* | 0.31 |
| Assertiveness (improvement) | 5.74 (1.25) | 6.12 (1.21)* | 0.29 |
| Readiness to change (increase) | 8.83 (1.49) | 9.28 (1.12)* | 0.28 |
| Cognitive distortions regarding child abuse (reduction) | 9.87 (0.35) | 9.92 (0.41) | |
| Cognitive distortions against women (decrease) | 9.06 (0.97) | 9.61 (0.70)* | 0.56 |
| Impulsivity (decrease) | 7.45 (1.39) | 7.77 (1.37)* | 0.27 |
| Aggressiveness (reduction) | 7.26 (1.53) | 7.77 (1.54) | 0.40 |
| Self-esteem (improvement) | 8.89 (1.55) | 9.15 (1.47) | |
| Feelings of loneliness (reduction) | 7.20 (2.09) | 7.73 (1.77)* | 0.25 |
| Empathy (improvement) | 7.90 (0.98) | 8.28 (1.06)* | 0.30 |
Related sample t-test results comparing before and after treatment were carried out. Participants presented significant differences in the PASSO overall score after treatment, rising to 82.90 (SD=7.21) compared with a pre-treatment score of 79.05 (SD=7.16), which is a significant improvement of 3.85 points, t(152)=-6.77, p<.001.
In addition to the overall therapeutic score, results also indicate significant differences in the treated participants for eight of the ten therapeutic subscales (all but reduction of cognitive distortions regarding child abuse and improvement of self-esteem).
Figure 1 represents the differences between the pre and post scores obtained by participants on all the therapeutic variables mentioned. The post hoc size effects for the subscales that revealed significant differences are also indicated.

The significant differences shown in Figure 1 indicate improvements in the treated participants, both in their overall performance on the PASSO and on the specific therapeutic variables mentioned above.
Post hoc effect sizes range from small to moderate (d=0.25 to d=0.56). Seemingly, the most modest increase in the scores was obtained on the reduction of feelings of loneliness subscale with a small effect size (d=0.25). By contrast, the variable decrease in cognitive distortions against women showed the highest effect size (d=0.56). The effect size of the PASSO overall score was also moderate (d=0.55).
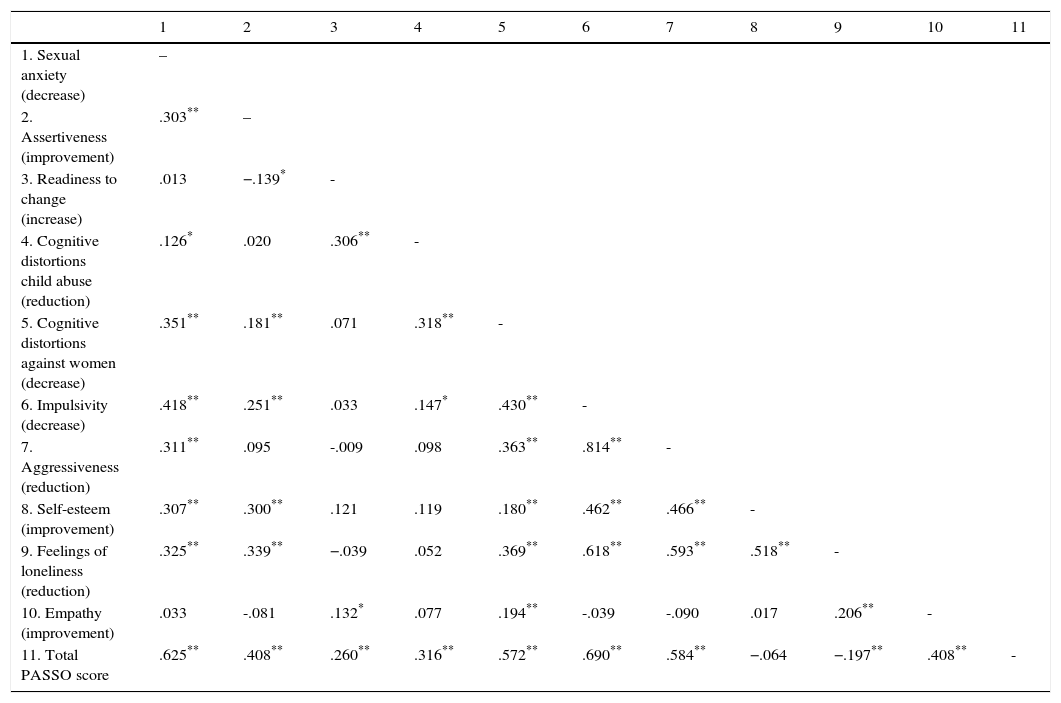
Association Between Criminogenic NeedsTable 3 shows the Pearson's correlations between the PASSO subscales and the overall punctuation. As can be seen high and positive correlations are shown between the subscales decrease of impulsivity and reduction of aggressiveness (r=.814). Also, the subscale reduction of feelings of loneliness shows a high correlation with decrease of impulsivity (r=.6.18), reduction of aggressiveness (r=.593), and improvement of self-esteem (r=.518). Other positive moderate associations emerge between the subscale decrease of impulsivity and the subscales decrease of sexual anxiety and decrease of cognitive distortions against women (r=.418, r=.430, respectively); as well as between the subscale improvement of self-esteem with the subscales decrease of impulsivity and reduction of aggressiveness (r=.462, r=.466, respectively). Other relevant associations can be found in Table 3.
