




The Law for the Regulation of Health Professions (LOPS) indicates that health professionals will carry out continuous training throughout their professional life, and will regularly prove their professional competence. The objective of the study was to carry out a national survey to find out the opinion of Spanish surgeons and thus be able to prepare a recertification project by the Spanish Association of Surgeons.
MethodsCross-sectional observational study carried out in June–July 2020, through a survey sent to the members of the Spanish Association of Surgeons.
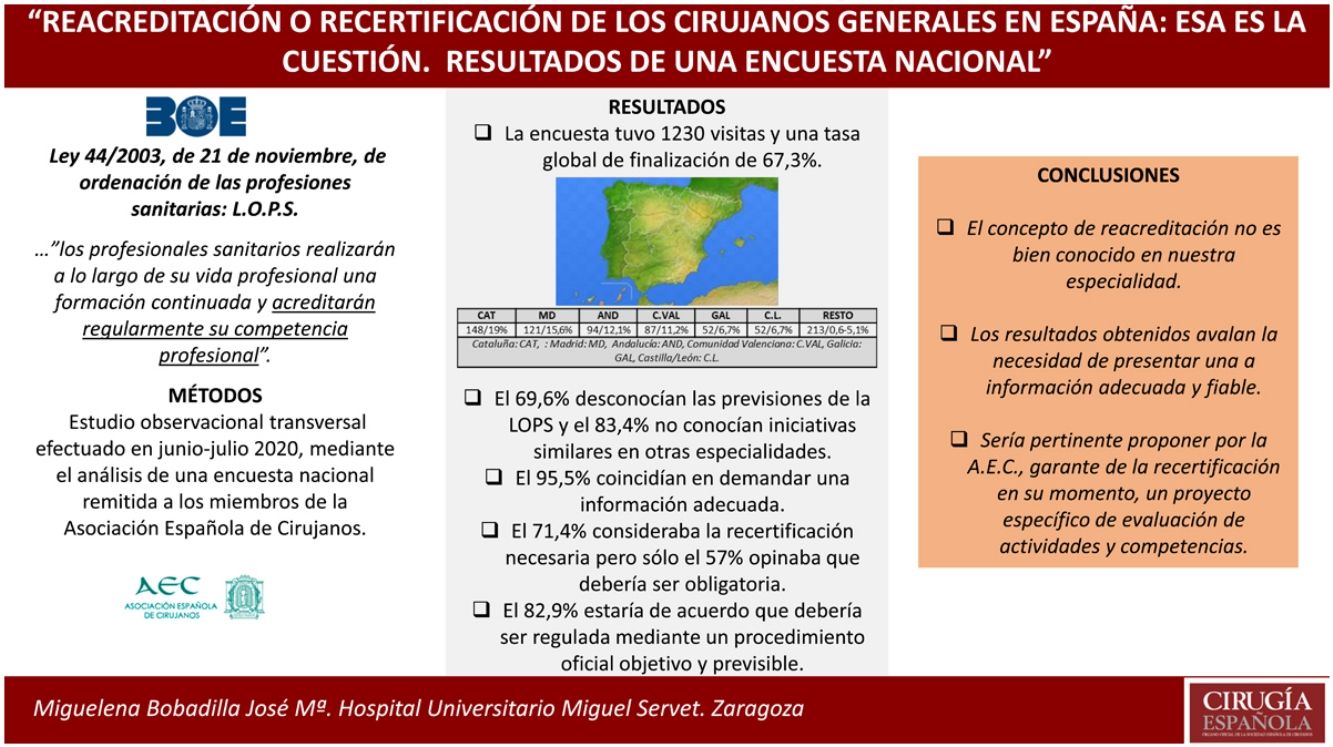
ResultsThe survey had a total of 1230 visits and an overall completion rate of 784 responses (67.3%). 69.6% were unaware of the LOPS forecasts and 83.4% were unaware of similar initiatives in other specialties and 95.5% agreed to demand adequate information. 71.4% believed it necessary but only 57% believed that it should be mandatory. 82.9% would agree that it should be regulated through an objective and predictable official procedure.
