



Editado por: Dra. Núria Torner CIBER Epidemiologia y Salud Publica CIBERESP Unitat de Medicina Preventiva i Salut Pública Departament de Medicina, Universitat de Barcelona
Más datosThe spread of the COVID-19 pandemic at the end of 2019, with its well-known consequences in terms of morbidity and mortality, has triggered an intense mobilization of the scientific community in the search for knowledge about the SARS-Cov2 virus and the development of a vaccine.
ObjectiveThis study aims to investigate the knowledge, perceptions, attitudes, and intentions of the resident Cape Verdean population regarding the COVID-19 vaccine.
MethodsThis was a descriptive, cross-sectional, and analytical study involving 1704 resident Cape Verdeans, whose ages ranged from 16 to 60 years old and the majority of participants were male (52.6%). The data was collected using the Google form platform between March 9 and 15, 2021.
ResultsThe data indicated that the majority of participants (95.8%) knew of at least one approved vaccine against COVID-19, and this knowledge (74.9%) was obtained from television, radio, and newspapers. The Oxford-AstraZeneca vaccine was the best known (54.1%) among the study subjects and the majority of respondents (69.7%) had enough information to consciously decide whether or not to get vaccinated against COVID-19. The majority (68.0%) of participants were in favor of the COVID-19 vaccine being administered to all interested people. About 59% of participants considered the COVID-19 vaccine to be safe and 49.6% of participants intended to get vaccinated when the time came. The greatest vaccine hesitancy was related to fear of side effects (21.4%), followed by the fact that it was developed too quickly (12.8%). Health professionals were seen as the priority group (81.5%) to be vaccinated.
ConclusionsThe results show that the Cape Verdean population had a good level of knowledge about the COVID-19 vaccine. Despite initial hesitation, the vast majority of participants were willing to get vaccinated. These data suggest that awareness-raising, education, and information campaigns about the COVID-19 vaccine should be strengthened to reduce hesitation and increase confidence and adherence to the COVID-19 vaccine among Cape Verdean residents.
La propagación de la pandemia de COVID-19 a finales de 2019, con sus conocidas consecuencias en términos de morbilidad y mortalidad, ha desencadenado una intensa movilización de la comunidad científica en la búsqueda de conocimientos sobre el virus SARS-Cov2 y el desarrollo de una vacuna.
ObjetivoEste estudio pretende investigar los conocimientos, percepciones, actitudes e intenciones de la población caboverdiana residente en relación a la vacuna COVID-19.
MétodoSe trata de un estudio descriptivo, transversal y analítico en el que participaron 1.704 caboverdianos residentes, cuyas edades oscilaban entre los 16 y los 60 años y la mayoría de los participantes eran hombres (52,6%). Los datos se recogieron utilizando la plataforma de formularios de Google entre el 9 y el 15 de marzo de 2021.
ResultadosLos datos indicaron que la mayoría de los participantes (95,8%) conocían al menos una vacuna aprobada contra el COVID-19, y este conocimiento (74,9%) lo obtuvieron de la televisión, la radio y los periódicos. La vacuna de Oxford-AstraZeneca era la más conocida (54,1%) entre los sujetos del estudio y la mayoría de los encuestados (69,7%) disponía de información suficiente para decidir conscientemente si vacunarse o no contra el COVID-19. La mayoría (68,0%) de los participantes estaba a favor de que la vacuna COVID-19 se administrara a todas las personas interesadas. Alrededor del 59% de los participantes consideraban que la vacuna COVID-19 era segura y el 49,6% de los participantes tenían intención de vacunarse llegado el momento. Las mayores dudas sobre la vacuna estaban relacionadas con el miedo a los efectos secundarios (21,4%), seguido del hecho de que se desarrollara demasiado rápido (12,8%). Los profesionales sanitarios se consideraron el grupo prioritario (81,5%) para vacunarse.
ConclusionesLos resultados muestran que la población caboverdiana tenía un buen nivel de conocimiento sobre la vacuna COVID-19. A pesar de las dudas iniciales, la gran mayoría de los participantes estaban dispuestos a vacunarse. Estos datos sugieren que deberían reforzarse las campañas de concienciación, educación e información sobre la vacuna COVID-19 para reducir las dudas y aumentar la confianza y la adherencia a la vacuna COVID-19 entre los residentes de Cabo Verde.
The emergence of COVID-19, a respiratory disease caused by the SARS-CoV-2 virus, which broke out at the end of 2019 in the city of Wuhan, China, triggered an intense mobilization of the international scientific community in the search for knowledge about the virus and the development of a vaccine, considered an effective strategy to control the COVID-19 pandemic.1,2 Due to the seriousness of the situation, the active dynamic of scientists in finding a vaccine has taken on unprecedented urgency worldwide. Several governmental and non-governmental organizations, as well as the private sector, have made efforts, providing technical and financial resources in an attempt to approve an effective vaccine against the SARS-CoV-2 virus as soon as possible.3 Mass vaccination of the population was considered one of the most cost-effective measures to control the pandemic and reduce its impact on health, the economy, and society.4 According to the World Health Organization (WHO), in December 2020, there were more than 200 candidate vaccines for immunization in development, of which more than 50 had already been tested on humans.5 Thanks to the efforts and dedication of the international scientific community, the first vaccines (Pfizer/BioNTech and Moderna with 90% and 94.5%) for the immunization of the population against COVID-19 were approved at the end of 2020.5 In this sense, in the first quarter of 2021, the process of vaccinating selected groups (priority groups according to each country's vaccination plan) began worldwide.6
It should be noted that the process of producing vaccines against COVID-19 did not begin with the emergence of COVID-19 in 2019, because long before the emergence of the new coronavirus (SARS CoV-2) in 2019, in recent decades, the pharmaceutical industries and the international scientific community have been encouraged to produce vaccines quickly and effectively against the epidemics of H1N1, Ebola, Zika, and currently, the SARS-CoV-2 virus.7
Consequently, as clinical research into the development of the COVID-19 vaccine progresses, fake news against the immunizer is on the rise everywhere. Conspiracy theories that the vaccine under development was a ploy to monitor people from an injected microchip, or that the vaccine caused autism spectrum disorder, among other theories and (mis)information to discourage the population.8–10
Disinformation in the context of the COVID-19 pandemic has gained widespread prominence, leading the WHO, academic and government institutions to launch communication platforms aimed at uncovering and preventing the spread of fake news, a contemporary phenomenon that influences decision-making and behavior, and alters the perception of risk.11
Experts point out that disinformation disproportionately affects individuals with less access to information channels, who are more likely to ignore warnings from health organizations and governments about prevention measures.8
Vaccine hesitancy is not a recent phenomenon; according to data from previous studies, the population's relationship with vaccines has not always been peaceful. Contestation and resistance are part of the very history of vaccine development, reflected in the anti-vaccine movements scattered all over the place.12
According to studies carried out on this subject, vaccine hesitancy is defined as a refusal to be vaccinated, despite the availability of vaccination services. Vaccine hesitancy is complex and context-specific and varies by time, place, and vaccines. It is influenced by factors such as complacency, convenience, and trust.13,14
The WHO defines vaccine hesitancy or refusal as a delay, despite availability, in administering the recommended vaccines.15 Hesitation encompasses a wide range of attitudes, from fear to outright refusal, with different degrees.
