





Variability in the prevalence of allergic diseases has been detected not only between different countries, but also between cities with similar national and different socio-economic or climatic characteristics. The aim of this study was to determine the prevalence of childhood asthma and allergies and which factors are associated with them, in the two largest Greek cities, Athens and Thessaloniki.
MethodsTwo thousand and twenty-three Greek 9-10-year-old schoolchildren from Athens (Central Greece) and Thessaloniki (North Greece, more humid), were included in ISAAC-II study. All participants followed the ISAAC-II protocol by questionnaire, skin prick testing and flexural dermatitis examination.
ResultsCompared with Athens, the prevalence of current wheezing (8.4% vs. 5.7%, p=0.002), lifetime asthma (11.5% vs. 7.7%, p=0.004), atopic current asthma (3.2% vs. 1.6%, p=0.02), allergic rhinitis (8.2% vs. 5.2%, p=0.007), and hay fever (21.7% vs. 12.5%, p<0.001) were higher in Thessaloniki. The overall sensitisation rate was also higher in Thessaloniki than in Athens (25.2% vs. 16%, p<0.001) with more prevalent sensitising due to the perennial allergens (D. pteronyssinus, D. farinae, Alternaria tenuis) and cat dander. Perennial allergens sensitisation was a risk factor for current asthma in both cities.
ConclusionA higher prevalence of asthma symptoms, allergic rhinitis, and sensitisation rate was detected in Greek schoolchildren living in Thessaloniki compared to those in Athens. Allergy to mites and mould was more prevalent in Thessaloniki. The more humid weather of Thessaloniki may be implicated.
Differences in the prevalence of allergic diseases, not only in countries but also in cities, have been reported by many well-designed studies that cannot be attributed to genetic or national characteristics. In Germany, prevalence rates of asthma, sensitisation and hay fever were greater in the western than in the eastern part, shortly after unification, but a few years later the difference was confirmed only for diagnosed asthma.1 In Spain, considerable geographic variation in the prevalence of asthma symptoms was noted among the 23 centres, emphasising that even among young children, asthma symptoms were more frequent in northern Atlantic cities than in Southern.2 Within Palestinian refugee camps, the prevalence of wheezing in the last 12 months and physician-diagnosed asthma for older schoolchildren was higher in the westernised district of Ramallah than in North Gaza.3 The analysis of three large samples in United Kingdom showed a considerable variation in the prevalence of persistent wheeze and other respiratory symptoms, except occasional wheeze and asthma, by various factors and geographical area.4
In the International Study of Asthma and Allergies in Childhood (ISAAC), great differences were reported between cities with similar national characteristics and geographical points but with varied financial status and ways of life.5 Lifestyle, dietary factors, infections, socio-economic influences, climatic changes, diagnostic differences and management practices have been proposed as causable for these differences.6 The ISAAC phase II (ISAAC-II) data indicated that the prevalence rates of asthma symptoms and atopic sensitisation in children vary widely among the 22 countries worldwide. The link between atopic sensitisation and asthma symptoms differs strongly among populations and increases with economic development.7
There are a number of studies in Greece on childhood asthma and other allergic diseases epidemiology reporting different prevalence rates over the country during the last decade.8–11 In a national sample followed up from birth to adolescence, different epidemiological features of asthma prevalence as measured in seven and 18 year-old people between regions, but within the country, were found.11
The two largest cities in Greece are Athens and Thessaloniki; one is located in the centre and the other in the north of the country. They are characterised by the same financial and living conditions and situated in the same geographic latitude but even at a distance from each other of 500km, experience significant different climate conditions. Both of them were involved in ISAAC-II project. The aim of this study was to evaluate the prevalence of childhood asthma and allergies in these two cities and investigate indoor and outdoor factors associated with the potential differences in the prevalence of the disease. The study based on the hypothesis that macro-environment plays a crucial role in allergic diseases possibly altering or influencing micro-environment. This is one of the few studies which aimed to evaluate the North-to-South polarisation in the prevalence of allergic diseases in the children population, in a Mediterranean country, Greece.
Materials and methodsStudy population and field workDuring October 2000 - November 2001, some 2023 Greek schoolchildren, 1000 from Athens, 1023 from Thessaloniki, aged 9-10 year-old (47.9% boys), were included in the ISAAC-II survey.12 In brief, children were selected from 43 and 31 schools located in the above-mentioned areas, respectively. The selection of schools was random, based on the school listings provided by the Ministry of Education, whereas all children from each school were asked to participate. All participated children a) answered the ISAAC-II questionnaire; b) were tested with skin prick testing (SPT) to seven common aeroallergen produced by ALK (Horsholm, Denmark); and c) were examined for flexural dermatitis. The SPTs were performed for sensitisation to seasonal (mixed grass pollen, mixed tree pollen, and olive tree pollen) or perennial allergens (Dermatophagoides pteronyssinus, Dermatophagoides farinae, Alternaria tenuis) and cat dander. They were considered to be positive if at least one yielded a positive test result. A positive skin-reaction was defined as a wheal diameter of ≥3mm, after subtraction of the negative control.
