

The da Vinci robot was initially adapted for use in radical prostatectomy over a decade ago. Some studies have demonstrated advantages over open prostatectomy for short-term outcomes of perioperative morbidity, blood loss, recovery time and surgical margins. However, there seems to be minimal benefit for long-term outcomes of cancer control, continence and potency.
In the United States, about 80% of all radical prostatec tomies are currently performed using the robot, and many institutions—both academic and community-based—have emerged as the leaders for this new technology. The result is that there has been a centralization of care for these com plicated procedures. Many studies show the importance of surgeon experience for prostatectomy outcomes, so this increased centralization may ultimately lead to better outcomes.
At NYU, we are also using the robot for complex renal surgery. The NYU Robotic Surgery Center has 5 da Vinci robots which are used across several surgical disciplines. Although a pure laparoscopic approach is sufficient for small, straightforward tumors, the robot can greatly facili tate partial nephrectomy for complex, endophytic or hilar tumors.
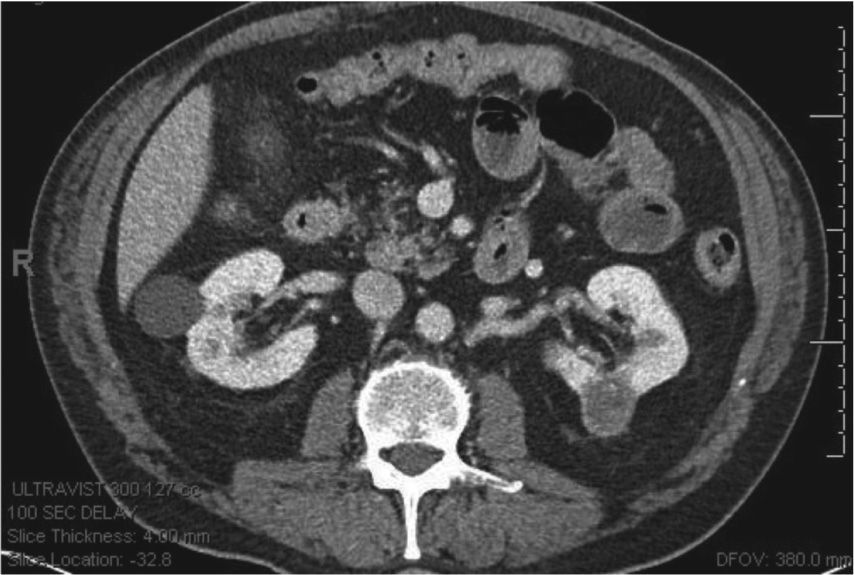
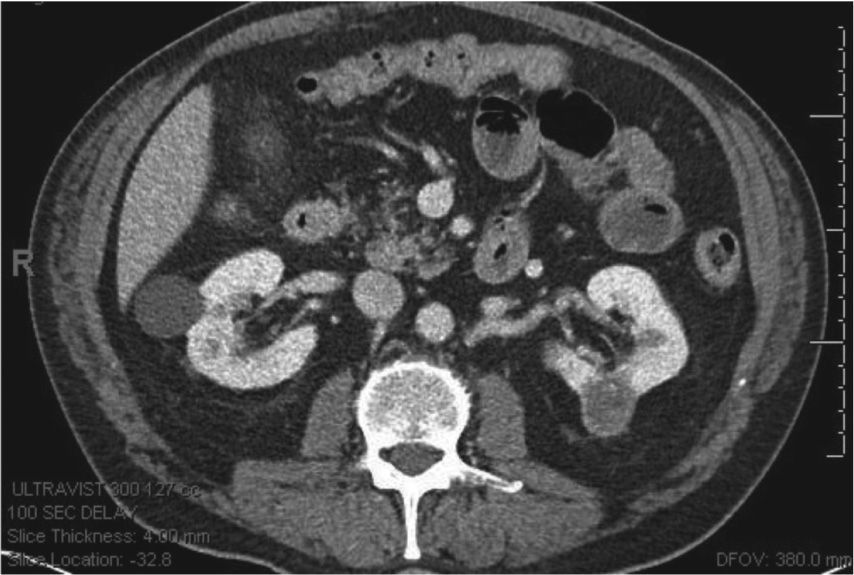
Another useful application of the robot is for posterior tumors using a retroperitoneal approach. At NYU, we frequently perform robotic retroperitoneal partial nephrectomy, which avoids the peritoneal cavity and facilitates quick access to the renal hilum. For example, this patient had 3 tumors in his left kidney which were removed by a robotic retroperitoneal approach (Fig. 1).