The COVID-19 vaccine has brought to light the conflict between the individual and the community.8 According to the author, collective immunity is achieved when vaccination is carried out in large numbers and reaches high coverage. This immunity provides, in addition to the individual protection of the vaccinated person, the elimination of the circulation of the infectious agent in the environment and the indirect protection of susceptible people.8
Despite the obstacles in developing the vaccine and an effective treatment against COVID-19, experts argue that the COVID-19 pandemic has (re)placed science as the central element in combating the pandemic and highlighted health professionals as the essential agents in tackling it.9
There is a consensus among experts, government officials, non-governmental organizations, and the general population that vaccination is the safe way to control the pandemic, reduce the international health crisis, and reduce the economic and social impacts caused by the COVID-19 pandemic.
Experts argue that, with the exception of the use of drinking water, vaccines are one of humanity's greatest advances in the fight against disease, with the basic principle of exposing the body to antigens, substances present in microorganisms, thus stimulating the production of antibodies through an induced immune response without the individual contracting the disease in question.16
With the onset of the COVID-19 pandemic, research into the determinants of vaccine hesitancy has become one of the priority issues in public health.17
In this context, in the first quarter of 2021, the first doses of COVID-19 vaccines (Pzifer and Astrazeneca) acquired through the COVAX program arrived in Cape Verde.18 In the same period, the process of immunizing the resident Cape Verdean population began, with the first phase targeting health professionals on the front line of the fight against the COVID-19 pandemic, followed by the population aged 60 and over and then the entire population over 18.19
Since the start of the vaccination campaign in Cape Verde, the uptake of the COVID-19 vaccine by the resident population is considered to be excellent. Epidemiological data shows that the population has adhered more to the first dose than to the other doses recommended by the WHO. According to data from the COVID-19 Vaccine Epidemiological Bulletin, by October 9, 2022, 98.6% of the eligible adult population in the country had been vaccinated with the first dose, 86.2% of the target population had been vaccinated with the second dose, and 38.0% of the resident population had received booster doses.20
Following the vaccination campaign, at the end of 2021, the campaign to vaccinate adolescents and young people aged 12–17 began and the data show that by October 9, 2022, 88.1% of adolescents had been vaccinated with the first dose and 74.6% were fully vaccinated.20 This study was conducted to determine the knowledge, attitudes, and factors associated with the uptake of the COVID-19 vaccine by the resident Cape Verdean population aims to produce scientific evidence to support the national health system in defining public policies to prevent and combat the COVID-19 pandemic, as well as to respond to the concerns, doubts, and fake news disseminated around the COVID-19 vaccine.
A study conducted in Europe14 to determine the predictors of COVID-19 vaccination attitudes through multiple waves in 7 countries geographically spread across the European continent, the results of these studies showed that perception of social norms in relation to COVID-19 vaccination was defined as the most important predictor of vaccine acceptance. In this study, the main determinants included demographic variables related to the respondent's knowledge and exposure to information.
Recent studies have reported that variables related to more general vaccination attitudes and beliefs in relation to the respondent's social norms, attitudes towards wearing masks, attitudes towards the flu vaccine, distrust of government health authorities and scientists, and the level of knowledge of existing treatments for COVID-19 determined participants' attitudes towards vaccination against COVID_19.14 Potential predictive determinants in the COVID-19 vaccine uptake decision included demographic variables related to the respondent's knowledge and exposure to information and variables related to more general vaccination attitudes and beliefs in relation to the respondent's social norms.
Data from studies on the determinants of acceptance of the COVID-19 vaccine have shown that sociodemographic variables such as age, gender, and education have influenced the acceptance of vaccination, intention to vaccinate, and recommendations for the COVID-19 vaccine. A study carried out in the USA33 showed that men, university students, and/or graduate degree holders were the groups most likely to accept being vaccinated compared to women and people with no university degree.33 Another study on vaccine hesitancy reported that people aged 25–54, 55–64, and 65+ were more likely to accept the vaccine than those aged 18–24 (29) and those with higher levels of education were also positively associated with vaccine acceptance.29
Despite the fact that the study was carried out in a low-income social reality, the results of this study make a valuable contribution to national health authorities and the international scientific community, allowing a better understanding of the knowledge and attitudes of the general population towards the COVID-19 vaccine, allowing the development of general strategies to combat hesitation and increase multinational confidence in the COVID-19 vaccine.
MethodsStudy designAn observational, cross-sectional, and descriptive study was conducted by the National Institute of Public Health from March 9 to 15, 2021. The survey universe was made up of data on individuals residing at national level, according to data from the National Statistics Institute.