Institutional Bioethics committees approved the aims and design of the project; children's parents or guardians were informed about the aims and design of the study and provided their consent. The participation rates were 85% and 63%, in Athens and Thessaloniki, respectively.
Questionnaires and other measurementsThe ISAAC standardised and validated self-administered questionnaires enquiring about asthma symptoms, rhinitis and eczema were applied to the parents.13
Factors also studied in this project were nationality of parents (Greek or other), smoking habits of the mother (ever, in pregnancy), smoking habits of other members in the family, parents’ education status, atopic symptoms in parents, birth weight (based on children's medical records), breast feeding (duration in months), order of birth, number of siblings, sharing the bedroom, kindergarten or nursery attendance, pets in house, farm animals, central heating in the house, visible moulds fitted carpets and some dietary habits (eating meat and fish >3 times per week, fruits and vegetables every day).
Geo-climatological information of the citiesAthens is the capital and largest city of Greece that dominates the Attica periphery, located in central Greece. The Greek capital extends beyond the administrative city limits with a large urban zone, thus it is listed as the 7th most populous in the European Union with a population of 4,013,368.14 The city expands on and around seven hills in an area of 3,808km2 and the population density is 987 habitants /km2.15 The climate is typically Mediterranean, with the greatest amounts of precipitation mainly occurring from mid-October to mid-April. Due to its location, in a strong rain shadow, the Athenian climate is much drier compared to most of the rest of Mediterranean Europe and Greek cities. The mountainous northern suburbs, for their part, experience a somewhat differentiated climatic pattern, with generally lower temperatures and more substantial snowfalls during winter, -6°C (21 °F). Summers can be particularly hot. Athens experiences an average humidity range from 47% (July) to 70% (December) with an annual mean rate of 61.8-63.1%. The air-pollution, especially during the hot summers, prone to smog and pollution related conditions, is characterised by high concentrations of particles and photochemical smog.16
Thessaloniki is the second largest city of the country, located in North Greece, with a population of 363,987 in the centre and 763,468 in the entire urban area.14 It lies in an area of 3,683km2 between the northern fringe of the Thermaic Gulf and the south-eastern border of mount Hortiatis. The population density is 284 habitants /km2, much less than the capital. The city borders the Mediterranean and the Mid-European temperate climates with dry winters but morning frost and a hot humid summer. The average humidity ranges from 53.6% (July) to 77.8% (December) with an annual mean rate of 67.3%.16 In the summer, rain is infrequent and in the form of thunderstorms. Air pollution in Thessaloniki is also due to small particles and photochemical smog. Ozone levels are kept at moderate levels as the break-up of the night-time inversion and the onset of the sea breeze decisively decrease concentrates. Winter higher values may be associated with higher fuel consumption but also with natural seasonal variations such as local winter wind with low level inversion layers and poor dispersion conditions.17
Statistical analysisPrevalence of allergic diseases was defined as the ratio of cases divided by the number of subjects. Comparisons between the prevalence of children's and family characteristics between the two cities were made using the Pearson's chi-square test. The cities specific odds ratios as well as their corresponding 95% confidence intervals, for the prevalence of allergic diseases and various children's characteristics have been calculated using logistic regression analysis, after adjusting for factors that showed significance in the univariate analyses. Three models were estimated; one evaluating the association of socioeconomic-environmental factors and any sensitisation (model 1); a second evaluating specific sensitisation after adjusting for socioeconomic-environmental factors (model 2); and the third evaluating only the association of history of allergic diseases (model 3). Hosmer - Lemeshow statistics were calculated and used to assess the models’ goodness of fit. Colinearity between factors entered in each model was evaluated using the correlation coefficients of the estimates. In the diet-specific analysis for asthma, fish variable was not included in the model as there were not enough cases in each stratum. To compare the effect size measures for specific risk factors between Athens and Thessaloniki, we have compared the log-ORs and the corresponding SEs. SPSS 14.0 statistical programme (SPSS Hellas, Athens, Greece) was used to analyse the data.
ResultsDescription of the study sampleIn Table 1 a description of the children's and their families characteristics are presented. There were more parents with academic education in Thessaloniki than in Athens, whereas in Athens more mothers were atopic, they were smoking during pregnancy and they were heavy smokers; in addition, more children shared a room with siblings and more houses were designed with central heating and covered with fitted carpets in Athens. Pet ownership was more frequent in Athens but pets during the first year after child's birth was more frequent in Thessaloniki. The majority of the children (>2/3) were breast fed in both cities, but families in Athens consumed more fruit than in Thessaloniki.