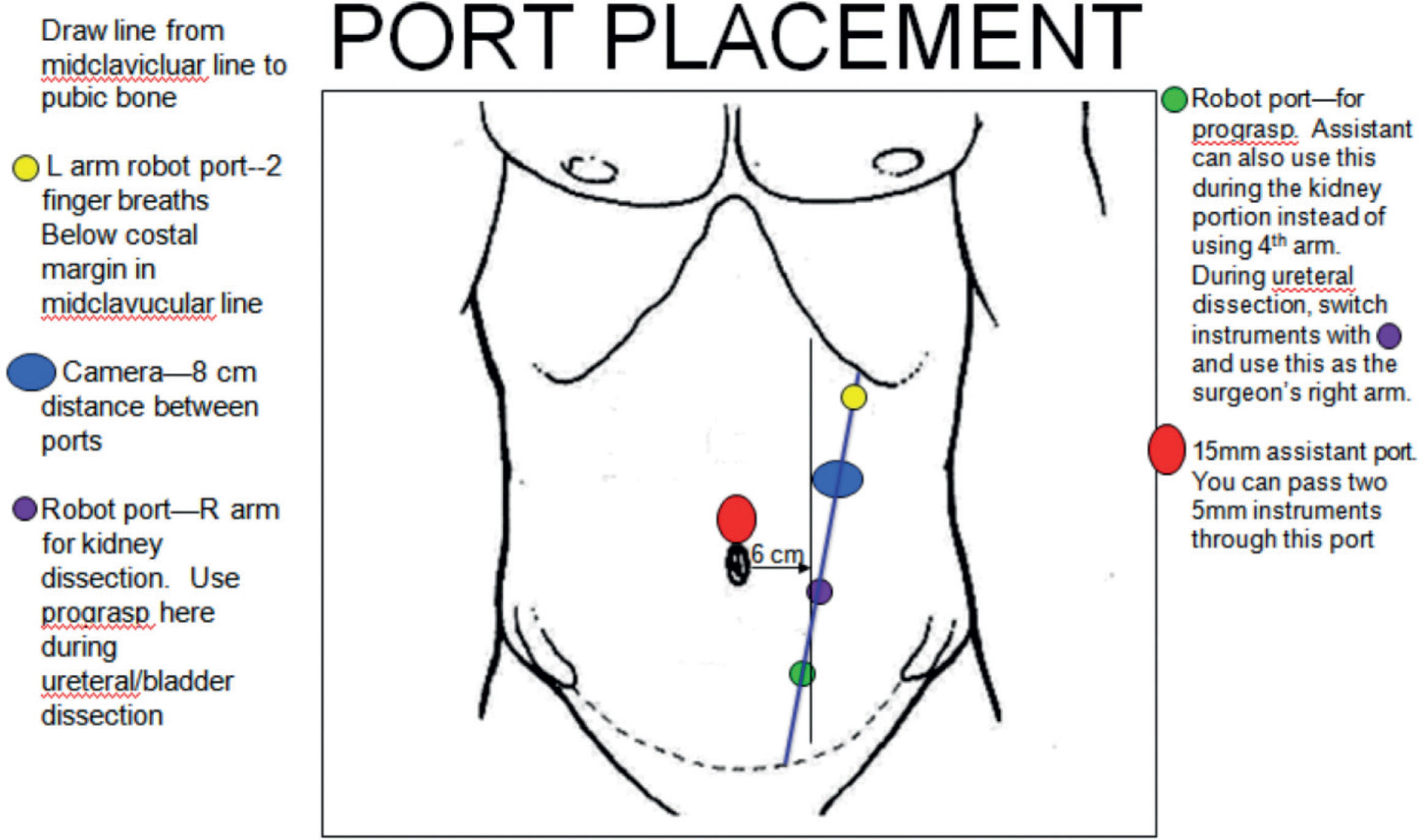
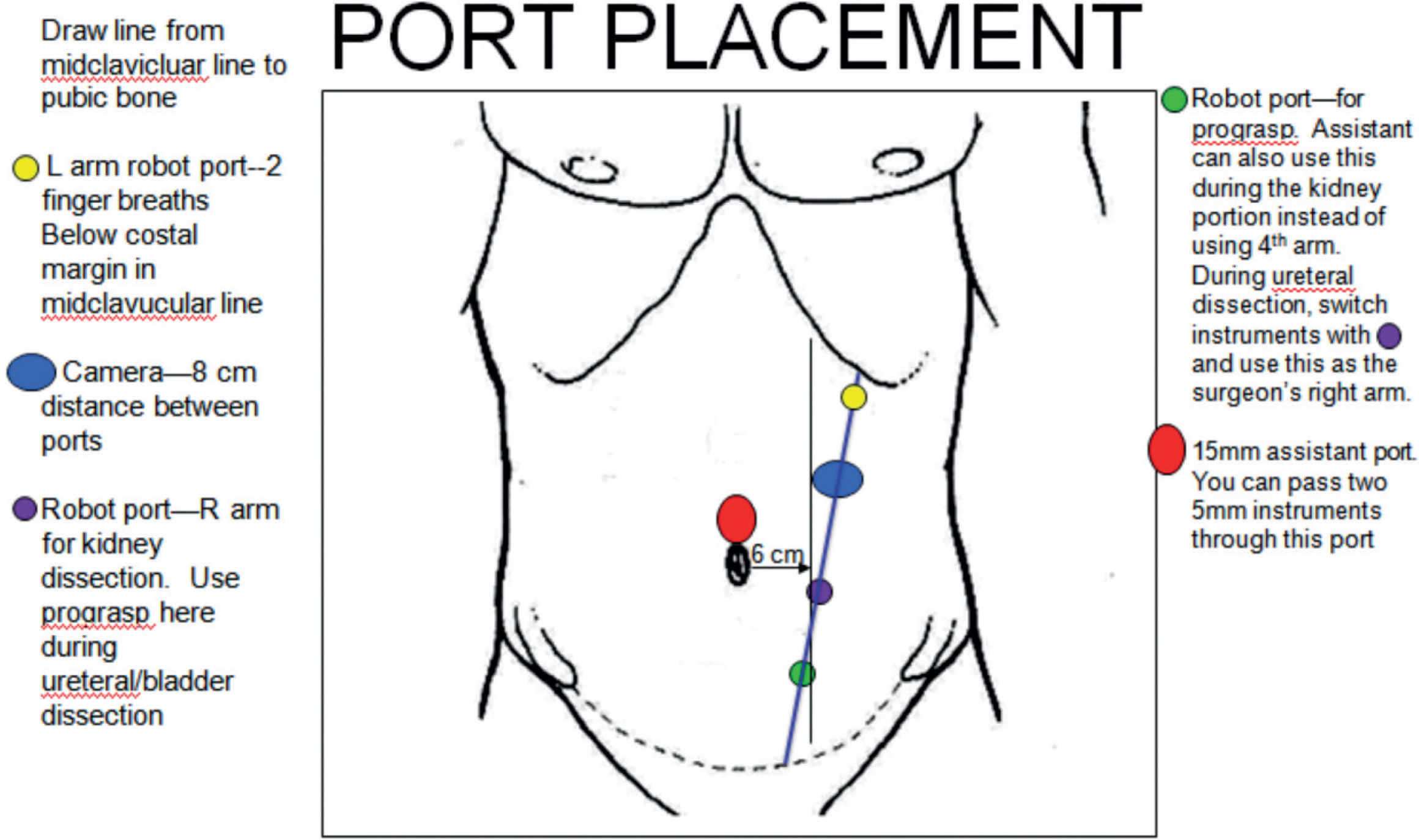
The robot is also invaluable for nephroureterectomy. I recently devised a method of simplified port placement which allows the procedure to be performed without having to redock the robot or change the patient’s position. Using this template avoids instrument clashing and ensures adequate reach from the upper pole of the kidney to the distal ureter. A diagonal line is drawn starting from the subcostal margin in the midclavicular line down to a point on the pubic bone halfway between midline and the lateral border of rectus. A robotic port is placed 2 finger breadths below the subcostal margin, the camera is placed ∼8 cm caudally on the diagonal line, then 2 more robotic ports placed at 8 cm intervals. A 15 mm assistant port is placed in the midline, above or below the umbilicus. This port will facilitate placement of a large specimen bag. Additionally, the assistant can pass two 5 mm instruments at the same time to allow for simultaneous suction and retraction (Fig. 2).
These innovations can reduce operative time and greatly enhance the ability to perform complex urologic surgery, safely and efficiently.
Article available on line.