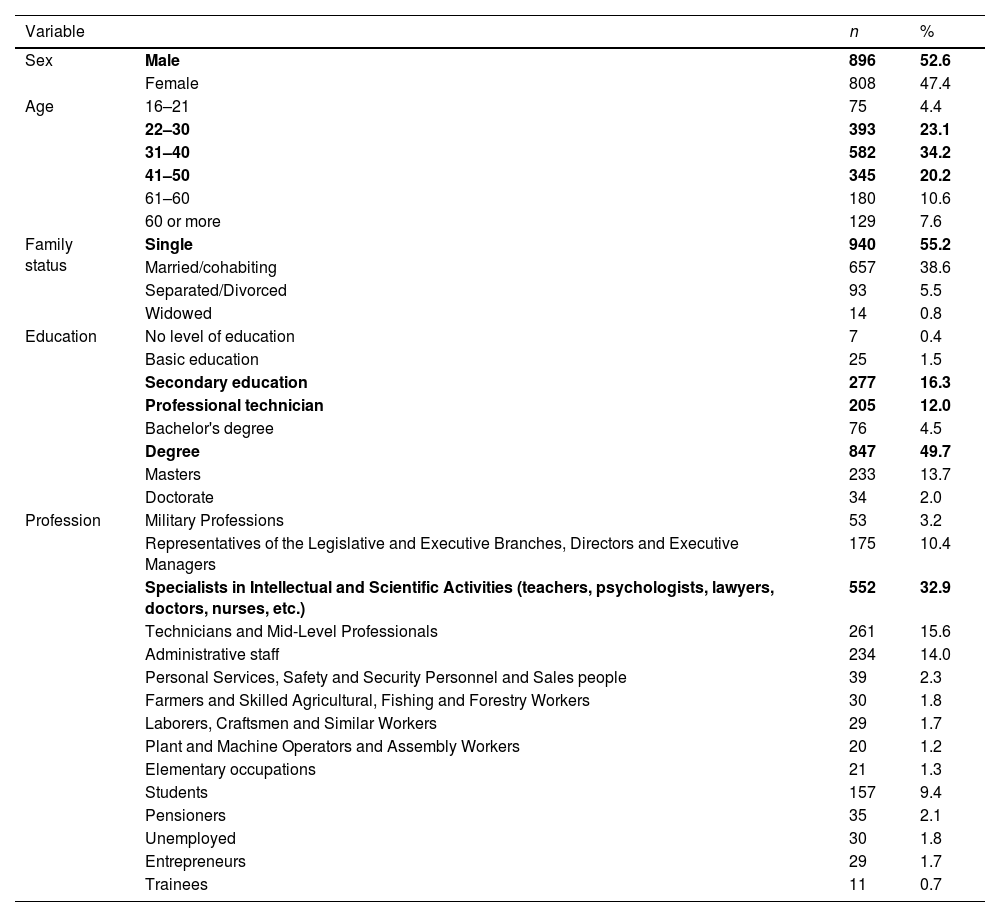
PopulationA study involving 1704 citizens living in the archipelago of Cape Verde, whose ages ranged from 16 to 60. The majority (52.6%) of the participants were male, single (55.2%), and lived on the island of Santiago (72.7%). The most prevalent age group was 31–40 years old (34.2%). Graduates were the most frequently represented by the participants (49.7%) and specialists in intellectual and scientific activities (32.9%) were the main professional activity of the study subjects according to the sociodemographic data (Table 1).
Sociodemographic data.
| Variable | n | % | |
|---|---|---|---|
| Sex | Male | 896 | 52.6 |
| Female | 808 | 47.4 | |
| Age | 16–21 | 75 | 4.4 |
| 22–30 | 393 | 23.1 | |
| 31–40 | 582 | 34.2 | |
| 41–50 | 345 | 20.2 | |
| 61–60 | 180 | 10.6 | |
| 60 or more | 129 | 7.6 | |
| Family status | Single | 940 | 55.2 |
| Married/cohabiting | 657 | 38.6 | |
| Separated/Divorced | 93 | 5.5 | |
| Widowed | 14 | 0.8 | |
| Education | No level of education | 7 | 0.4 |
| Basic education | 25 | 1.5 | |
| Secondary education | 277 | 16.3 | |
| Professional technician | 205 | 12.0 | |
| Bachelor's degree | 76 | 4.5 | |
| Degree | 847 | 49.7 | |
| Masters | 233 | 13.7 | |
| Doctorate | 34 | 2.0 | |
| Profession | Military Professions | 53 | 3.2 |
| Representatives of the Legislative and Executive Branches, Directors and Executive Managers | 175 | 10.4 | |
| Specialists in Intellectual and Scientific Activities (teachers, psychologists, lawyers, doctors, nurses, etc.) | 552 | 32.9 | |
| Technicians and Mid-Level Professionals | 261 | 15.6 | |
| Administrative staff | 234 | 14.0 | |
| Personal Services, Safety and Security Personnel and Sales people | 39 | 2.3 | |
| Farmers and Skilled Agricultural, Fishing and Forestry Workers | 30 | 1.8 | |
| Laborers, Craftsmen and Similar Workers | 29 | 1.7 | |
| Plant and Machine Operators and Assembly Workers | 20 | 1.2 | |
| Elementary occupations | 21 | 1.3 | |
| Students | 157 | 9.4 | |
| Pensioners | 35 | 2.1 | |
| Unemployed | 30 | 1.8 | |
| Entrepreneurs | 29 | 1.7 | |
| Trainees | 11 | 0.7 |
The study population was chosen by non-probability convenience sampling. The Cape Verde Archipelago is a small island country with a total area of 4033 km2, made up of 10 islands and 5 islets, situated 560 km off the west coast of Senegal and made up of a group of islands to the north, the Barlavento islands, and a group of islands to the south, the Sotavento islands. The largest and most populated island is Santiago (990 km2 and 155 252 ha) and the only uninhabited island, with the smallest surface area, is Santa Luzia (35 km2).
Cape Verde is a medium-low development country with a very young population (more than 50% of the inhabitants are between 20 and 40 years old) and intense mobility of people due to its geographical and climatic characteristics. Its economy relies heavily on the tourism industry and its links with the vast and dispersed Cape Verdean diaspora.21
According to the 2020 Census, the resident population fell from 491 575 in 2010 to 483 628 inhabitants, distributed 74% in urban areas and 26% in rural areas, while men represent 50.3% of the population.21
Cape Verde's epidemiological profile, which is undergoing a transition, has a double burden of non-communicable diseases and infectious diseases. Non-communicable diseases represent the main causes of mortality in Cape Verde, the most frequent being cardiovascular and oncological diseases. Communicable diseases still need to be monitored and controlled, as they continue to have an impact on the public health of the Cape Verdean population and represent new challenges for the National Health Service.22–26
Cape Verde has made significant gains in terms of improving the health of its population in recent decades. In relation to the country's main indicators, the maternal mortality rate has tended to decrease since the 1990s, despite the fluctuations in rates in recent years, between 49.1/100 000 LB in 2010, 9.4/100 000 in 2014 and 105.1/100 000 LB in 2019, varying in absolute numbers from 5 women in 2000 to 1 in 2014 and 11 in 2019.25
In relation to the infant mortality rate over the same period, the trend is also downwards, from 22.9/‰ LB in 2010 to 20.3/‰ LB in 2014 and 15.6/‰ LB in 2019 (MS, 2021; MSSS, 2019).25
Measurement instrumentsData was collected online, on the Google form platform, using a standardized questionnaire, adapted from similar studies, subdivided into 2 parts, with the first part containing sociodemographic variables and the second part the variables of knowledge, attitudes, practices, and adherence of the resident population to the COVID-19 vaccine.
For this study, the instrument was adapted. The questionnaire was administered nationwide by trained surveyors. The results were analyzed by members of the research team. The admission criteria for this study were: citizens living in Cape Verde, over 16 years of age, and who agreed to take part in the study by signing the informed consent form and the exclusion criteria: citizens living in the country for less than 6 months, under 16 years of age, and all those who did not sign the informed consent form.
