



Adenotonsillar hypertrophy (ATH) is an important health condition that leads to upper airway obstruction and constitutes the main cause of obstructive sleep disordered breathing (OSDB) in children. The aim of this study was to analyze the effect of surgical intervention on spirometrical parameters of children with ATH/OSDB and upper airway recurrent infections (URTIs).
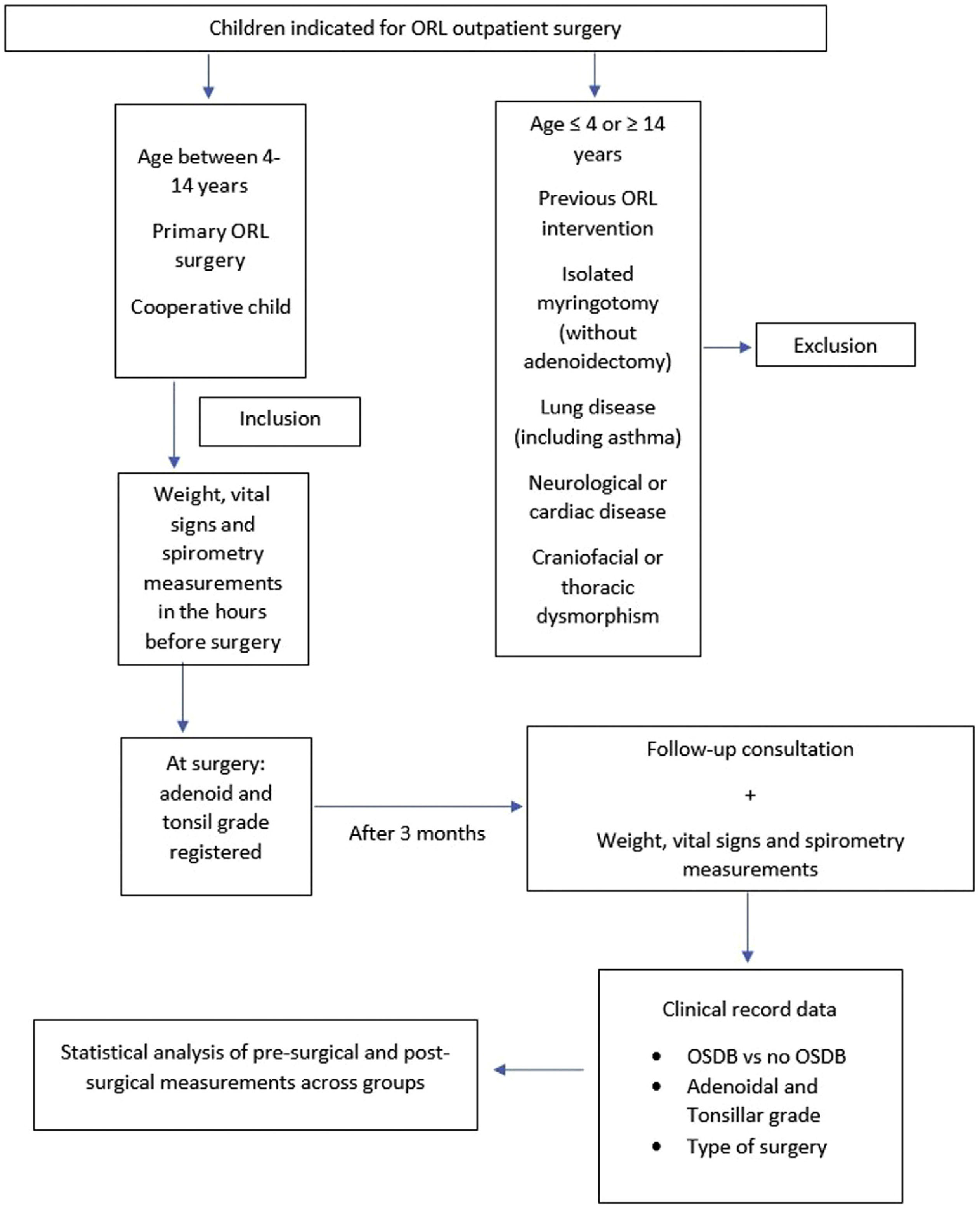
Material and methodsThe study covered children treated surgically in a Pediatric Ambulatory Unit in a tertiary hospital. Spirometric tests were performed before and three months after surgery and results were compared.