ConclusionsThe concept of re-accreditation is not well known in our specialty and in view of the results obtained, adequate and reliable information seems necessary. Therefore, it would be pertinent to propose by the A.E.C. a specific project to assess activities and skills.
La Ley de Ordenación de las Profesiones Sanitarias (LOPS) indica que los profesionales sanitarios realizarán a lo largo de su vida profesional una formación continuada, y acreditarán regularmente su competencia profesional. El objetivo del estudio ha sido realizar una encuesta nacional para conocer la opinión de los cirujanos españoles y así poder preparar un proyecto de recertificación por la Asociación Española de Cirujanos.
MétodosEstudio observacional transversal efectuado en junio-julio 2020, a través de una encuesta remitida a los miembros de la Asociación Española de Cirujanos.
ResultadosLa encuesta tuvo un total de visitas de 1230 y una tasa global de finalización de 784 respuestas (67,3%). El 69,6% desconocían las previsiones de la LOPS y el 83,4% no conocían iniciativas similares en otras especialidades y el 95,5% coincidían en demandar una información adecuada. El 71,4% la creía necesaria pero sólo el 57% opinaba que debería ser obligatoria. El 82,9% estaría de acuerdo que debería ser regulada mediante un procedimiento oficial objetivo y previsible.
ConclusionesEl concepto de reacreditación no es bien conocido en nuestra especialidad y en vista de los resultados obtenidos parece necesaria una información adecuada y fiable. Por ello sería pertinente proponer por la A.E.C. un proyecto específico de evaluación de actividades y competencias.
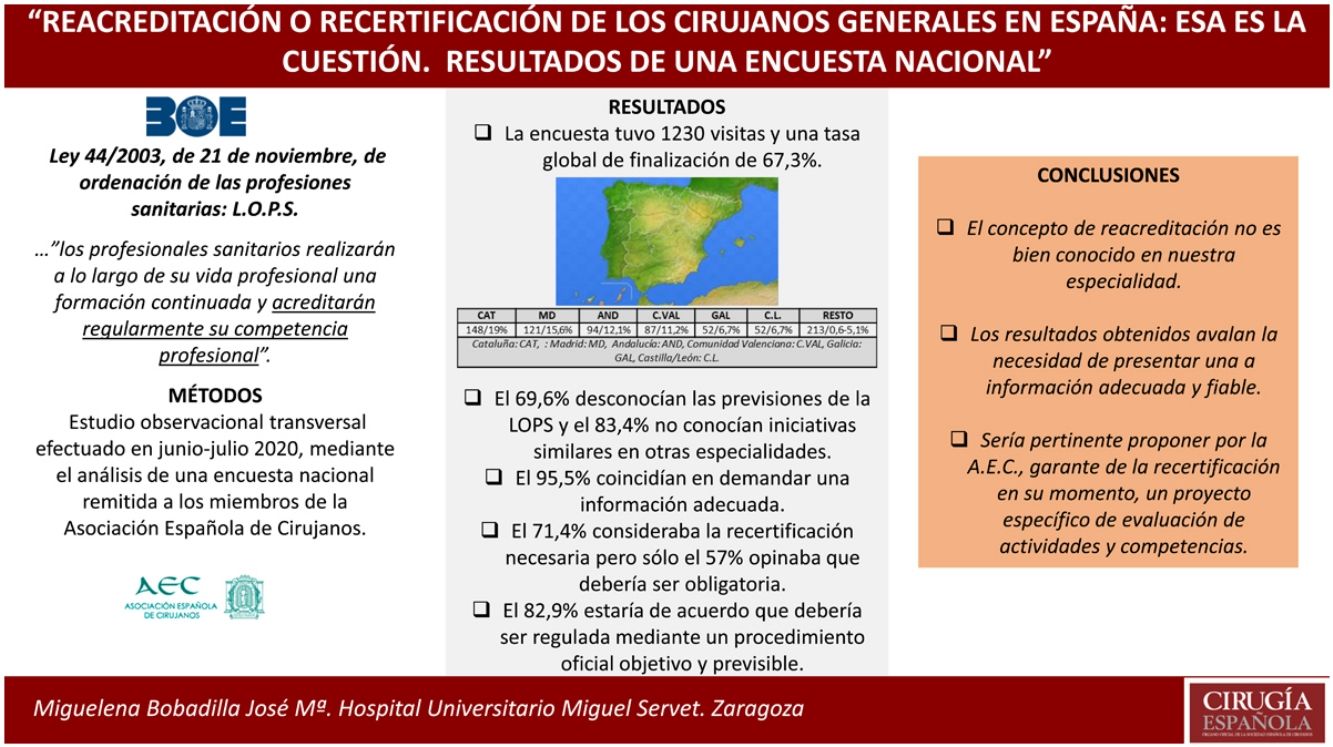
The Spanish Law for the Regulation of Healthcare Professions (Ley de Ordenación de las Profesiones Sanitarias, or LOPS)1 indicates in Article 4 that “…healthcare professionals shall carry out continuing professional development (CPD) throughout their professional careers and accredit their professional competence on a regular basis.” It defines continuous training as “…the process of teaching and learning, both active and permanent, to which healthcare professionals have the right and are obligated to comply with, which is aimed at updating and improving their knowledge, skills, and approaches in the context of scientific and technological evolution, demands and needs, both social as well as those of the healthcare system itself.”
It also defines ‘continuing professional development’ (CPD)1 as “…all those activities aimed at maintaining, updating, developing and improving the knowledge, skills and aptitudes of doctors in response to the needs of their patients,” which is understood as the process by which doctors maintain and improve their degree of competence, inherent to medical practice. It is characterized by being independent and applying self-learning in all activities, and it does not include supervised training in many instances. In this context, the concept of recertification emerges as a fundamental element of the regulatory framework of the medical profession, not only in our country, but also in most developed Western countries.