Data collectionData collection took place in March 2021, with a team of trained surveyors and supervisors. Before filling in the online questionnaire, participants were informed about the objectives and details of the study, and provided their free and informed consent online, an essential condition for accessing the study questionnaire. The participants' voluntariness and anonymity were guaranteed. The study received the assent of the National Commission for Data Protection and Ethics in Health Research, through deliberation no. 16/CNPD/2021.
Data analysisThe data collected was analyzed using the Statistical Package for the Social Sciences (v.26) and EXCELL to produce the tables. Statistics were used to calculate relative and absolute frequencies and binary logistic regression to measure the effect of sociodemographic variables and previous vaccine experience on vaccine safety, intention to vaccinate, and recommendation of the COVID-19 vaccine in the Cape Verdean population. The variables vaccine safety, intention to vaccinate, and recommending the COVID-19 vaccine were treated as dichotomous, i.e., 2 categories, yes and no, and the level of statistical significance for all tests was set at P<.05.
To build the logit model, taking into account how the model works with the categorical dependent variable and opting for the binary model (1=yes, 0=no), the dependent variables (vaccine safety, intention to vaccinate, and recommending the COVID-19 vaccine) had to be recoded as 1=success and 0=failure.
In this test, an Odds Ratio was predominantly used, comparing the analysis category with the reference category (indicated in Table 5 as reference or with an OR value=1.00). Furthermore, only the variables that had a significant effect (in a clear direction of increase or decrease at a maximum level of 5%) were highlighted and analyzed.
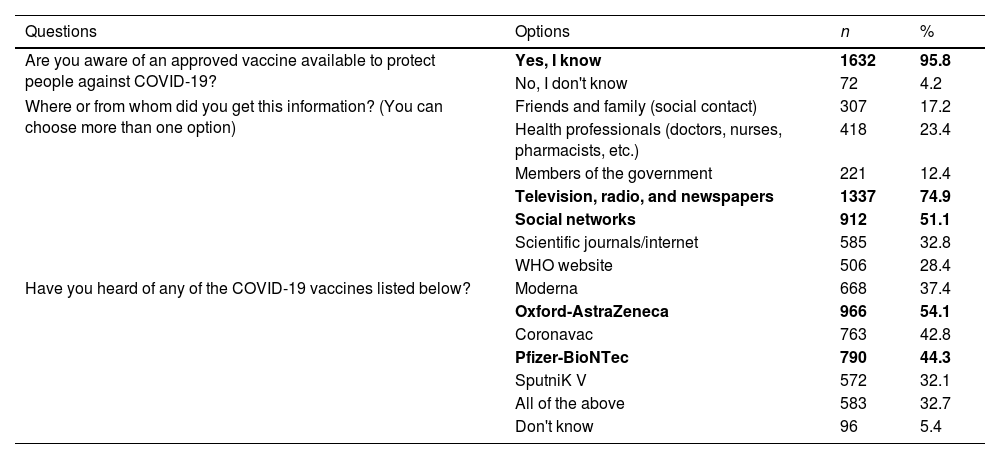
ResultsKnowledge of the Cape Verdean population about the COVID-19 vaccineThe results show that, at the time of data collection, the majority (95.8%) of participants were highly aware of the existence of an approved vaccine against COVID-19, and only 4.2% of participants were unaware of the existence of an immunizer against COVID-19. And, as for the means of acquiring this information, the majority of subjects said they had learned about it through television, radio, and newspapers (74.9%), followed by social media (51.1%). The vaccine best known at the time by the resident Cape Verdean population was AstraZeneca (54.1%), followed by Pfizer-BioNTec (44.3%) (Table 2).
Vaccine knowledge.
| Questions | Options | n | % |
|---|---|---|---|
| Are you aware of an approved vaccine available to protect people against COVID-19? | Yes, I know | 1632 | 95.8 |
| No, I don't know | 72 | 4.2 | |
| Where or from whom did you get this information? (You can choose more than one option) | Friends and family (social contact) | 307 | 17.2 |
| Health professionals (doctors, nurses, pharmacists, etc.) | 418 | 23.4 | |
| Members of the government | 221 | 12.4 | |
| Television, radio, and newspapers | 1337 | 74.9 | |
| Social networks | 912 | 51.1 | |
| Scientific journals/internet | 585 | 32.8 | |
| WHO website | 506 | 28.4 | |
| Have you heard of any of the COVID-19 vaccines listed below? | Moderna | 668 | 37.4 |
| Oxford-AstraZeneca | 966 | 54.1 | |
| Coronavac | 763 | 42.8 | |
| Pfizer-BioNTec | 790 | 44.3 | |
| SputniK V | 572 | 32.1 | |
| All of the above | 583 | 32.7 | |
| Don't know | 96 | 5.4 |
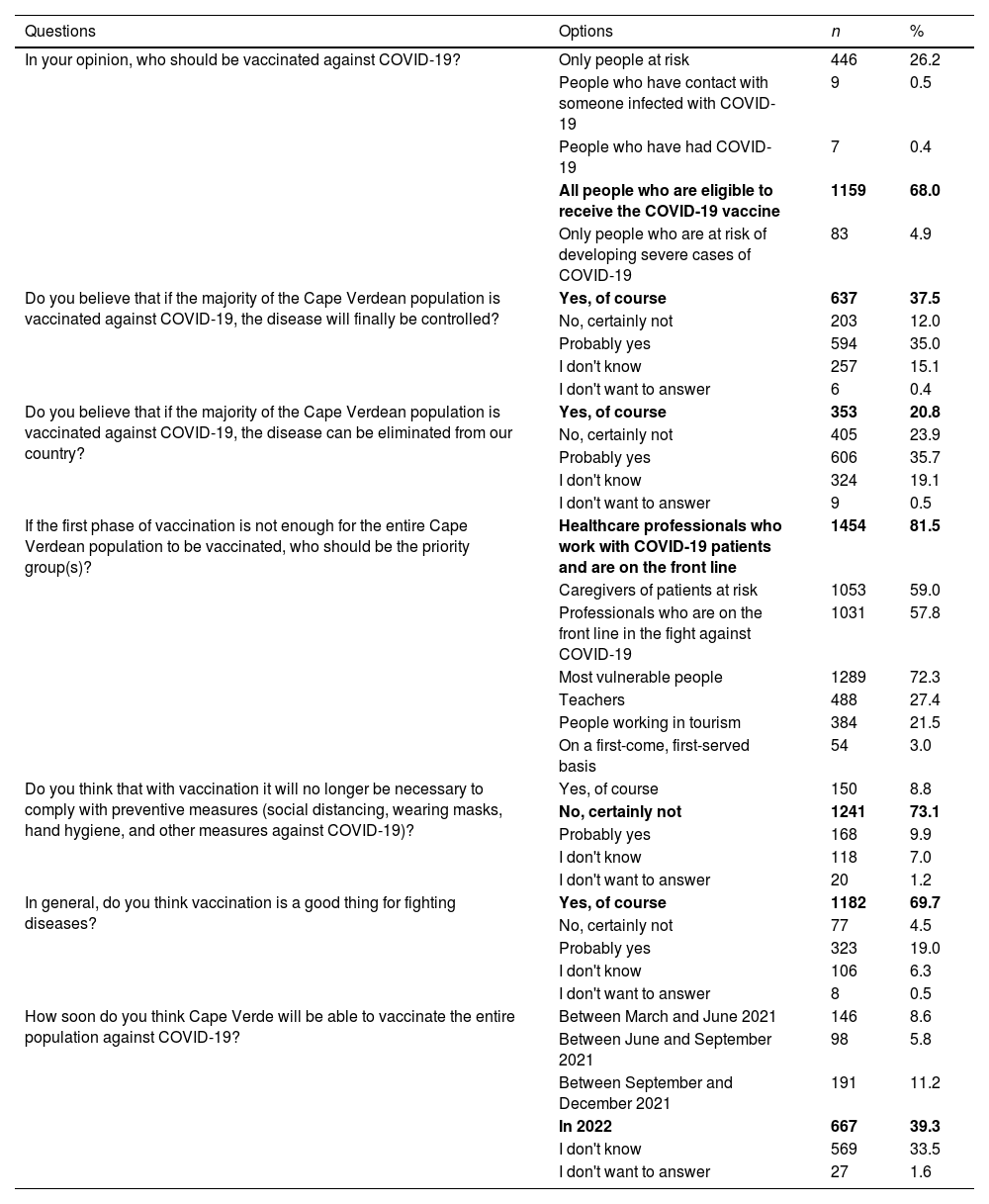
