



The aim of this study was to examine the role of vital exhaustion in predicting the recurrence of vascular events.
MethodThe sample comprised of 816 individuals (65.3% female, Mage=43.2 years, SD=14.7 years), 395 (48.4%) of whom reported treatment for the reoccurrence of a vascular event during the four-year follow-up period. Concurrent effects of baseline vital exhaustion (measured by a shortened version of the Maastricht Questionnaire), depression (assessed by a shortened version of the BDI), anxiety (assessed by the HADS), and hostility (assessed by a shortened version of the Cook-Medley Hostility Scale) in predicting the recurrence of T2 vascular events were examined. The analyses were also controlled for traditional risk factors, such as age, education, body mass index, smoking, alcohol use, and lack of physical activity.
ResultsThe regression analyses showed that vital exhaustion scores significantly predicted the reoccurrence of vascular events even after controlling for all covariates. None of the other psychological predictors (depression, anxiety, and hostility) was significant in the final model.
ConclusionsThese results suggest that despite the partial conceptual overlap with several similar constructs, vital exhaustion is a distinct phenomenon that deserves consideration when planning and implementing interventions to reduce the risk of vascular diseases.
El objetivo de este estudio fue examinar el papel del agotamiento vital en la predicción de la recurrencia de eventos vasculares.
MétodoLa muestra estaba compuesta por 816 sujetos (65,3% mujeres, Medad=43,20 años; DT=14,70 años), 395 (48,40%) de los cuales tuvieron tratamiento para la reincidencia de evento vascular durante los cuatro años de seguimiento. Se examinaron los efectos concurrentes del agotamiento vital inicial (medido por una versión abreviada del Maastricht Questionnaire), depresión (evaluada por una versión abreviada del BDI), ansiedad (evaluada por el HADS) y hostilidad (evaluada por una versión reducida de la Cook-Medley Hostility Scale) en la predicción de la recurrencia de eventos vasculares T2. Los análisis también fueron controlados por factores de riesgo (edad, educación, índice de masa corporal, tabaquismo, consumo de alcohol y falta de actividad física).
ResultadosLas puntuaciones de agotamiento vital predijeron la recurrencia de eventos vasculares, incluso después de controlar todas las covariables. Ninguno de los otros predictores psicológicos fue significativo en el modelo final.
ConclusionesA pesar de la superposición conceptual parcial con varios constructos similares, el agotamiento vital es un fenómeno distinto que merece ser considerado al planificar e implementar intervenciones para reducir el riesgo de enfermedades vasculares.
Vital exhaustion is defined as a state of excessive fatigue, loss of energy, increased irritability, and a sense of demoralization and it has proven to be a precursor of acute myocardial infarction and a risk factor of incident coronary heart disease and cerebrovascular events (Cohen, Bavishi, Haider, Thankachen, & Rozanski, 2017; Frestad & Prescott, 2017; Schnohr et al., 2015). Additionally, studies also have found an association between vital exhaustion and increased risk for adverse cardiac events and mortality in patients with established coronary heart disease (Smith, Kupper, Denollet, & de Jonge, 2011; Zimmermann-Viehoff et al., 2013).
Given the partial conceptual overlaps between vital exhaustion and some related psychological constructs known to be predictive of cardiovascular outcomes, some have criticized the research accumulated to date for neglecting to devote appropriate efforts toward controlling for these related variables when investigating the role of vital exhaustion in the development or prognosis of different cardio- and cerebrovascular disorders (Bianchi, Schonfeld, & Laurent, 2017; Luepker & Schulz, 2015). Therefore, the purpose of the present longitudinal study was to examine whether vital exhaustion predicts recurrent vascular events even when controlling for both traditional lifestyle factors (age, education, body mass index, smoking, alcohol use, and physical activity) and psychological constructs with partial conceptual overlap with vital exhaustion (i.e., depression, anxiety, hostility) that have proven to be significant predictors of vascular diseases (Meijer, Zuidersma, & de Jonge, 2013; Tully, Cosh, & Baune, 2013).
