




Petrous apex cholesterol granuloma, a benign pseudocystic lesion, is very infrequent in adults, with an incidence of 0.6 cases per million population in the general population (mean age: 42 years; range, 8–77). It is very rarely reported in the paediatric population.1,2 Its aetiology is unclear, although the most widely accepted hypothesis is that it is caused by a foreign body reaction to cholesterol crystals from an old local haemorrhage, together with poor ventilation of cells.3 History of head trauma or chronic otitis media are predisposing factors. It may be identified incidentally in an MRI study performed for a different reason or manifest with symptoms of headache and cranial nerve compression, sometimes in very aggressive forms: headache (56%), vertigo (33.5%), facial pain or paraesthesia (12.2%), sensorineural hearing loss (6.7%), facial palsy (2.2%), or diplopia (1.1%).2 In MRI studies, it may appear hyperintense on T1- and T2-weighted sequences due to the presence of blood metabolites, with lesions showing no gadolinium uptake.1,4 Differential diagnosis includes other petrous apex lesions such as cholesteatoma, meningioma, schwannoma, glomus jugulare tumour, cartilaginous tumours, lymphoma, Langerhans cell histiocytosis, arachnoid cysts, aneurysms, Wegener granulomatosis, mucocele, and metastasis.3,5 Surgical treatment is classically indicated in symptomatic patients or those with aggressive growth. The intervention aims to drain the content of the granuloma and restore ventilation; recurrences are described in some cases.6--9
We present the case of an 11-year-old boy without history of head trauma or chronic otitis media, who attended our hospital due to 2-month history of headache, associated with diplopia during the previous week.
The physical examination revealed good general health. Vision examination revealed limited abduction of the right eye and diplopia, with normal results for acuity, colour vision, visual field, and eye fundus. Facial sensitivity and motor function were preserved. Otoscope examination of the right ear revealed opacification and patchy ecchymosis of the tympanic membrane. Audiometry of the right ear showed conduction deficit. The Romberg sign was negative, with normal gait and balance.
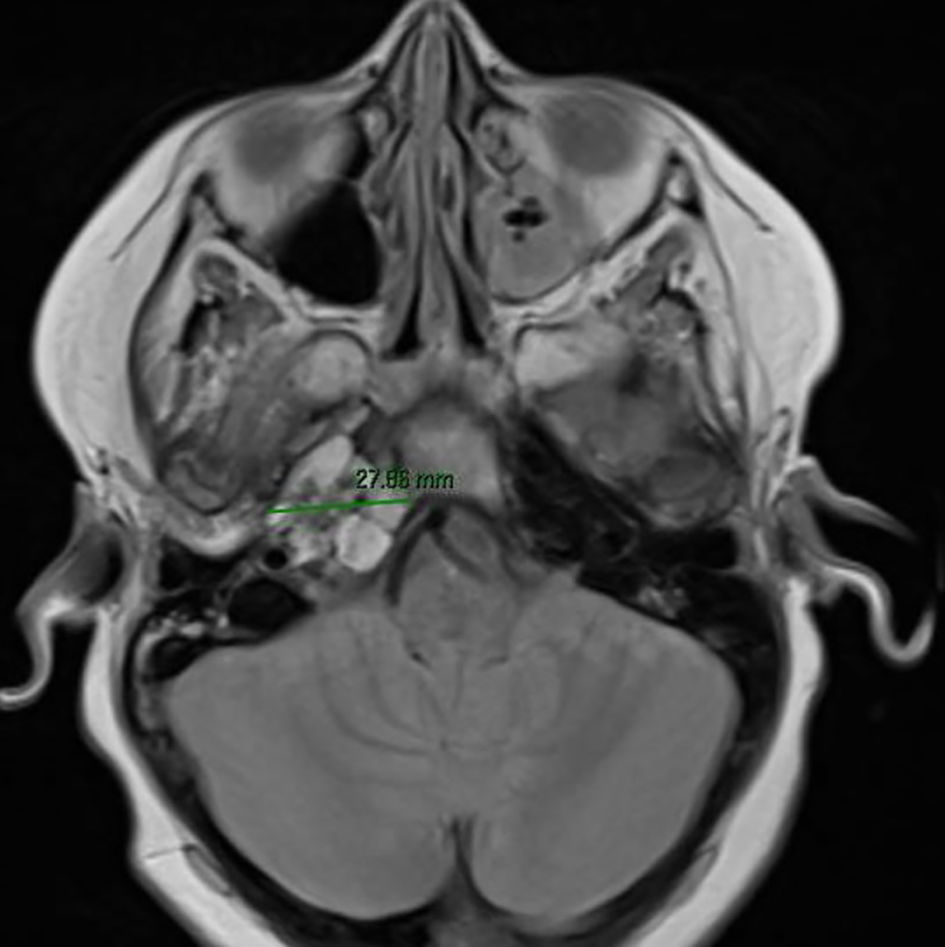
The MRI study showed a polylobulated lesion at the tip of the petrous apex, which was hyperintense on T1- and T2-weighted sequences, and measuring 2 × 2.2 × 2.8 cm. The lesion showed no contrast uptake, and presented a mass effect at the medullopontine level, compressing the sixth cranial nerve in its cisternal segment. Fluid was observed in the mastoid cells, and the cortical layer was intact. These findings are compatible with cholesterol granuloma (Figs. 1 and 2).
 compatible with cholesterol granuloma.")

We consider this case to be exceptional due to the age of the patient and the manifestation with diplopia; a similar case has been published in an adult patient.2
FundingThe authors have received no funding for this study.
Informed consentThe patient and his family gave written informed consent for the use of patient images for scientific purposes.
Ethical considerationsThe authors declare that no human or animal experiments were conducted as part of this study. We disclose no patient data and the rights to privacy and informed consent have been respected.
Supplementary material 1