Social-economic, lifestyle and environmental characteristics of the 9-10-year-old children who participated in the study.
| Athens n=1000 | Thessaloniki n=1023 | Ratio AT/TH | p | ALL n=2023 | |
| Sex (male, %) | 46.1 (43, 49) | 49.7 (47, 53) | 0.93 | 0.11 | 47.9 |
| Born in Greece, % | 96.0 (95, 97) | 97.9 (97, 99) | 0.98 | 0.01 | 96.9 |
| Greek both parents, % | 86.9 (85, 89) | 78.1 (76, 81) | 1.11 | <0.01 | 82.5 |
| Parents with academic education, % | 22.8 (20, 25) | 57.0 (54, 60) | 0.40 | <0.01 | 39.9 |
| Mother smoke, % | 43.6 (41, 47) | 45.7 (43, 49) | 0.95 | 0.35 | 44.6 |
| Mother smoke >20 cig/day, % | 21.1 (19, 24) | 12.7 (11, 15) | 1.66 | 0.01 | 17.0 |
| Mother smoke during pregnancy, % | 15.7 (13, 18) | 12.0 (10, 14) | 1.31 | 0.02 | 13.8 |
| Other smoke in family, % | 58.4 (55, 61) | 55.6 (53, 59) | 1.05 | 0.20 | 57.0 |
| Maternal allergic disease % | 28.0 (25, 31) | 23.9 (21, 27) | 1.17 | 0.03 | 25.9 |
| Atopic father, % | 18.5 (16, 21) | 16.9 (15, 19) | 1.09 | 0.35 | 17.7 |
| Birth weight in grams | |||||
| <1500, % | 0.5 (0, 1) | 1.0 (0, 2) | 0.50 | 0.21 | 0.7 |
| 1500-2500, % | 8.1 (6, 10) | 8.2 (6, 10) | 0.99 | 0.92 | 8.1 |
| >2500, % | 91.4 (90, 93) | 90.8 (89, 93) | 1.01 | 0.63 | 91.1 |
| Preterm birth, % | 15.5 (13, 18) | 15.2 (13, 17) | 1.02 | 0.67 | 15.3 |
| Number of siblings | 1.18 (1, 2) | 1.19 (1, 2) | 0.99 | 0.65 | 1.1 |
| >2 siblings, % | 6.8 (5, 8) | 5.5 (4, 7) | 1.24 | 0.22 | 6.1 |
| Order of birth | |||||
| 1st, % | 50.5 (47, 54) | 51.2 (48, 54) | 0.99 | 0.73 | 50.8 |
| last, % | 57.9 (55, 61) | 55.6 (53, 59) | 1.04 | 0.30 | 56.7 |
| Share bedroom now, % | 64.7 (62, 68) | 73.5 (71, 76) | 0.88 | <0.01 | 31.7 |
| Share bedroom from the 1styear, % | 78.4 (76, 81) | 78.1 (76, 81) | 1.00 | 0.88 | 78.2 |
| Breast feeding, % | 78.6 (76, 81) | 74.7 (72, 77) | 1.05 | 0.04 | 76.6 |
| Breast feeding <4m, % | 61.6 (59, 65) | 61.0 (58, 64) | 1.01 | 0.01 | 61.3 |
| Breast feeding >6m, % | 22.9 (20, 26) | 20.2 (18, 23) | 1.13 | 0.13 | 21.5 |
| Kindergarten attendance, % | 91.4 (90, 93) | 90.4 (89, 92) | 1.01 | 0.46 | 90.9 |
| Nursery attendance <2years, % | 13.0 (11, 15) | 10.8 (9, 13) | 1.20 | 0.13 | 11.9 |
| Pets in the house, % | 27.5 (25, 30) | 21.8 (19, 24) | 1.26 | <0.01 | 24.6 |
| Pets in first year of life, % | 8.3 (7, 10) | 12.2 (10, 14) | 0.68 | <0.01 | 10.2 |
| Farm animals, % | 4.0 (3, 5) | 4.7 (3, 6) | 0.85 | 0.44 | 4.3 |
| Farm animals during pregnancy, % | 1.6 (1, 2) | 2.4 (1, 3) | 0.67 | 0.18 | 2.0 |
| Central heating in the house, % | 76.6 (74, 79) | 41.4 (38, 44) | 1.85 | <0.01 | 59.0 |
| Visible moulds in the house, % | 5.7 (4, 7) | 5.4 (4, 7) | 1.06 | 0.75 | 5.5 |
| Fitted carpets in child's bedroom, % | 52.0 (49, 55) | 27.5 (25, 30) | 1.89 | <0.01 | 39.7 |
| Living area urban with no trees, % | 54.8 (52, 58) | 82.4 (0.80,0.85) | 0.67 | <0.01 | 68.6 |
| Eating meat >3/week, % | 13.9 (12, 16) | 12.2 (10, 14) | 1.14 | 0.79 | 13.0 |
| Eating fish >2/week, % | 3.7 (3, 5) | 4.4 (3, 6) | 0.84 | 0.79 | 4.0 |
| Eating fruits every day, % | 51.3 (48, 54) | 44.2 (41, 47) | 1.16 | 0.02 | 47.7 |
| Eating vegetables every day, % | 24.9 (22, 28) | 24.5 (22, 27) | 1.02 | 0.29 | 24.7 |
Results are presented as percentages, 95% Confidence Intervals and ratios between Athens and Thessaloniki. P-values retrieved from Pearson's chi square test.