MethodParticipants and procedureThis study evaluated data from the Hungarian Epidemiological Panel Survey, a prospective study with a four-year time lag focusing on the biopsychosocial determinants of chronic diseases of public health importance among Hungarian adults. The study protocol was approved by the Ethical Committee of Semmelweis University. In case of the first wave of data collection, the sampling frame was the National Population Register. Municipalities with a population over 10,000 inhabitants, as well as a representative random sample of smaller communities throughout the country were included. At follow-up, approximately 4 years later, 4524 adult individuals were again interviewed face-to-face. At this time, the sampling frame was limited to those individuals who had given informed consent at baseline to be re-interviewed at follow-up; the refusal rate was 23.7%. The representativeness of the wave 2 sample by age, gender, and sub-region was obtained by a weighting process. A detailed description of the study methodology is available elsewhere (Susánszky et al., 2007).
From the entire sample, the data of 816 individuals (65.3% female, Mage=43.2 years, SD=14.7 years) who reported at baseline that they had been treated for a vascular event were selected for this study. Among those selected, 395 (48.4%) participants reported treatment for at least one additional vascular event during the four-year follow-up period.
InstrumentsThe occurrence of cardiovascular events, as well as other vascular events, at baseline was assessed by three questions: “Have you ever been treated for (1) a cerebrovascular disease; (2) heart attack; (3) other heart or vascular disease?” Initial respondent feedback suggested that more examples would be beneficial in helping participants answer the questions; as such, the wording was modified for the follow-up assessment. At this point, the reoccurrence of vascular events was assessed by two questions: “Since the previous data collection period, have you been treated for (1) cardiac diseases such as coronary artery disease, cardiomyopathy, ischemic heart disease, chest pain (angina), congestive heart failure, or myocardial infarction; (2) other vascular diseases such as transient ischemic attack, apoplexy, thrombosis, embolism, ischemic stroke, or hemorrhagic stroke?” The different vascular event groups were collapsed in the analyses to increase statistical power.
All independent variables of the present analyses were assessed at baseline. Vital exhaustion was assessed by the shortened Hungarian version (MQ-S; Kopp et al., 2010) of the Maastricht Questionnaire. With respect to validity, the shortened Hungarian version was reported to correlate very strongly with the full-length, 21-item questionnaire (r=.94; Kopp, Falger, Appels, & Szedmák, 1998). The internal reliability coefficient of this nine-item assessment tool was good in the present sample (Cronbach's α of .77).
Depressive symptomatology was measured by the shortened Hungarian version (Rózsa, Szádóczky, & Füredi, 2001) of the Beck Depression Inventory (BDI). As reported by Kopp and colleagues, this adaptation contained 9 items (symptoms) from the 21-item version of the BDI and showed a very strong correlation with total BDI scores (r=.92; Kopp et al., 1998). In the present sample, internal consistency of the measure was excellent (Cronbach's α=.83).
Anxiety was measured by the seven items related to anxiety from the Hungarian version (Muszbek et al., 2006) of the Hospital Anxiety and Depression Scale. Internal consistency of the measure was good in the present sample (Cronbach's α=.75). Hostility was assessed by the Hungarian version (Kopp et al., 1998) of the Shortened Cook-Medley Hostility Scale. Internal consistency of this five-item tool was suboptimal in the current sample (Cronbach's α=.64).
A number of conventional risk factors for vascular diseases were also measured, including age (as a continuous variable), educational attainment (six categories), hazardous drinking, smoking status (smoker versus non-smoker), physical activity, and body mass index. Hazardous drinking was assessed by the Hungarian version (Gerevich, Bácskai, & Rózsa, 2006) of the ten-item Alcohol Use Disorder Identification Test (AUDIT), the scores of which were dichotomized using the standard cut-off score of eight. Physical activity was assessed by a single question (“How often are you involved in doing sports; e.g., swimming, jogging, cycling, football, aerobic, etc.?”), which best represented a larger number of questions on physical activity asked in a previous wave of the survey. Response options were 0=never, 1=irregular, once in a while; 2=less than monthly; 3=once in a month; 4=once per week; 5=several times per week; and 6=daily. These were transformed into a dichotomous variable (“0–3” versus “4–6”) in accordance with recent literature pointing out that physical activity, even on a weekly basis, can significantly decrease cardiovascular risk (Després, 2016).
Statistical analysesAll analyses were performed using the SPSS 23.0 statistical package (SPSS Inc., Chicago, Illinois). To investigate the role of vital exhaustion in the reoccurrence of vascular events, a set of hierarchical multiple logistic regression analyses were run. In addition to vital exhaustion, the first model contained the traditional sociodemographic and lifestyle factors relevant for vascular morbidity, followed by depression (second model), and anxiety and hostility (third model).