The analysis of training needs and the way to organize their provision are the duty of national/regional accreditation bodies of each Member State of the European Union, which must define the credits for Continuing Medical Education (CME) and the required curricula for a certain period of time2,3. In this context, and in order to homogenize criteria for calculating training credits, the European Union of Medical Specialists (UEMS) introduced a credit system (European Continuing Medical Education Credits [ECMEC]) in the year 2000 to facilitate the process4.
In Spain, the Spanish Continuing Medical Education Accreditation System (Sistema Español de Acreditación de Formación Médica Continuada, or SEAFORMEC) is a national organization that has an accreditation system for continuing education activities with criteria similar to those of the National Healthcare System. It is integrated into the UEMS accreditation system, having also established collaboration agreements with the Accreditation Council for Continuing Medical Education (ACCME)5 and the American Medical Association (AMA). There are also accreditation commissions in the autonomous communities of Spain for recognizing training activities at all levels6.
In this scenario, the Spanish Association of Surgeons (AEC) cannot forfeit its leading role and involvement in the CME and in the CPD of surgeons. The AEC must be prepared to develop a specific reaccreditation procedure, as stipulated by law1. This must be accessible to the diversity of surgeons who carry out their work at different levels and in different areas of our country. This process should include the number of credits required, as well as the method of obtaining them, their equivalencies and their frequency over time.
The objective of our study was to bring attention to the issue and conduct a survey7 to determine the opinion of Spanish surgeons on the subject and thus be able to inform the AEC in order to propose an adequate recertification project for Spanish surgeons who may voluntarily request it. Said project should be based on a rigorous and justified analysis of the clinical, educational and research requirements inherent to the maintenance of correct and current professional practice and would establish the procedure and assessment of the CPD of the applicant.
MethodsWe have conducted a cross-sectional observational study adapted to the criteria of the Declaration of Helsinki and following the STROBE guidelines for cross-sectional observational studies. The study was carried out through a survey sent electronically (personal email) to the members of the AEC. This survey was available online from June 12, 2020 to July 31, 2020 through the company Im3dia Comunicación, which recorded the results obtained from all the surveys and carried out the initial descriptive study. The surveys were blind, with no knowledge of the results of other participants.
