


House dust mites are a ubiquitous air allergen in the human habitat. It has been shown that exposure to them is a fundamental factor in sensitisation and development of atopic disease. The objective of the study was to analyse changes in sensitisation to Dermatophagoides pteronyssinus (Der p.) in children treated in a tertiary level care hospital in Mexico City for a period of 11 years and compare with other studies carried out in Mexico.
MethodsA retrospective study was performed at the Hospital Infantil de México Federico Gómez (HIMFG). Information was gathered from skin tests for Der p. performed in the Allergy Laboratory from January 2004 to April 2015. Patients 2–18 years old who presented for examination of some type of allergic condition and who had immediate hypersensitivity tests to Der p. were included in the study. Results were compared with prior reports from other institutions. Descriptive analysis and χ2 statistics were used.
ResultsA total of 8794 patients were included in the study; 49.3% of the tests (95% CI 48–50) were positive for Der p. The percentage of monosensitised to mites was 2.7% for Der p. (95% CI 2–3). A significant difference was found between the results of older patients and those <6 years old. The frequency of sensitisation had a tendency to decrease during the 11 years analysed in all age groups.
Conclusions and clinical relevanceThe frequency of sensitisation to Der p. increased with age until reaching adolescence. In the last 11 years a decrease in sensitisation to this air allergen was observed.
The house dust mite is a ubiquitous air allergen in human habitat and is considered to be one of the most important causes of sensitisation to indoor allergens.1,2 It is an eight-legged arthropod of the arachnid group, belonging to the order Acari and comprises a large number of species grouped under several suborders, families and genera.
The term “house dust mites” has been used traditionally for members of the family Pyroglyphidae that live permanently and almost exclusively in house dust where the main representatives (80–90%) are Dermatophagoides pteronyssinus (Der p.), Dermatophagoides farinae (Der f.), and Euroglyhpus maynei; whereas others such as Blomia tropicalis and Lipidoglyphus destructor, despite being considered as warehouse mites, are species commonly found in homes located in tropical and subtropical climates.3
It has been demonstrated that exposure to dust mites is a fundamental factor for sensitisation and development of atopic pathology.4 The prevalence of exposure and sensitisation varies greatly according to the region studied, which greatly depends on geographic and environmental factors of the mentioned regions, i.e., in Spain a sensitisation for Dermatophagoides is reported in children <6 years old of 11.8%, in Germany of 11.9% and The Netherlands of 13.6%,5 with an overall average prevalence in Europe of 21.7% (4.8–36.8%) for Der p.6; whereas in Korea the frequency of sensitisation is from 36.8 to 40.9%.7 In Latin America the frequency depends on the study location and ranges from 60.7% to Der p. in Colombia to 91.2% in Brazil.8
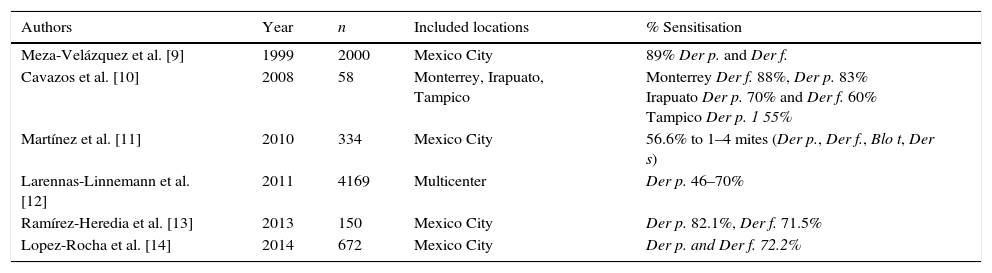
According to world statistics, an estimated 1–2% of the world's population could be allergic to this allergen, i.e., equivalent to 65–130 million persons.1 In México, various studies have been published on the frequency of sensitisation to house dust mites (Table 1).