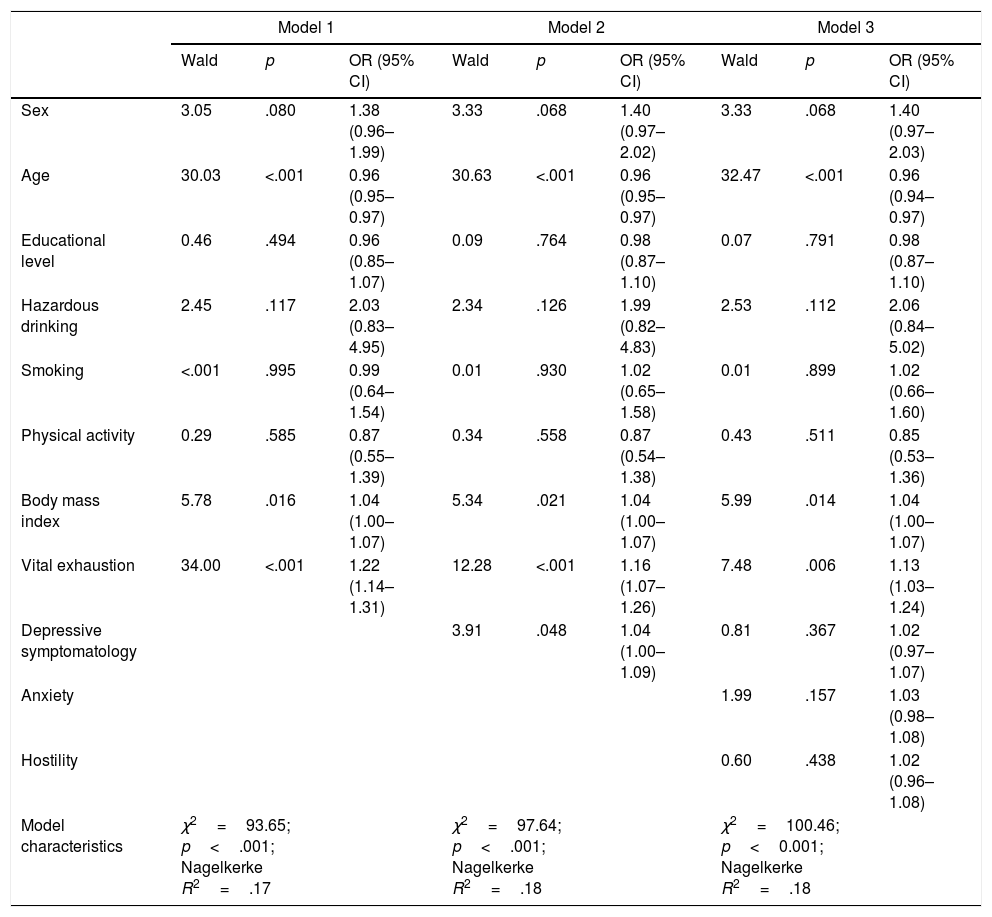
ResultsThe results (Table 1) indicated that an increased level of vital exhaustion was an independent, significant predictor of recurrent vascular events even after controlling for sex, age, educational attainment, hazardous alcohol consumption, smoking, physical activity level, and body mass index (Model 1). When adding depressive symptomatology into the equation, both vital exhaustion and the newly-entered variable were significant in predicting the outcome variable (Model 2). However, when including further variables – namely anxiety and hostility – into the model, only vital exhaustion but not depression, proved to be a significant predictor of the reoccurrence of vascular events (Model 3).
T1 predictors of the re-occurrence of vascular events.