The questions posed, or study variables, were of two types: a) demographic variables: gender, age, number of hospital beds, teaching hospital (Spanish MIR residency program), autonomous community (region) where the hospital is located, professional category (attending, head of unit/division/service, etc); and b) specific variables: 1.) Do you think reaccreditation/recertification is necessary in our specialty?; 2) Do you know about the pertinent legislation (Law for the Regulation of Healthcare Professions [LOPS])?; 3) Do you think healthcare professionals should be properly informed?; 4) Do you think there should be an ‘official’ procedure that is simple to complete, with objective, organized assessment?; 5) Do you think it should be mandatory?; 6) Do you think it could be associated with the periodic validation of medical associations?; 7) Do you know of similar initiatives in our country in other specialties?
Statistical analysisThe SPSS program (version 23) was used to carry out the statistical analysis. All the variables analyzed were categorical and have been described in absolute numbers and percentages.
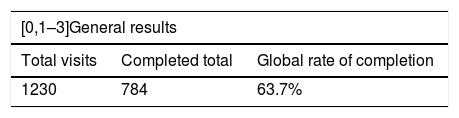
ResultsThe general results of the survey are described in Table 1. A total of 1230 online visits were registered, and a total of 784 surveys were completed (67.3%). A priori, this participation rate is higher than rates obtained by previous surveys. No significant differences were observed in terms of participant age. The age range of 31–60 years represented 79% of the participants, while 60% of those who responded to the survey were men.
Summary of the data/general results of the survey.
| [0,1–3]General results | ||
|---|---|---|
| Total visits | Completed total | Global rate of completion |
| 1230 | 784 | 63.7% |
| [0,1–5]Age, years | [0,6–7]Sex | |||||
|---|---|---|---|---|---|---|
| <30 | 31–40 | 41–50 | 51–60 | <61 | Male | Female |
| 47/6% | 202/25.8% | 161/20.6% | 257/32.9% | 115/14.7% | 470/60.1% | 312/39.9% |
| [0,1–3]Position | [0,4–7]Hospital beds (n) | |||||
|---|---|---|---|---|---|---|
| Attending/FEA | Head of Unit | Head of Department | <200 | 201–500 | 501–1000 | >1000 |
| 530/67.8% | 115/14.7% | 74/9.5% | 166 | 283 | 239 | 94 |
| [0,1–7]Autonomous communities | ||||||
|---|---|---|---|---|---|---|
| CAT | MD | AND | VAL | GAL | C.L. | Remainder |
| 148/19% | 121/15.6% | 94/12.1% | 87/11.2% | 52/6.7% | 52/6.7% | 213/0.6%–5.1% |
AND: Andalusia; CAT: Catalonia; C.L.: Castilla-Leon; VAL: Valencia; GAL: Galicia; MD: Madrid.
Regarding the hospital sizes of the surgeons surveyed, a generally homogeneous distribution was observed in terms of the hospital type and number of beds, with only a somewhat lower participation in hospitals with more than 1000 beds. The involvement of specialists (attendings, FEA) was also notably higher (67.8%) compared to unit heads (14.75%) and department heads (9.5%).
Similar to other surveys of these characteristics, the regions of Spain with the largest populations and/or the largest number of hospitals were the most widely represented, especially by participating surgeons from Catalonia (19%), Madrid (15.6%), Andalusia (12.1%) and the Valencian Community (11.2%).