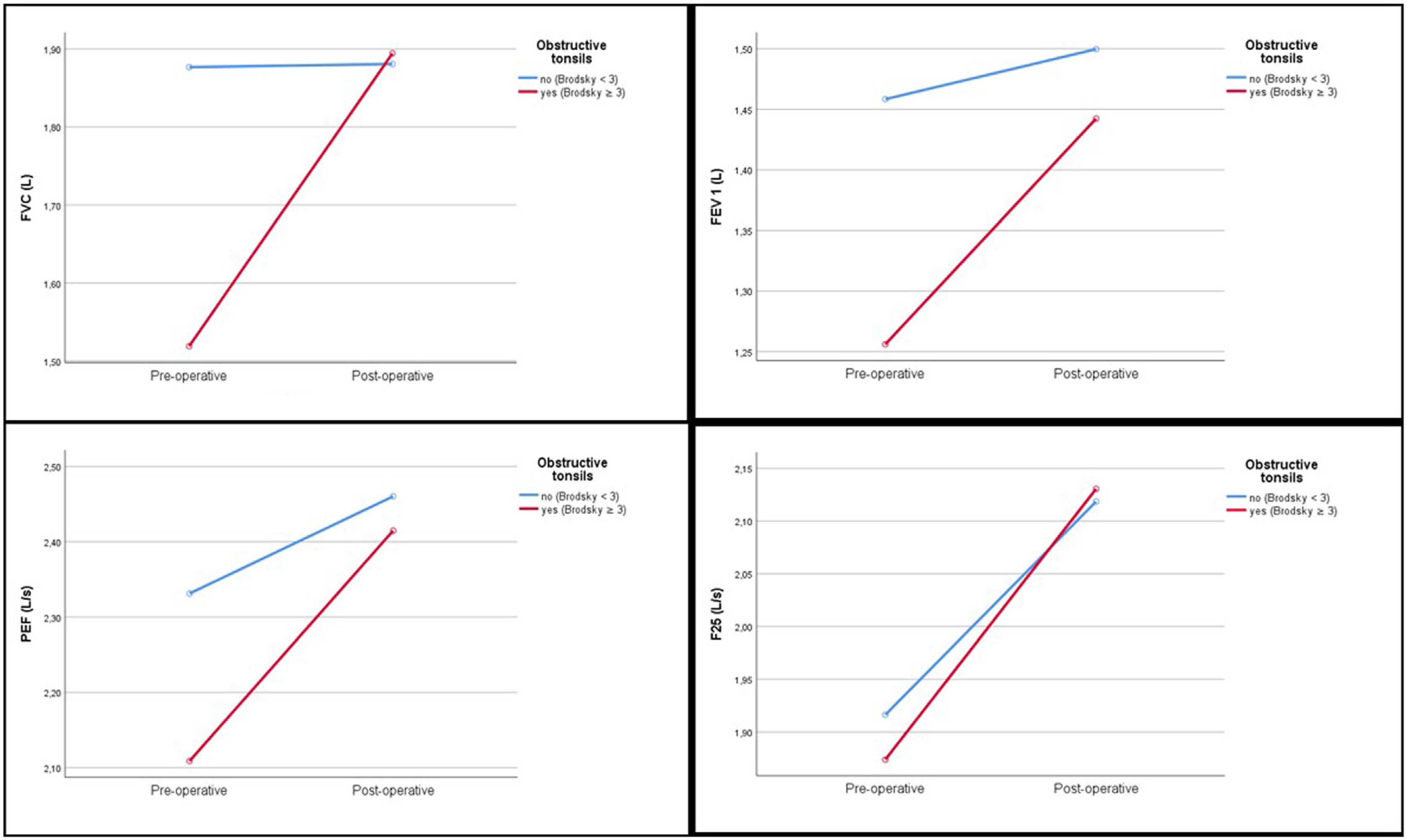
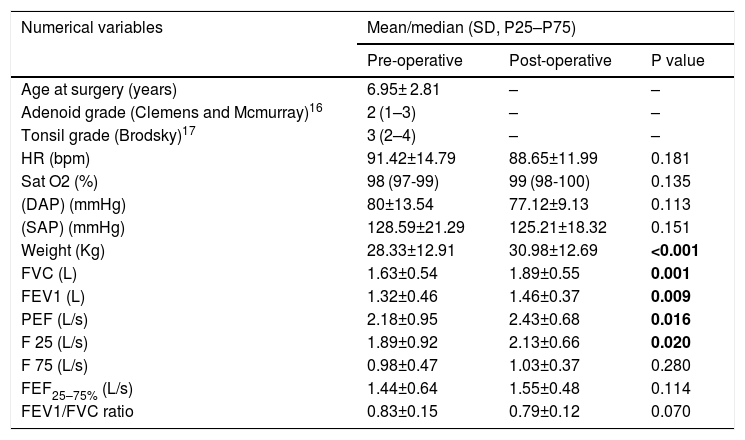
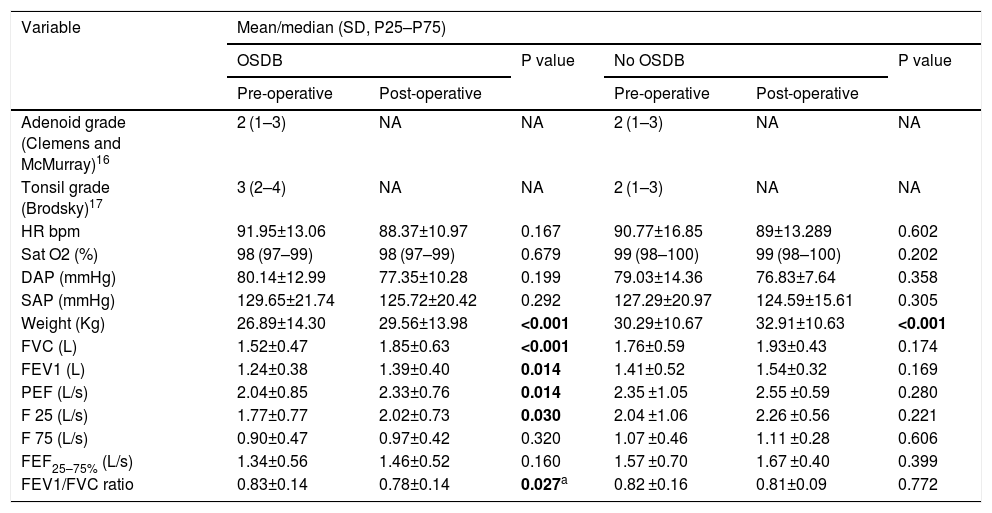
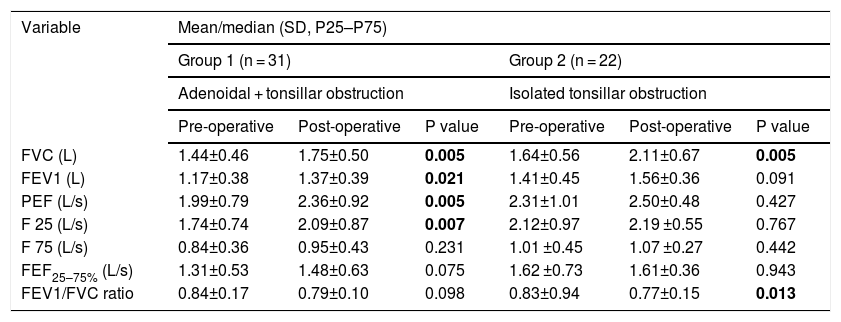
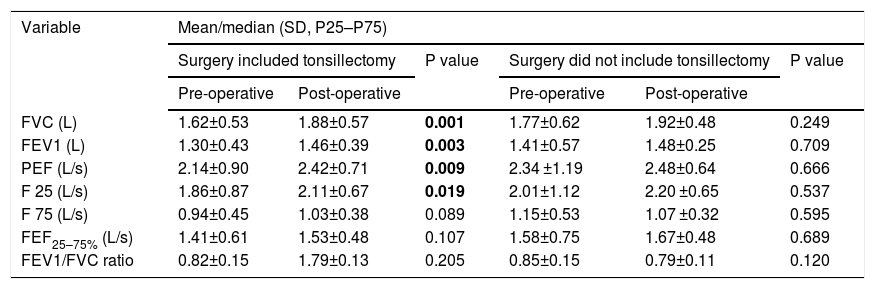
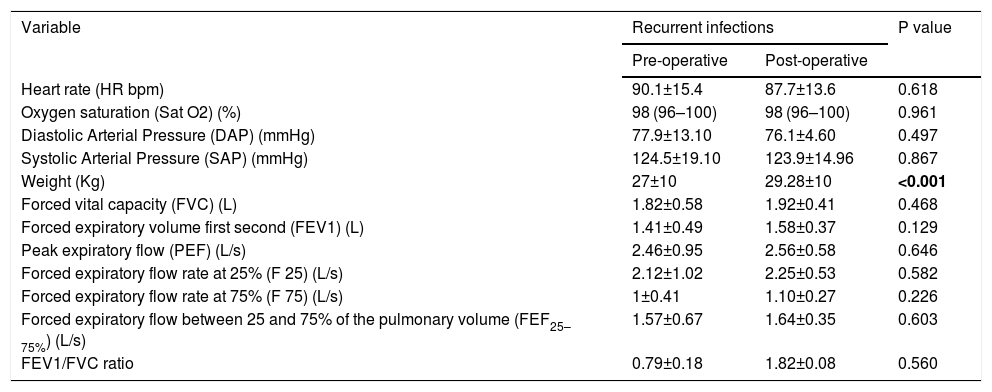
ResultsA total of 78 children were enrolled with a mean age of 6.95 ± 2,81 years. There was a significant improvement in forced vital capacity (FVC), forced expiratory volume in the first second (FEV1), peak expiratory flow (PEF) and forced expiratory flow rate at 25% (F25) values after surgery in children suffering from OSDB (FVC pre: 1.52 ± 0.47 L vs FVC post: 1.85 ± 0.63 L, p < 0.001; FEV1 pre: 1.24 ± 0.38 L vs FEV1 post: 1.39 ± 0.40 L, p = 0.014; PEF pre: 2.04 ± 0.85 L/s vs PEF post: 2.33 ± 0.76 L/s, p = 0.014; F25 pre: 1.77 ± 0.77 L/s vs F25 post: 2.02 ± 0.73 L/s, p = 0.030). On a multivariate analysis model, preoperative tonsil size and performing tonsillectomy were the most significant determinants of improvement in spirometric values (p < 0.05). Children with isolated adenoid hypertrophy without tonsillar obstruction and those with URTIs alone did not show relevant differences in spirometric values after surgery (p > 0.05). No significant differences were found concerning pre-operative and post-operative forced expiratory flow rate at 75% (F75) and forced expiratory flow between 25 and 75% of the pulmonary volume (FEF25–75%) in any group (p > 0.05).