| Model 1 | Model 2 | Model 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Wald | p | OR (95% CI) | Wald | p | OR (95% CI) | Wald | p | OR (95% CI) | |
| Sex | 3.05 | .080 | 1.38 (0.96–1.99) | 3.33 | .068 | 1.40 (0.97–2.02) | 3.33 | .068 | 1.40 (0.97–2.03) |
| Age | 30.03 | <.001 | 0.96 (0.95–0.97) | 30.63 | <.001 | 0.96 (0.95–0.97) | 32.47 | <.001 | 0.96 (0.94–0.97) |
| Educational level | 0.46 | .494 | 0.96 (0.85–1.07) | 0.09 | .764 | 0.98 (0.87–1.10) | 0.07 | .791 | 0.98 (0.87–1.10) |
| Hazardous drinking | 2.45 | .117 | 2.03 (0.83–4.95) | 2.34 | .126 | 1.99 (0.82–4.83) | 2.53 | .112 | 2.06 (0.84–5.02) |
| Smoking | <.001 | .995 | 0.99 (0.64–1.54) | 0.01 | .930 | 1.02 (0.65–1.58) | 0.01 | .899 | 1.02 (0.66–1.60) |
| Physical activity | 0.29 | .585 | 0.87 (0.55–1.39) | 0.34 | .558 | 0.87 (0.54–1.38) | 0.43 | .511 | 0.85 (0.53–1.36) |
| Body mass index | 5.78 | .016 | 1.04 (1.00–1.07) | 5.34 | .021 | 1.04 (1.00–1.07) | 5.99 | .014 | 1.04 (1.00–1.07) |
| Vital exhaustion | 34.00 | <.001 | 1.22 (1.14–1.31) | 12.28 | <.001 | 1.16 (1.07–1.26) | 7.48 | .006 | 1.13 (1.03–1.24) |
| Depressive symptomatology | 3.91 | .048 | 1.04 (1.00–1.09) | 0.81 | .367 | 1.02 (0.97–1.07) | |||
| Anxiety | 1.99 | .157 | 1.03 (0.98–1.08) | ||||||
| Hostility | 0.60 | .438 | 1.02 (0.96–1.08) | ||||||
| Model characteristics | χ2=93.65; p<.001; Nagelkerke R2=.17 | χ2=97.64; p<.001; Nagelkerke R2=.18 | χ2=100.46; p<0.001; Nagelkerke R2=.18 | ||||||
In real life, psychological factors cluster together within individuals and therefore many authors call attention to the need to simultaneously analyze numerous psychosocial factors that are relevant in determining physical health outcomes. The aim of the present study, therefore, was to investigate if vital exhaustion predicts recurrent vascular events even when controlling for related psychological constructs. As vital exhaustion's overlap with depression has received the biggest emphasis in empirical research to date, this latter construct received distinct attention in our analysis as well (i.e., it was entered into the regression model separately from anxiety and hostility).
Our results indicate that even after controlling for sex, age, educational attainment, hazardous alcohol consumption, smoking, physical activity, and body mass index, both vital exhaustion and depressive symptomatology were significant risk factors for the reoccurrence of vascular events. After including anxiety and hostility in the model, the predictive effect of depression disappeared and the newly entered variables were non-significant in predicting the outcome variable; vital exhaustion remained the only psychological variable significantly predicting the reoccurrence of vascular events. These results are consistent with previous studies confirming the distinct nature of vital exhaustion and other constructs in their relation to vascular diseases (Balog et al., 2017; Kudielka, von Känel, Gander, & Fischer, 2004).
This study's strengths include the relatively large sample size, the four-year prospective design, and the large number of related control variables making it possible to compare the concurrent roles of vital exhaustion, depression, anxiety, and hostility in predicting vascular disease prognosis. Nevertheless, several limitations of the present study also need to be acknowledged. First, only self-report data were collected to assess all study variables, including those regarding vascular events. This approach may lead to less reliable data concerning diagnoses due to recall errors and lack of information on vascular events with a fatal outcome. In addition, the slight difference in the wording of the questions referring to the outcome variable is also less ideal than a design with perfect consistency. Further – because of the lack of information from the second assessment point – it was impossible to control for T2 vital exhaustion scores in the analyses or conduct a formal cross-lagged analysis. Finally, psychometric properties of the hostility measure were suboptimal, indicating that the results regarding this variable should be interpreted with caution.
Despite these limitations, our results provide further support for the notion that in spite of the partial conceptual overlap with several similar constructs, vital exhaustion is a distinct phenomenon. The present data also point into the direction that vital exhaustion deserves consideration when planning and implementing interventions to reduce the risk of vascular diseases and as such, it might be considered as an addition to the Systematic Coronary Risk Evaluation (SCORE) algorithm (Graversen, Abildstrøm, Jespersen, Borglykke, & Prescott, 2016).
The authors express their gratitude to late Professor Mária S. Kopp who designed the Hungarian Epidemiological Panel Survey, which was supported by OTKA K-73754/2008 and ETT-100/2006 grants.