Prevalence of current wheezing and atopic current asthma was higher in Thessaloniki compared with Athens (8.4% vs. 5.7%, P=0.02, and 3.2% vs 1.6%, P=0.02, Table 2). Moreover, lifetime asthma was more prevalent in Thessaloniki (11.5% vs. 7.7%, P=0.004), as well as allergic rhinitis, atopic current rhinitis and hay fever (P -values<0.05). No differences between the two cities were observed regarding the rates of current rhinitis, lifetime rhinitis, and eczema. Finally, the overall sensitisation rate to any allergen among children in Thessaloniki was higher compared to those in Athens (p<0.001); similarly, sensitisation rates to specific allergens such as perennial allergens and cat dander were higher in Thessaloniki than in Athens (P<0.05).
Prevalence of allergic diseases and sensitisation in 9-10-year-old children who participated in the study.
| Allergic disease | Athens n=1000 | Thessaloniki n=1023 | Ratio AT/TH | p | ALL n=2023 |
| 12-months current asthma | |||||
| Current wheezing,% | 5.7 (4, 7) | 8.4 (7, 10) | 0.68 | 0.02 | 7.1 |
| >4 episodes /y, % | 1.2 (1, 2) | 0.7 (0, 1) | 1.71 | 0.23 | 0.9 |
| Dyspnoea episodes,% | 0.7 (0, 1) | 1.6 (1, 2) | 0.44 | <0.001 | 1.1 |
| Admissions, % | - | 0.9 (0, 1) | - | 0.03 | 0.9 |
| Atopic current asthma,% | 1.6 (1, 2) | 3.2 (2, 4) | 0.50 | 0.01 | 2.4 |
| Lifetime asthma, % | 7.7 (6, 9) | 11.5 (10, 13) | 0.67 | <0.01 | 9.6 |
| 12 months rhinitis | |||||
| Current rhinitis, % | 18.1 (16, 20) | 19.9 (17, 22) | 0.91 | 0.30 | 19.0 |
| Rhinitis interfere actions,% | 1.3 (1, 2) | 2.8 (2, 4) | 0.46 | 0.02 | 2.0 |
| Atopic current rhinitis, % | 4.4 (3, 6) | 7.4 (6, 9) | 0.59 | <0.001 | 5.9 |
| Hay fever, % | 12.5 (10, 15) | 21.7 (19, 24) | 0.58 | <0.001 | 17.1 |
| Lifetime rhinitis, % | 21.3 (19, 24) | 24.2 (22, 27) | 0.88 | 0.12 | 22.8 |
| Allergic rhinitis, % | 5.2 (4, 7) | 8.2 (7, 10) | 0.63 | <0.001 | 6.7 |
| 12 months eczema | |||||
| current eczema, % | 10.1 (8, 12) | 8.2 (7, 10) | 1.23 | 0.16 | 9.1 |
| flexural dermatitis, % | 1.3 (1, 2) | 1.4 (1, 2) | 0.93 | 0.89 | 1.3 |
| atopic eczema, % | 2.1 (1, 3) | 1.9 (1, 3) | 1.11 | 0.58 | 2.0 |
| sleep problems >1/week, % | 1.4 (1, 2) | 1.8 (1, 3) | 0.78 | 0.41 | 1.6 |
| Lifetime eczema, % | 14.4 (12, 17) | 11.7 (10, 14) | 1.23 | <0.001 | 13 |
| Skin Prick Test | |||||
| At least one, % | 16.0 (14, 18) | 25.2 (23, 28) | 0.63 | <0.001 | 20.7 |
| Pollen sensitisation, % | 14.7 (13, 17) | 17.0 (15, 19) | 0.86 | 0.15 | 10.2 |
| Perennial sensitisation, % | 4.1 (3, 5) | 7.3 (6, 9) | 0.56 | <0.001 | 10.8 |
| Cat sensitisation, % | 5.8 (4, 7) | 8.7 (7, 10) | 0.67 | 0.01 | 7.3 |
Results are presented as percentages, 95% Confidence Intervals and ratios between Athens and Thessaloniki. P-values retrieved from Pearson's chi square test. Atopic were children with asthma, rhinitis or eczema, after sensitisation to at least one allergen (positive skin test). Hay fever was the seasonal allergic rhinitis after sensitisation to pollen. Lifetime was defined as ever having had the symptom in the children's life, current was defined as having the symptom during the last 12 months.