Pearson's Correlations of PASSO.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Sexual anxiety (decrease) | – | ||||||||||
| 2. Assertiveness (improvement) | .303** | – | |||||||||
| 3. Readiness to change (increase) | .013 | −.139* | - | ||||||||
| 4. Cognitive distortions child abuse (reduction) | .126* | .020 | .306** | - | |||||||
| 5. Cognitive distortions against women (decrease) | .351** | .181** | .071 | .318** | - | ||||||
| 6. Impulsivity (decrease) | .418** | .251** | .033 | .147* | .430** | - | |||||
| 7. Aggressiveness (reduction) | .311** | .095 | -.009 | .098 | .363** | .814** | - | ||||
| 8. Self-esteem (improvement) | .307** | .300** | .121 | .119 | .180** | .462** | .466** | - | |||
| 9. Feelings of loneliness (reduction) | .325** | .339** | −.039 | .052 | .369** | .618** | .593** | .518** | - | ||
| 10. Empathy (improvement) | .033 | -.081 | .132* | .077 | .194** | -.039 | -.090 | .017 | .206** | - | |
| 11. Total PASSO score | .625** | .408** | .260** | .316** | .572** | .690** | .584** | −.064 | −.197** | .408** | - |
In recent years, considerable support has been given for the development of treatment programmes for prison inmates and for the evaluation of their effectiveness. Given the gravity of their offences, rapists represent a particularly important subsample of the prison population. They are the focus of the therapeutic efficacy analysis presented here.
The current paper is an evaluation of the sex offenders’ treatment program applied in Spain since 2005, the Sexual Offending Control Programme (SOCP). Here, individual therapeutic changes are assessed through the specific scale called the Psychological Assessment Scale for Sex Offenders (PASSO) (Redondo et al., 2016). The PASSO scale evaluates ten therapeutic variables (including assertiveness, cognitive distortions about women and the use of violence, impulsivity, etc.). According to the literature, improvements in these variables as a result of treatment are positively associated with rehabilitation and desistance from crime. For each respondent, the PASSO provides a global therapeutic improvement score and ten specific scores corresponding to the different therapeutic subscales assessed.
The analysis of therapeutic improvement of this paper was carried out in a sample of 153 treated rapists. The analysis of overall therapeutic change in subjects revealed a significant improvement in the participants between pre and post-treatment assessments.
In parallel, regarding subjects’ changes on the different specific therapeutic variables, the intra-subject comparison also showed participant improvements on most of the assessed subscales (eight out of ten variables).
The post hoc effect sizes of these therapeutic subscales also put forward that the changes between the pre- and post-periods were distributed unevenly between the different variables. The therapeutic change scores in the pre- and post-treatment assessments in the participants ranged from small to moderate. Besides, the difference found in the PASSO overall score between the periods was moderate and statistically significant.
The results of the administered analyses suggest a general therapeutic improvement in this population of rapists in Spanish prisons.