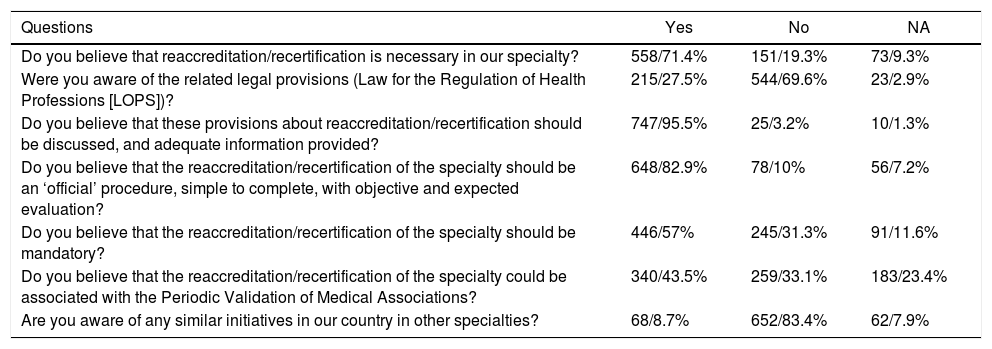
The results of the responses to the specific questions of the survey are shown in Table 2. These were generic ‘clarifiers’, and, as could be foreseen, 544 (69.6%) of the respondents were unaware of the LOPS provisions on this subject. A total of 747 of the respondents (95.5%) agreed that surgeons should be properly informed. Regardless, what is most important is that 558 (71.4%) believed that reaccreditation of the specialty was necessary, and 652 (83.4%) stated that they were not aware of similar initiatives in our country in other specialties.
Specific survey results.
| Questions | Yes | No | NA |
|---|---|---|---|
| Do you believe that reaccreditation/recertification is necessary in our specialty? | 558/71.4% | 151/19.3% | 73/9.3% |
| Were you aware of the related legal provisions (Law for the Regulation of Health Professions [LOPS])? | 215/27.5% | 544/69.6% | 23/2.9% |
| Do you believe that these provisions about reaccreditation/recertification should be discussed, and adequate information provided? | 747/95.5% | 25/3.2% | 10/1.3% |
| Do you believe that the reaccreditation/recertification of the specialty should be an ‘official’ procedure, simple to complete, with objective and expected evaluation? | 648/82.9% | 78/10% | 56/7.2% |
| Do you believe that the reaccreditation/recertification of the specialty should be mandatory? | 446/57% | 245/31.3% | 91/11.6% |
| Do you believe that the reaccreditation/recertification of the specialty could be associated with the Periodic Validation of Medical Associations? | 340/43.5% | 259/33.1% | 183/23.4% |
| Are you aware of any similar initiatives in our country in other specialties? | 68/8.7% | 652/83.4% | 62/7.9% |
Regarding the establishment of a reaccreditation procedure, 648 (82.9%) agree that it should be an ‘official’ procedure that is simple to complete, with ‘objective and predictable’ evaluation. While the majority (446; 57%) think that it should be mandatory, 11.6% did not respond, 31.3% did not agree.
Lastly, a uniform general response was not obtained regarding the possible association of the procedure with the Periodic Validation of the Medical Association (PVMA), although this disparity of opinion is diluted in the context of insufficient information.
DiscussionThe results obtained from the survey demonstrate the need for information that clarify the questions posed, which were not known by a large number of surgeons in our country.
‘Certification’ or ‘accreditation’ is a process whereby a medical professional or specialist-in-training demonstrates having acquired the appropriate level of competence with demonstrated quality. ‘Recertification’ refers to the periodic evaluation procedure of practicing medical professionals who are already certified or accredited, thereby confirming maintained and/or improved professional competence8.
In Spain, accreditation is granted by the Ministry of Education, while the Ministry of Health is responsible for designing and monitoring training activities, and the National Commission of each specialty acts as an advisory body. However, recertification must be carried out by the medical societies (and/or medical colleges) and endorsed by the National Healthcare System.
Although there is no consensus on the terminology or contents of the recertification process, it is generally accepted (as the result of the survey also confirms) that a series of criteria or periodic requirements should be established for acting physicians to comply with in order to maintain their skills and medical license up to date. These should be objective and evaluable.
‘Competence’ refers to the dynamic combinations of knowledge, skills and approaches necessary to effectively perform certain tasks. A good model to understand clinical competence has been proposed by Miller9. This author has created a four-step pyramid: “knows” (knowledge), “knows how” (knowing how to apply knowledge), “shows” (technical skills and procedures) and “does” (professional application). It is therefore coherent to consider these concepts when evaluating a process of this type.