ConclusionsSurgery seems effective in ameliorating spirometry values in patients with OSDB and ATH, namely FVC, FEV1, PEF and F25. Spirometry may give a clue on the importance of adequate surgical resolution of pediatric lymphoid hypertrophy obstruction. No significant differences exist on spirometric parameters of children with isolated adenoid hypertrophy and URTIs without ATH. Further studies are needed in order to evaluate the potential benefit of spirometry utilization in the daily clinical setting.
La hipertrofia adenoamigdalar (HAA) es una importante condición de salud que conduce a la obstrucción de las vías respiratorias superiores y constituye la principal causa de trastornos respiratorios obstructivos del sueño (TROS) en los niños. El objetivo de este estudio fue analizar el efecto de la intervención quirúrgica sobre los parámetros espirométricos de niños con HAA/TROS e infecciones recurrentes de las vías respiratorias superiores (IrVAS).
Material y MétodosEl estudio abarcó a niños operados en una Unidad Ambulatoria Pediátrica de un hospital de tercer nivel. Se realizaron espirometrías antes y tres meses después de la cirugía y se compararon los resultados.
ResultadosSe incluyeron un total de 78 niños con una edad media de 6,95 ± 2,81 años. Hubo una mejora significativa en los valores de capacidad vital forzada (FVC), volumen espiratorio forzado en el primer segundo (FEV1), flujo espiratorio máximo (PEF) y tasa de flujo espiratorio forzado al 25 % (F25) después