At the time of data collection, Cape Verdean residents were in favor of vaccination against COVID-19. That is, 68.0% of the participants thought that all eligible people should be vaccinated against COVID-19, 37.5% of the subjects were confident that if the majority of the Cape Verdean population got vaccinated, the pandemic could be controlled, and 20.8% of the participants believed that it could even be eliminated from the country. The majority of participants (81.5%) considered that the priority groups for vaccination should be health professionals, followed by the most vulnerable (the elderly and people with chronic illnesses) (72.3%). For the majority of participants (73.1%), after mass vaccination of the population, there would no longer be any need to continue with restrictive measures (wearing a mask, social distancing, and respiratory etiquette). The majority of subjects (69.7%) were of the opinion that vaccination was an effective measure to end the COVID-19 pandemic in Cape Verde. Finally, 39.3% of respondents believed that by the end of 2022, Cape Verde would have the necessary conditions to vaccinate the entire resident population against COVID-19 (Table 3).
Attitudes towards vaccination.
| Questions | Options | n | % |
|---|---|---|---|
| In your opinion, who should be vaccinated against COVID-19? | Only people at risk | 446 | 26.2 |
| People who have contact with someone infected with COVID-19 | 9 | 0.5 | |
| People who have had COVID-19 | 7 | 0.4 | |
| All people who are eligible to receive the COVID-19 vaccine | 1159 | 68.0 | |
| Only people who are at risk of developing severe cases of COVID-19 | 83 | 4.9 | |
| Do you believe that if the majority of the Cape Verdean population is vaccinated against COVID-19, the disease will finally be controlled? | Yes, of course | 637 | 37.5 |
| No, certainly not | 203 | 12.0 | |
| Probably yes | 594 | 35.0 | |
| I don't know | 257 | 15.1 | |
| I don't want to answer | 6 | 0.4 | |
| Do you believe that if the majority of the Cape Verdean population is vaccinated against COVID-19, the disease can be eliminated from our country? | Yes, of course | 353 | 20.8 |
| No, certainly not | 405 | 23.9 | |
| Probably yes | 606 | 35.7 | |
| I don't know | 324 | 19.1 | |
| I don't want to answer | 9 | 0.5 | |
| If the first phase of vaccination is not enough for the entire Cape Verdean population to be vaccinated, who should be the priority group(s)? | Healthcare professionals who work with COVID-19 patients and are on the front line | 1454 | 81.5 |
| Caregivers of patients at risk | 1053 | 59.0 | |
| Professionals who are on the front line in the fight against COVID-19 | 1031 | 57.8 | |
| Most vulnerable people | 1289 | 72.3 | |
| Teachers | 488 | 27.4 | |
| People working in tourism | 384 | 21.5 | |
| On a first-come, first-served basis | 54 | 3.0 | |
| Do you think that with vaccination it will no longer be necessary to comply with preventive measures (social distancing, wearing masks, hand hygiene, and other measures against COVID-19)? | Yes, of course | 150 | 8.8 |
| No, certainly not | 1241 | 73.1 | |
| Probably yes | 168 | 9.9 | |
| I don't know | 118 | 7.0 | |
| I don't want to answer | 20 | 1.2 | |
| In general, do you think vaccination is a good thing for fighting diseases? | Yes, of course | 1182 | 69.7 |
| No, certainly not | 77 | 4.5 | |
| Probably yes | 323 | 19.0 | |
| I don't know | 106 | 6.3 | |
| I don't want to answer | 8 | 0.5 | |
| How soon do you think Cape Verde will be able to vaccinate the entire population against COVID-19? | Between March and June 2021 | 146 | 8.6 |
| Between June and September 2021 | 98 | 5.8 | |
| Between September and December 2021 | 191 | 11.2 | |
| In 2022 | 667 | 39.3 | |
| I don't know | 569 | 33.5 | |
| I don't want to answer | 27 | 1.6 |
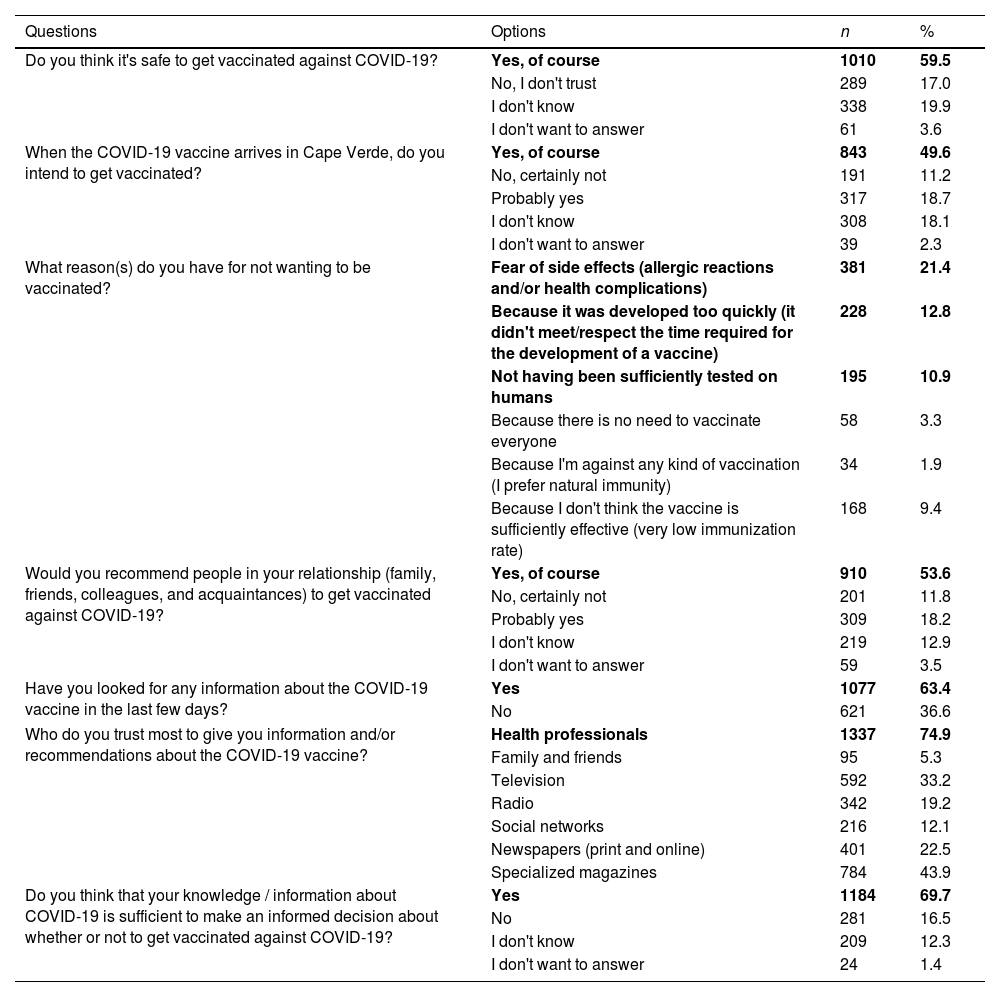