The implementation of a recertification system involves the introduction of a procedure that practicing physicians would have to complete periodically, and the majority of the survey participants agree that this should be an ‘official’ procedure with objective evaluation. The introduction of recertification systems has never been easy. However, once this practice is implemented, it is adopted without too many issues, and there is general agreement that it makes a powerful contribution to the prestige and legitimacy of the profession, as viewed by society10. However, the results obtained from the survey show that making it mandatory would be controversial.
The fundamental objectives of recertification would be a triple guarantee: for patients, ensuring that specialists meet certain standards in order to practice as surgeons; for surgeons, guaranteeing that their professional activities are certified by professional associations, medical schools and healthcare administrations; and for society, bearing witness to the quality of these medical activities.
In this context, the General Council of Medical Associations (Consejo General de Colegios de Médicos, or CGCM) has launched a certification procedure called the Periodical Validation for Membership (Validación Periódica de la Colegiación, or PVMA) for which these medical societies evaluate and recognize good professional practice, adequate psychophysical condition and the professional activities of doctors in order to practice their profession, certifying that doctors meet and maintain defined standards for medical practice11.
As a complement to this procedure and in collaboration with certain scientific societies, the concept of PVMA-recertification (PVMA-R) has been created as a system to assess specific competence that the specialist must present based on the CPD and continuing education, as a sort of credential that would certify competence for a 6-year period11. The PVMA-R has been adopted by several scientific societies, such as: the Spanish Society of Pulmonology and Thoracic Surgery, Spanish Society of Digestive Pathology, Spanish Society of Emergency Medicine, Spanish Society of Hematology and Hemotherapy, and the Spanish Society of Pediatric Surgery. However, a large majority of our survey responses claim to be unaware of these initiatives in other specialties.
It may be a difficult-to-resolve error to ‘unionize’ the question if tacit or expressed connections or implications are established with professional advancement. This should be homogeneously defined, adapted and regulated exclusively by the healthcare administration with the consensus of union organizations and medical societies.
The concept of reaccreditation in our specialty is generally not very well known and would require more adequate information.
It would be relevant to design a project based on a rigorous and well-founded analysis of the necessary requirements that justify the recertification and propose an effective ‘tool’ to evaluate activities and competence, possibly using a portfolio-type system.
It should be a document that includes a series of activities considered within the continuing education/CPD concept, defined and proposed by the Scientific Committee of the AEC and accessible to the broad spectrum of surgeons in our country as a ‘roadmap’ for recertification that would ultimately justify issuing an appropriate certificate or credential.
The evaluable activities should also be included in a nationally standardized personal curriculum vitae and could be related to what is contemplated in the OMC document on PVMA-R11. A minimum score required should be established as well.
Parameters that could be included in the reaccreditation program:
- 1
Certified clinical care and clinical management activities.
- 2
Accredited continuing education and CPD activities in the specialty.
- 3
Activity as a professor in accredited activities of the specialty.
- 4
Accredited scientific/research activity.
- 5
Having obtained European BOARD accreditation of the surgical specialty or subspecialties or an accreditation diploma for the Specific Training Area (ACE).
Completion achievement should be part of the point system used for professional advancement at NHS hospitals. The periodicity of reaccreditation could be established at every 6 years, a period that seems logical, appropriate, and has greater national and international recognition.
Conflict of interestsNone.
The authors would like to thank all the surgeons, members of AEC, who have participated in this survey. Thanks also go to the Secretary of the AEC for always being available and making this survey possible, without forgetting all the members of the Training Division and Scientific Committee of the AEC for supporting this project.
Training Division of the Spanish Association of Surgeons (AEC)
Please cite this article as: Miguelena Bobadilla JM, Serra Aracil X, Targarona Soler EM, Ramos Rodríguez JL, Jover Navalón JM, Millán Scheiding M, et al. Reacreditación o recertificación de los cirujanos generales en España: esa es la cuestión. Resultados de una encuesta nacional. Cir Esp. 2022;100:149–153.
recomendados

Cirugía Española (English Edition) sigue las recomendaciones para la preparación, presentación y publicación de trabajos académicos en revistas biomédicas