de la cirugía en niños que sufrían de TROS (FVC pre: 1.52 ± 0.47 L vs FVC post: 1.85 ± 0.63 L, p < 0.001; FEV1 pre: 1.24 ± 0.38 L vs FEV1 post: 1.39 ± 0.40 L, p = 0.014; PEF pre: 2.04 ± 0.85 L/s vs PEF post: 2.33 ± 0.76 L/s, p = 0.014; F25 pre: 1.77 ± 0.77 L/s vs F25 post: 2.02 ± 0.73 L/s, p = 0.030). En un modelo de análisis multivariado, el tamaño preoperatorio de las amígdalas y la amigdalectomía fueron los determinantes más significativos de la mejora en los valores espirométricos (p < 0.005). Los niños con hipertrofia adenoidea aislada sin obstrucción amigdalina y aquellos con IrVAS sin TROS no mostraron diferencias relevantes en los valores espirométricos tras la cirugía (p > 0,05). No se encontraron diferencias significativas en cuanto a flujo espiratorio forzado al 75% (F75) y flujo espiratorio forzado entre el 25 y el 75% del volumen pulmonar (FEF25–75%) en ningún grupo (p > 0,05).
ConclusionesLa cirugía parece efectiva para mejorar los valores de espirometría en pacientes con TROS y HAA, en particular FVC, FEV1, PEF y F25. La espirometría puede dar una pista sobre la importancia de la resolución quirúrgica en la obstrucción por hipertrofia linfoide pediátrica. No hubo diferencias significativas en los parámetros espirométricos de niños con hipertrofia de adenoides aislada y IrVAS sin HAA. Se necesitan más estudios para evaluar el beneficio potencial de la utilización de la espirometría en el entorno clínico diario.