The majority (59.5%) of the subjects said that it was safe to get vaccinated against COVID-19, while 17% of the participants showed no confidence in the COVID-19 vaccine. Regarding the intention to get vaccinated, almost half (49.6%) of the respondents intended to get vaccinated when the vaccine arrived in Cape Verde and only 11.2% said they had no intention of getting vaccinated. The main reasons why participants were hesitant to get vaccinated were: fear of side effects (21.4%), the minimum time needed to develop a vaccine had not been met/respected (12.8%), the vaccine had not been sufficiently tested on humans (10.9%), and they did not believe in the efficacy of vaccines (9.4%).
On the other hand, 53.6% of participants would recommend the COVID-19 vaccine to their loved ones. The majority of participants (63.4%) had sought some kind of information about the vaccine in the last few days, trusted health professionals as the safest way to receive any information about the COVID-19 vaccine (74.9%), and were of the opinion that the knowledge/information they had at the time was sufficient for them to make an informed decision about whether to get vaccinated against COVID-19 (69.7%) (Table 4).
Population for or against vaccination.
| Questions | Options | n | % |
|---|---|---|---|
| Do you think it's safe to get vaccinated against COVID-19? | Yes, of course | 1010 | 59.5 |
| No, I don't trust | 289 | 17.0 | |
| I don't know | 338 | 19.9 | |
| I don't want to answer | 61 | 3.6 | |
| When the COVID-19 vaccine arrives in Cape Verde, do you intend to get vaccinated? | Yes, of course | 843 | 49.6 |
| No, certainly not | 191 | 11.2 | |
| Probably yes | 317 | 18.7 | |
| I don't know | 308 | 18.1 | |
| I don't want to answer | 39 | 2.3 | |
| What reason(s) do you have for not wanting to be vaccinated? | Fear of side effects (allergic reactions and/or health complications) | 381 | 21.4 |
| Because it was developed too quickly (it didn't meet/respect the time required for the development of a vaccine) | 228 | 12.8 | |
| Not having been sufficiently tested on humans | 195 | 10.9 | |
| Because there is no need to vaccinate everyone | 58 | 3.3 | |
| Because I'm against any kind of vaccination (I prefer natural immunity) | 34 | 1.9 | |
| Because I don't think the vaccine is sufficiently effective (very low immunization rate) | 168 | 9.4 | |
| Would you recommend people in your relationship (family, friends, colleagues, and acquaintances) to get vaccinated against COVID-19? | Yes, of course | 910 | 53.6 |
| No, certainly not | 201 | 11.8 | |
| Probably yes | 309 | 18.2 | |
| I don't know | 219 | 12.9 | |
| I don't want to answer | 59 | 3.5 | |
| Have you looked for any information about the COVID-19 vaccine in the last few days? | Yes | 1077 | 63.4 |
| No | 621 | 36.6 | |
| Who do you trust most to give you information and/or recommendations about the COVID-19 vaccine? | Health professionals | 1337 | 74.9 |
| Family and friends | 95 | 5.3 | |
| Television | 592 | 33.2 | |
| Radio | 342 | 19.2 | |
| Social networks | 216 | 12.1 | |
| Newspapers (print and online) | 401 | 22.5 | |
| Specialized magazines | 784 | 43.9 | |
| Do you think that your knowledge / information about COVID-19 is sufficient to make an informed decision about whether or not to get vaccinated against COVID-19? | Yes | 1184 | 69.7 |
| No | 281 | 16.5 | |
| I don't know | 209 | 12.3 | |
| I don't want to answer | 24 | 1.4 |
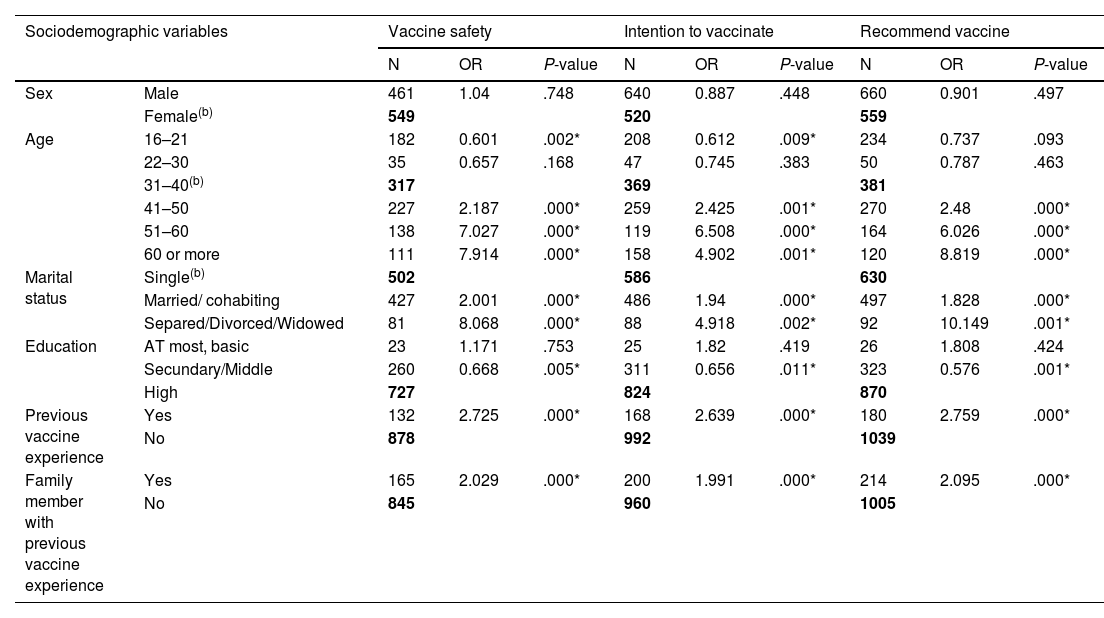
The data from this study show that, according to the level of significance taken in this study, there is no statistically significant difference between the sexes in relation to COVID-19 vaccine safety. In terms of age group, respondents aged 41–50, 51–60, and 60 and over were 2.27 and 7.9 times safer, respectively, when compared to respondents aged 31–40 (P<.05). Meanwhile, respondents in the 16–21 age group reported being less safe with the COVID-19 vaccine (OR=0.601).