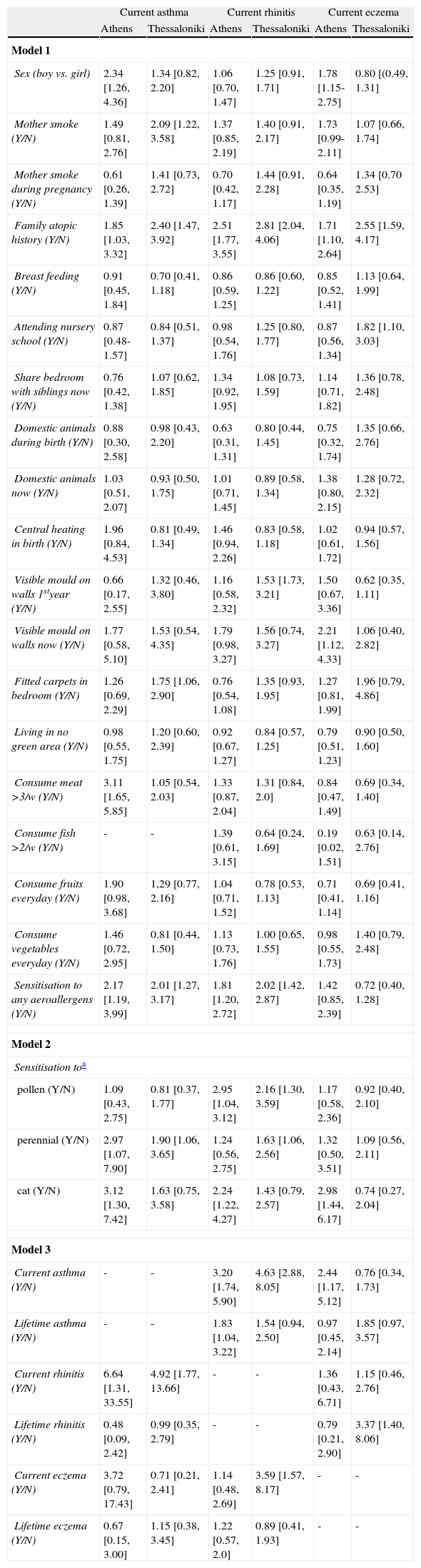
Further analysis evaluated factors associated with current asthma, rhinitis and eczema, in Athens and Thessaloniki, separately (Table 3). Colinearity between these factors was not evident in all three models estimated. Boys were more likely to have current asthma and eczema than girls in Athens, but not in Thessaloniki. Mother's smoking habits were associated only with current asthma in children living in Thessaloniki. Atopic family history was found as a factor associated with current asthma, rhinitis and eczema, in both cities. No differences were observed between the cities regarding parental allergy (Table 3). Fitted carpets in the bedroom were associated to current wheezing in Thessaloniki, visible mould in walls was associated to eczema in Athens, while visible mould in walls during the first year of life was associated to current rhinitis in Thessaloniki. Attending nursery school was associated with eczema in Thessaloniki.
Results from multiple logistic regression analyses (odds ratio and 95% CI) that evaluated factors associated with asthma and allergies in 9-10-year-old children living in Athens and Thessaloniki, Greece.
| Current asthma | Current rhinitis | Current eczema | ||||
| Athens | Thessaloniki | Athens | Thessaloniki | Athens | Thessaloniki | |
| Model 1 | ||||||
| Sex (boy vs. girl) | 2.34 [1.26, 4.36] | 1.34 [0.82, 2.20] | 1.06 [0.70, 1.47] | 1.25 [0.91, 1.71] | 1.78 [1.15-2.75] | 0.80 [(0.49, 1.31] |
| Mother smoke (Y/N) | 1.49 [0.81, 2.76] | 2.09 [1.22, 3.58] | 1.37 [0.85, 2.19] | 1.40 [0.91, 2.17] | 1.73 [0.99-2.11] | 1.07 [0.66, 1.74] |
| Mother smoke during pregnancy (Y/N) | 0.61 [0.26, 1.39] | 1.41 [0.73, 2.72] | 0.70 [0.42, 1.17] | 1.44 [0.91, 2.28] | 0.64 [0.35, 1.19] | 1.34 [0.70 2.53] |
| Family atopic history (Y/N) | 1.85 [1.03, 3.32] | 2.40 [1.47, 3.92] | 2.51 [1.77, 3.55] | 2.81 [2.04, 4.06] | 1.71 [1.10, 2.64] | 2.55 [1.59, 4.17] |
| Breast feeding (Y/N) | 0.91 [0.45, 1.84] | 0.70 [0.41, 1.18] | 0.86 [0.59, 1.25] | 0.86 [0.60, 1.22] | 0.85 [0.52, 1.41] | 1.13 [0.64, 1.99] |
| Attending nursery school (Y/N) | 0.87 [0.48-1.57] | 0.84 [0.51, 1.37] | 0.98 [0.54, 1.76] | 1.25 [0.80, 1.77] | 0.87 [0.56, 1.34] | 1.82 [1.10, 3.03] |
| Share bedroom with siblings now (Y/N) | 0.76 [0.42, 1.38] | 1.07 [0.62, 1.85] | 1.34 [0.92, 1.95] | 1.08 [0.73, 1.59] | 1.14 [0.71, 1.82] | 1.36 [0.78, 2.48] |
| Domestic animals during birth (Y/N) | 0.88 [0.30, 2.58] | 0.98 [0.43, 2.20] | 0.63 [0.31, 1.31] | 0.80 [0.44, 1.45] | 0.75 [0.32, 1.74] | 1.35 [0.66, 2.76] |
| Domestic animals now (Y/N) | 1.03 [0.51, 2.07] | 0.93 [0.50, 1.75] | 1.01 [0.71, 1.45] | 0.89 [0.58, 1.34] | 1.38 [0.80, 2.15] | 1.28 [0.72, 2.32] |
| Central heating in birth (Y/N) | 1.96 [0.84, 4.53] | 0.81 [0.49, 1.34] | 1.46 [0.94, 2.26] | 0.83 [0.58, 1.18] | 1.02 [0.61, 1.72] | 0.94 [0.57, 1.56] |