Pearson's correlations revealed numerous associations between the different therapeutic variables assessed with PASSO. Those results are congruent with other studies that highlight the fact that different criminogenic needs may be highly correlated and possibly influence each other in treatment. In the analyses presented here it can be seen that the subscale decrease of impulsivity was associated with reduction of aggressiveness which could be an expected result. But also, similarly to the results previously presented by Marshall et al. (1997), Marshall et al. (2009), and Webster and Beech (2000), interesting associations have been found between different subscales. For instance, reduction of feelings of loneliness and improvement of self-esteem (which in the literature are not considered strong criminogenic need) are highly connected to relevant criminogenic needs such as decrease of impulsivity and reduction of aggressiveness. This suggests that the improvement of one of these factors could enhance the improvement of the others.
Furthermore, the association found between decrease of impulsivity and the subscales decrease of sexual anxiety and decrease of cognitive distortions against women is important to note. In practice this association could be rather helpful as these specific criminogenic needs are the most difficult to work with. That is, the application of one specific therapeutic technique could also benefit the later application of other techniques. An example is to practice “relaxation” (used commonly for impulsivity control) prior to the initiation of “cognitive distortions’ detection” (in the context of cognitive restructuration).
The analysis of specific therapeutic variables, as proposed here, could help to identify the elements that are likely to be most useful and effective, and also the ones that may require more intensity and commitment. It may help to guide decisions regarding the inclusion, modification, or elimination of some of the current components of interventions in sex offenders.
In general, in studies of therapeutic effectiveness it is difficult to determine whether the changes observed are mainly due to the treatment administered. The present study is no exception. Theoretically, other reasons could also explain the rapists’ individual changes observed here. For instance, imprisoned offenders may improve over time without receiving specific treatment for a variety of reasons, such as the natural development of subjects with age, a decrease in impulsivity and aggressiveness, or the positive effects of general educational activities inside prisons such as formal education, workshops, work, and so on.
Nevertheless, some of the empirical results obtained seem to suggest that participants show an overall therapeutic improvement and for a variety of specific therapeutic changes. At the same time, these positive changes would increase the probability of rehabilitation and desistence from crime.
A relevant methodological shortcoming, which precludes any conclusive claim that the positive changes were directly produced by treatment, is the absence of a control group. Another methodological limitation of this study is that some PASSO items may be too transparent and the subjects learn to give “better” responses in the post-treatment assessment.
In spite of these methodological limitations, the results presented here suggest that interventions with rapists in Spanish prisons have a moderate therapeutic efficacy. To our knowledge, this is the first comprehensive assessment of this issue conducted in Spain that goes beyond the standard, non-specific studies of recidivism rates.
Over the past decades, important advances have been made in the understanding and the prevention and treatment of rape, but major challenges still remain. For instance, as far as the aetiology of sexual aggression is concerned, we are familiar with many of the associated correlates and factors, such as affective deficits and traumatic sexual experiences, family neglect, low self-esteem and so on. But we still know little of the dynamic processes that mediate between these experiential factors and the specific onset of sexually deviant and criminal behaviour.
Huge scientific challenges remain regarding the prevention of this criminal activity and the treatment of rapists and other sex offenders. Most of the current preventive efforts in this area have concentrated on the application of specialised treatments, which essentially reach the individual level of this problem. Nevertheless, in the future, other kinds of preventive actions at educational and community level will probably be necessary to prevent, or at least control, sexual aggression more effectively.
Financial SupportThis research was funded by grants SEJ2005-09170-C04-01 and PSI2009-13265 from Ministerio de Ciencia y Innovación [Spain's Ministry of Science and Innovation] and by grant PSI2013-47043-C2-2-R from Ministerio de Economía y Competitividad [Spain's Ministry of Economy and Competitiveness]. Financial support (FBG305486) was also provided by the Secretaría General de Instituciones Penitenciarias del Ministerio de Interior, Gobierno de España [Correctional Services, Home Office, Government of Spain].
Conflict of InterestThe authors of this article declare no conflict of interest.
Generally, in strict legal terms, the word “rape” is used to refer to sexual crimes involving forced sexual penetration. However, in criminological analyses the term tends to include other forms of violent sexual abuse that do not necessarily involve penetration. This is the definition we apply here.
See <http://www.government.se/>.