With regard to marital status, married or cohabiting and separated/divorced and widowed respondents were 2.0 and 8.1 times more likely to be vaccinated against COVID-19, respectively, when compared to single respondents (P<.05).
Regarding education, the results indicated that respondents with secondary/middle school education had less confidence in the vaccine (OR = 0.668), when compared to respondents with higher education (P<.05). Regarding previous vaccine experience, respondents with previous vaccine experience are 2.7 times safer with the COVID-19 vaccine when compared to individuals with no previous vaccine experience (P<.05).
Regarding situations where family members have previous vaccine experience: respondents whose family members have previous vaccine experience are 2 times safer with the COVID-19 vaccine when compared to individuals with no previous vaccine experience (P<.05).
Determinants of the intention to vaccinate against COVID-19Regarding the determinants of the intention to vaccinate on sociodemographic data, the variable Gender, and depending on the level of significance taken in this study, there is no statistically significant difference between the sexes and the respondents' intention to vaccinate against COVID-19. In terms of age group, respondents aged 41–50, 51–60, and 60 and over were 2.4, 6.5, and 4.9 times more likely to be vaccinated against COVID-19, respectively, when compared to respondents aged 31–40 (P<.05). Meanwhile, respondents in the 16–21 age group have fewer intentions to get vaccinated against COVID-19 (OR=0.612).
With regard to marital status, married or cohabiting respondents and separated/divorced and widowed respondents showed, respectively, 1.9 and 4.9 times more willingness to be vaccinated against COVID-19 when compared to single respondents (P<.05).
In terms of education, respondents with secondary/middle school education have fewer intentions to get vaccinated (OR=0.656), when compared to respondents with higher education (P<.05).
Regarding previous vaccine experience, respondents with previous experience of other vaccines were 2.6 times more likely to be vaccinated against COVID-19 when compared to individuals with no previous experience of any vaccine (P<.05).
Regarding the relationship between family members and previous vaccine experience, respondents whose family members had previous experience of any vaccine were 2.0 times more likely to be vaccinated against COVID-19 when compared to those with no previous vaccine experience (P<.05).
Determinants of indicating the COVID-19 vaccineRegarding the influence of sociodemographic variables on the determinant of indicating the COVID-19 vaccine, according to the significance level of this study, the gender variable did not show a statistically significant difference in relation to the determinant of indicating the COVID-19 vaccine.
With regard to age group, respondents aged 41–50, 51–60, and 60 and over were 2.4, 6, and 8.8 times more likely to recommend the COVID-19 vaccine, respectively, when compared to respondents aged 31–40 (P<.05).
Regarding marital status, married or cohabiting respondents and separated/divorced and widowed respondents were respectively 1.8 and 10.2 times more likely to suggest the COVID-19 vaccine when compared to single respondents (P<.05).
Regarding education, respondents with secondary/middle school education were less likely to recommend the COVID-19 vaccine (OR=0.676), when compared to respondents with higher education (P<.05).
Regarding previous experience with vaccines: respondents with previous experience with vaccines were 2.8 times more likely to recommend the COVID-19 vaccine when compared to individuals with no previous experience with vaccines (P<.05).
Family experience with vaccines: respondents whose family members had previous experience with vaccines were 2 times more likely to recommend the COVID-19 vaccine when compared to individuals with no previous experience with vaccines (P<.05), according to the data presented in Table 5.
Binary logistic regression to measure the effect of sociodemographic variables on vaccine safety, intention to vaccinate, and recommendation of the COVID-19 vaccine in the Cape Verdean population, 2020.
| Sociodemographic variables | Vaccine safety | Intention to vaccinate | Recommend vaccine | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | OR | P-value | N | OR | P-value | N | OR | P-value | ||
| Sex | Male | 461 | 1.04 | .748 | 640 | 0.887 | .448 | 660 | 0.901 | .497 |
| Female(b) | 549 | 520 | 559 | |||||||
| Age | 16–21 | 182 | 0.601 | .002* | 208 | 0.612 | .009* | 234 | 0.737 | .093 |
| 22–30 | 35 | 0.657 | .168 | 47 | 0.745 | .383 | 50 | 0.787 | .463 | |
| 31–40(b) | 317 | 369 | 381 | |||||||
| 41–50 | 227 | 2.187 | .000* | 259 | 2.425 | .001* | 270 | 2.48 | .000* | |
| 51–60 | 138 | 7.027 | .000* | 119 | 6.508 | .000* | 164 | 6.026 | .000* | |
| 60 or more | 111 | 7.914 | .000* | 158 | 4.902 | .001* | 120 | 8.819 | .000* | |
| Marital status | Single(b) | 502 | 586 | 630 | ||||||
| Married/ cohabiting | 427 | 2.001 | .000* | 486 | 1.94 | .000* | 497 | 1.828 | .000* | |
| Separed/Divorced/Widowed | 81 | 8.068 | .000* | 88 | 4.918 | .002* | 92 | 10.149 | .001* | |
| Education | AT most, basic | 23 | 1.171 | .753 | 25 | 1.82 | .419 | 26 | 1.808 | .424 |
| Secundary/Middle | 260 | 0.668 | .005* | 311 | 0.656 | .011* | 323 | 0.576 | .001* | |
| High | 727 | 824 | 870 | |||||||
| Previous vaccine experience | Yes | 132 | 2.725 | .000* | 168 | 2.639 | .000* | 180 | 2.759 | .000* |
| No | 878 | 992 | 1039 | |||||||
| Family member with previous vaccine experience | Yes | 165 | 2.029 | .000* | 200 | 1.991 | .000* | 214 | 2.095 | .000* |
| No | 845 | 960 | 1005 | |||||||
(b) - base or reference category; * - P<.05.