| Visible mould on walls 1styear (Y/N) | 0.66 [0.17, 2.55] | 1.32 [0.46, 3.80] | 1.16 [0.58, 2.32] | 1.53 [1.73, 3.21] | 1.50 [0.67, 3.36] | 0.62 [0.35, 1.11] |
| Visible mould on walls now (Y/N) | 1.77 [0.58, 5.10] | 1.53 [0.54, 4.35] | 1.79 [0.98, 3.27] | 1.56 [0.74, 3.27] | 2.21 [1.12, 4.33] | 1.06 [0.40, 2.82] |
| Fitted carpets in bedroom (Y/N) | 1.26 [0.69, 2.29] | 1.75 [1.06, 2.90] | 0.76 [0.54, 1.08] | 1.35 [0.93, 1.95] | 1.27 [0.81, 1.99] | 1.96 [0.79, 4.86] |
| Living in no green area (Y/N) | 0.98 [0.55, 1.75] | 1.20 [0.60, 2.39] | 0.92 [0.67, 1.27] | 0.84 [0.57, 1.25] | 0.79 [0.51, 1.23] | 0.90 [0.50, 1.60] |
| Consume meat >3/w (Y/N) | 3.11 [1.65, 5.85] | 1.05 [0.54, 2.03] | 1.33 [0.87, 2.04] | 1.31 [0.84, 2.0] | 0.84 [0.47, 1.49] | 0.69 [0.34, 1.40] |
| Consume fish >2/w (Y/N) | - | - | 1.39 [0.61, 3.15] | 0.64 [0.24, 1.69] | 0.19 [0.02, 1.51] | 0.63 [0.14, 2.76] |
| Consume fruits everyday (Y/N) | 1.90 [0.98, 3.68] | 1,29 [0.77, 2.16] | 1.04 [0.71, 1.52] | 0.78 [0.53, 1.13] | 0.71 [0.41, 1.14] | 0.69 [0.41, 1.16] |
| Consume vegetables everyday (Y/N) | 1.46 [0.72, 2.95] | 0.81 [0.44, 1.50] | 1.13 [0.73, 1.76] | 1.00 [0.65, 1.55] | 0.98 [0.55, 1.73] | 1.40 [0.79, 2.48] |
| Sensitisation to any aeroallergens (Y/N) | 2.17 [1.19, 3.99] | 2.01 [1.27, 3.17] | 1.81 [1.20, 2.72] | 2.02 [1.42, 2.87] | 1.42 [0.85, 2.39] | 0.72 [0.40, 1.28] |
| Model 2 | ||||||
| Sensitisation toa | ||||||
| pollen (Y/N) | 1.09 [0.43, 2.75] | 0.81 [0.37, 1.77] | 2.95 [1.04, 3.12] | 2.16 [1.30, 3.59] | 1.17 [0.58, 2.36] | 0.92 [0.40, 2.10] |
| perennial (Y/N) | 2.97 [1.07, 7.90] | 1.90 [1.06, 3.65] | 1.24 [0.56, 2.75] | 1.63 [1.06, 2.56] | 1.32 [0.50, 3.51] | 1.09 [0.56, 2.11] |
| cat (Y/N) | 3.12 [1.30, 7.42] | 1.63 [0.75, 3.58] | 2.24 [1.22, 4.27] | 1.43 [0.79, 2.57] | 2.98 [1.44, 6.17] | 0.74 [0.27, 2.04] |
| Model 3 | ||||||
| Current asthma (Y/N) | - | - | 3.20 [1.74, 5.90] | 4.63 [2.88, 8.05] | 2.44 [1.17, 5.12] | 0.76 [0.34, 1.73] |
| Lifetime asthma (Y/N) | - | - | 1.83 [1.04, 3.22] | 1.54 [0.94, 2.50] | 0.97 [0.45, 2.14] | 1.85 [0.97, 3.57] |
| Current rhinitis (Y/N) | 6.64 [1.31, 33.55] | 4.92 [1.77, 13.66] | - | - | 1.36 [0.43, 6.71] | 1.15 [0.46, 2.76] |
| Lifetime rhinitis (Y/N) | 0.48 [0.09, 2.42] | 0.99 [0.35, 2.79] | - | - | 0.79 [0.21, 2.90] | 3.37 [1.40, 8.06] |
| Current eczema (Y/N) | 3.72 [0.79, 17.43] | 0.71 [0.21, 2.41] | 1.14 [0.48, 2.69] | 3.59 [1.57, 8.17] | - | - |
| Lifetime eczema (Y/N) | 0.67 [0.15, 3.00] | 1.15 [0.38, 3.45] | 1.22 [0.57, 2.0] | 0.89 [0.41, 1.93] | - | - |
Regarding food habits, meat consumption more than three times per week was associated with current asthma only in Athens (Table 3); none of the other food habits investigated was associated with current asthma, rhinitis, or eczema in children.