Vaccination is considered to be one of the most cost-effective ways of preventing disease. Currently, it is estimated that vaccination prevents 2–3 million deaths a year and that a further 1.5 million diseases could be avoided if global coverage of available vaccines improved.9 The emergence of COVID-19 and the accelerated knowledge of the virus and the disease have enabled the development of effective and safe vaccines in a short space of time.
The results of this study showed that the majority (68.0%) of respondents were in favor of administering the COVID-19 vaccine to all eligible people. These data indicate that the resident Cape Verdean population has been attentive to the mechanisms for developing the vaccine and the movement set in motion by the international scientific community to put an end to the COVID-19 pandemic.
The data indicate a prevalence of 29.3% of subjects hesitating to be vaccinated against COVID-19. Similar results were found in studies carried out in Europe, America, and Asia, where there was also a significant prevalence of vaccine hesitancy against COVID-19.18 A survey with a random sample of 13 426 people from 19 countries (whose combined populations account for 55% of the world's population) found a prevalence of hesitancy of 28.5%, ranging from 11.4% in China to 45.1% in Russia.27,28
The data from this study shows that Brazil had the second lowest estimated prevalence in this study (14.7%), which is also lower than other middle-income countries evaluated, such as India, Mexico, and South Africa.27,29 Turkey had similar data, with a prevalence of vaccine hesitancy of 14.0%.30 And, other studies carried out in Europe and America provide indices of the rate of vaccine hesitancy in the population, with the UK showing a hesitancy rate of 31.0% and the USA 42.4%.30,31
In summary, studies show that, globally, it is estimated that vaccine hesitancy against COVID-19 is 25.0% in the general population, 22.0% in doctors, and 39.0% among nurses.27,29
In this study, the biggest reasons for hesitating to get vaccinated against COVID-19 were related to fear of side effects, followed by distrust of the vaccine's efficacy. These results corroborate a study carried out in China in March 2020, where 58.3% of respondents wanted to be vaccinated immediately, but the proportion fell to 23.0% in November–December 2020, due to the fact that respondents decided to postpone vaccination until its safety was guaranteed.32
Despite these data, in the present study on the knowledge, attitudes, and adherence of the Cape Verdean population to the COVID-19 vaccine, the majority of participants (53.6%) stated that they would recommend the COVID-19 vaccine to people in their relationships. In this study, predictors of vaccine safety, intention to vaccinate, and vaccine recommendation were age group, marital status, schooling, previous vaccine experience, and family members with previous vaccine experience. Individuals over 40 years of age, married, and divorced individuals, those with higher education, with vaccine experience, or family members with previous vaccine experience showed greater vaccine safety, as well as greater intention to vaccinate and vaccine recommendation (P<.005).
The results of a study on the determinants of acceptance of the COVID-19 vaccine in the USA showed that acceptance of vaccination varied by sociodemographic characteristics, with men more confident (72%) than women, adults over 55 (78%) compared to young people, Asians (81%) compared to other racial and ethnic groups, and university and/or graduate degree holders (75%) compared to people with less than a university degree being the groups most likely to accept being vaccinated.33 In this study, the respondents most likely to be vaccinated with the COVID-19 vaccine were those aged over 40, married/married in a de facto union, separated/divorced, widowed, and those with higher education.
Study subjects who had already been vaccinated against some type of disease (yellow fever, measles, tuberculosis, and hepatitis) showed greater certainty in the safety of the COVID-19 vaccine. They were the ones who most reported the intention to be vaccinated and presented higher percentages of vaccine recommendations to people in their relationships and, equally, were those who defended that the vaccine should be mandatory for the entire Cape Verdean resident population.
Regarding Cape Verdeans' confidence in vaccines (59.5%), they believed that the COVD-19 vaccine is safe and 49.6% intended to get vaccinated when the vaccine was available to the resident population. These data demonstrate a positive attitude of the resident Cape Verdean population towards adherence to the COVID-19 vaccine.
However, respondents in the 16–21 age group, singles, and those with secondary/secondary education were the group with the highest COVID-19 vaccine hesitancy (the refusal/I don't trust). These sections of the population should deserve special attention from education and awareness strategies to ensure widespread vaccination.
ConclusionsThe data of the present study allowed to know the attitudes, practices, and adherence of the Cape Verdean resident population in relation to the vaccine against COVID-19. Data collected days before the start of the national COVID-19 vaccination campaign in Cape Verde showed that at the time of data collection, study participants were optimistic about the vaccine's effectiveness in combating the COVID-19 pandemic. Similarly, participants were available to get vaccinated against COVID-19.
In summary, the present study brings credible scientific evidence about the knowledge, attitudes, and adherence of the resident Cape Verdean population about the COVID-19 vaccine. The results demonstrate that the success of the control of the COVID-19 pandemic at the local and global level depends on the combination of a set of actions, including the cooperation of the population in adhering to the vaccination campaign, as one of the safety measures recommended by the international scientific community for the prevention of the disease.
Finally, the results of the current study demonstrate, once again, the capacity, resilience, and perseverance of Cape Verdeans in the fight for local and universal causes. The proactive attitudes of the local population, the trust placed in the vaccine as a means of combating the COVID-19 pandemic and the active search for information about the vaccine, as well as the trust placed in the professionals are indicators of the positive result of the present study.
Notwithstanding these results, the data from this study suggest the mobilization of the active participation of the resident Cape Verdean population in adherence to the recommended doses of vaccination against COVID-19. Awareness, education, and information campaigns about the vaccine are key to controlling the hesitancy and fake news disseminated against the COVID-19 vaccine.
LimitationsAlthough the results of these studies are favorable, they should be taken with caution due to due to the fact that it is a convenience survey, online, limited only to the population with internet access, and not representative of the total population. The people with low digital literacy may have been left out. In this sense, and due to this limitation, the data from this study cannot be generalized to the entire Cape Verdean population.