Sensitisation to any aeroallergen was related to current asthma and rhinitis in both cities but not to current eczema (model 1, Table 3). Sensitisation to pollen was related to current rhinitis in both cities, to perennial allergens and to current asthma in both cities, and to current rhinitis only in Thessaloniki. Sensitisation to cat was associated with current asthma, rhinitis, and eczema only in the Athens area, after various adjustments were made (model 2, Table 3).
Current asthma was related to current rhinitis in both cities and to current eczema only in Athens, but lifetime asthma was related to current rhinitis in Athens only. Current rhinitis was related to asthmatic symptoms in both cities, lifetime and current rhinitis to current eczema only in Thessaloniki (model 3, Table 3).
Figure 1 depicts the prevalence of sensitisation to each of the seven aeroallergens tested in the two cities. Higher prevalence of any sensitisation was observed in Thessaloniki compared to Athens (25.2% vs. 16.0%, P<0.0001), as well as to specific types of sensitisation, such as D. pteronyssinus (12.5% vs. 3.4%, P<0.0001), D. farinae (5.2% vs. 0.8%, P<0.0001), Alternaria (4.4% vs. 0.5%, P<0.0001), cat (8.7% vs. 5.8%, P=0.01), and mix trees (2.9% vs. 0.8%, P<0.001).
Discussion
The present work, within the context of ISAAC phase II, aimed to examine differences in the prevalence of allergic diseases and the associated risk factors between the two largest Greek cities, Athens and Thessaloniki. The main findings were that Thessaloniki had higher prevalence of asthma, allergic rhinitis and sensitisation rate than Athens; sensitisation was related to current asthma and allergic rhinitis, but not to current eczema in both cities, while sensitisation to cat was associated with current asthma, rhinitis, and eczema only in Athens. It is of interest that none of the living conditions investigated, lifestyle, or other personal and family characteristics had any explanatory role in the differences observed in allergic disease rates between Athens and Thessaloniki. Several factors, such as gender; parental smoking habits; atopic family history and sensitisation to any or to perennial allergens; visible mould on house walls; attending nursery school; and eating meat and its products, were associated with the prevalence of these diseases in Athens, and in Thessaloniki, separately (see Table 3). Despite the limitations of the cross-sectional design, this is one of the few studies that aimed to evaluate the North-to-South polarisation in the prevalence of allergic diseases in a children's population, in a Mediterranean country, Greece. However, clear causative factors cannot be revealed, but the results presented here may be the basis for further research analysing quality and quantity in pairs of factors while controlling genetic background in order to explain the differences in event rates between countries, or between cities within one country.
Many studies have demonstrated the presence of geographic differences within countries regarding the prevalence of allergic diseases in children. These differences were not attributed to genetic or national characteristics. Environmental factors such as climatic and socio-environmental conditions could be implicated.1–7,11,18–23 Climatic conditions, like humidity and temperature, have been related to asthma prevalence in few studies, where exacerbations of the disease were correlated with changes in the weather. In a study investigating two different geo-climatic zones (coast and plateau) – based on their relative humidity and temperature range – it was found that mean asthma prevalence in the coastal areas was higher than that on the plateau.24 In another study, in Spain, three different climatic regions were tested and they found positive association with precipitation and humidity and a negative one with temperature and number of sunny hours.25 Fluctuations in humidity and temperature, that influenced emergency department visits due to paediatric asthma exacerbations, have also been reported.26
In our study, the weather conditions between the two cities were not analysed; however this characteristic appears to be their major difference and it could be speculated that humidity is the underlying cause of the higher prevalence of asthma and allergic rhinitis in Thessaloniki as compared to Athens. From the whole analysis, the prevalence difference cannot be explained by differences in living conditions, lifestyle factors, or other family characteristics. The more humid weather in Thessaloniki has been convincingly documented in a number of studies.16,17,27,28
Our analysis also revealed that maternal smoking was strongly associated with current asthma, especially in Thessaloniki (Table 3). Many cross-sectional and longitudinal observational studies suggest that, for asthma and pulmonary function outcomes, the strongest associations are with smoke exposure in utero and in early childhood.29,30 Exposure in later childhood to environmental tobacco smoke is associated with increased respiratory symptoms.29 We also found that fitted carpets and visible mould on walls were independent risk factors for current wheezing and rhinitis respectively in Thessaloniki. These observations are in line with existing literature showing that home dampness increases the indoor mould burden and is associated with increased allergic symptoms among young children, not only in temperate environments but even in the tropics.31 Both smoking and fitted carpets were factors higher detected in Athens (Table 1), but were shown to be associated to asthma prevalence only in Thessaloniki (Table 3).
The cumulative analysis of ISAAC phase II data revealed a wide variation in the prevalence of atopic sensitisation across the study's centres, with a weak link to asthma symptoms, rhinitis symptoms, and flexural eczema; it could be speculated that the importance of other environmental factors may vary in different conditions and could explain, at least in part, these differences.7 In the present study, sensitisation was related to current asthma and allergic rhinitis in both cities, but Thessaloniki had a higher sensitisation rate, lending support to the importance of sensitisation to asthma symptoms.32,33 Although sensitisation to seasonal allergens was the more prevalent sensitising allergen in both cities (Table 1), there was a slight difference in the effect size measures as regards sensitisation to perennial allergens and to cat dander on asthma symptoms between the two cites (Table 3). Allergy to mites and mould, i.e. perennial allergens, was more prevalent in Thessaloniki. Higher concentrations of Cladosporium and Alternaria spores in the more humid climate of Thessaloniki as compared to Athens have been reported previously.34 Consequently, in contrast to the drier climate of Athens, the humid weather of Thessaloniki probably provokes aeroallergens proliferation and facilitates induction of asthma by increasing sensitisation. These observations and hypotheses may also have implications for the assessment of potential health effects due to climate change observed in Europe and around the world in the last decades.
In our study, we found that pet ownership was more common in Athens and sensitisation to cat was associated with all allergic diseases only in Athens; however, sensitisation to cat was again more prevalent in Thessaloniki, where children were more likely to be exposed from the first year of life. Although data from recent years have shown that pet exposure in early childhood may actually prevent the development of allergic sensitisation and allergic diseases, our data do not support this. In contrast, genetic factors such as filaggrin mutation influence the expression of eczema in cat owners.35 Thus, genetic studies investigating the profile of Athenian versus Thessalonikan children might enlighten the different results even though the concept of a protective pet effect remains controversial and seems to be influenced by multiple factors.36,37
Diet plays a significant role in allergic disease, independent of sensitisation. ISAAC phase I and other studies emphasise the protective effect of fibre, vegetable, fruits, and fish in the probability of asthma.38 In Athens, children consumed more fruit daily than those in Thessaloniki, but it was not associated with current asthma. On the other hand, meat consumption more than three times per week was related to current wheezing. However, it should be acknowledged that in the ISAAC questionnaire we used in this work, diet history was not precisely defined and the information regarding duration and quantity of foods consumed was not clarified. Thus, a definite conclusion cannot be drawn.
Attendance at nursery school was more common in Athens but it was not found to be related to any allergic diseases; on the contrary, such attendance was related to current eczema in Thessaloniki. Most studies agree that early day-care attendance reduces risk for current wheeze or sensitisation.39 An increased risk of current eczema without any sign of asthma symptoms protection among children attending day-care centres has also been reported.40
Nearly all of the allergens we tested for, except olive tree pollen, showed a higher prevalence rate of sensitisation in Thessaloniki compared to Athens. These findings are in agreement with the results of another similar study conducted at the same time in schoolchildren in Athens 37; however, sensitisation rates to mites and moulds were not as low as found in the present one. In ISAAC phase II participated children living in various regions of Athens have a better chance to be exposed to the dry climate of Athens. For Thessaloniki, this is the first study to evaluate the sensitisation rates in a sample of schoolchildren in the general population.
The ISAAC-II study, as a cross-sectional study, shares the limitations of observational studies, like recall bias and absence of causal relationships. We had no data on air pollution for either city but both are the two major metropolitan areas of Greece. The target populations in both cities were living in heavy traffic areas.
ConclusionThe present study revealed a higher prevalence of asthma symptoms, allergic rhinitis and sensitisation rate in Greek schoolchildren living in Thessaloniki than in Athens. Allergy to perennial allergens such as mites and mould was more prevalent in Thessaloniki. The more humid weather of Thessaloniki probably provokes aeroallergen proliferation and may facilitate the development of asthma and allergic rhinitis by increasing sensitisation.