Prevalence of house dust mite sensitisation in Mexico.
| Authors | Year | n | Included locations | % Sensitisation |
|---|---|---|---|---|
| Meza-Velázquez et al. [9] | 1999 | 2000 | Mexico City | 89% Der p. and Der f. |
| Cavazos et al. [10] | 2008 | 58 | Monterrey, Irapuato, Tampico | Monterrey Der f. 88%, Der p. 83% Irapuato Der p. 70% and Der f. 60% Tampico Der p. 1 55% |
| Martínez et al. [11] | 2010 | 334 | Mexico City | 56.6% to 1–4 mites (Der p., Der f., Blo t, Der s) |
| Larennas-Linnemann et al. [12] | 2011 | 4169 | Multicenter | Der p. 46–70% |
| Ramírez-Heredia et al. [13] | 2013 | 150 | Mexico City | Der p. 82.1%, Der f. 71.5% |
| Lopez-Rocha et al. [14] | 2014 | 672 | Mexico City | Der p. and Der f. 72.2% |
It is well known that there are differences in the percentage of positivity reported depending on the region where the test is applied, climate, and geography, as well as the technique used, the allergen extracted, and its strength. Most studies reported in Mexico on the sensitisation to mites are cross-sectional studies with the exception of the study by Meza-Velázquez et al. where a review of 2000 records of children with asthma or allergic rhinitis over a 10-year period was included.
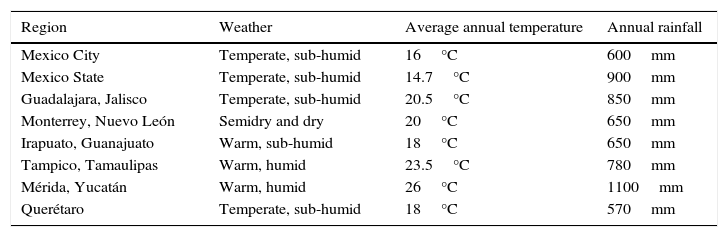
Mexico is located in the American Continent, in the northern hemisphere; comprising 1.9 million square kilometres of land area, with a climate from warm to cold, however, temperatures range from 10°C to 26°C in 93% of the territory15 (Table 2).
Climatic characteristics of some regions of Mexico.
| Region | Weather | Average annual temperature | Annual rainfall |
|---|---|---|---|
| Mexico City | Temperate, sub-humid | 16°C | 600mm |
| Mexico State | Temperate, sub-humid | 14.7°C | 900mm |
| Guadalajara, Jalisco | Temperate, sub-humid | 20.5°C | 850mm |
| Monterrey, Nuevo León | Semidry and dry | 20°C | 650mm |
| Irapuato, Guanajuato | Warm, sub-humid | 18°C | 650mm |
| Tampico, Tamaulipas | Warm, humid | 23.5°C | 780mm |
| Mérida, Yucatán | Warm, humid | 26°C | 1100mm |
| Querétaro | Temperate, sub-humid | 18°C | 570mm |
Source: Instituto Nacional de Estadística y Geografía México. Available on: http://www.cuentame.inegi.org.mx.
The prevalence of allergic diseases is increasing, but we do not know if, in terms of desensitisation, the same occurs as well, mainly to indoor allergens such as the house dust mites. The objective of this study was to determine the annual frequency and analyse changes in the sensitisation to Der p. in children treated in our hospital and compare these frequencies with different reports from Mexico.
Patients and methodsA retrospective study was conducted in the Allergy and Clinical Immunology Department of the hospital, which included the data collection of skin test results to Der p. carried out by physicians and laboratory technicians from January 2004 to April 2015. We recruited all patients aged 2–18 years old who presented for evaluation of any type of allergic condition and those who required a skin prick test (SPT) according to ongoing guides. After the clinical history and review by a certified allergist and immunologist, subjects who met the criteria had the skin test performed to inhalants (previous consent and assent signed), among which this indoor allergen was included. Patients came principally from Mexico City, Estado de México, and surrounding areas. Demographic information for all patients was reviewed as well as the referring diagnoses. This study was approved by the Ethics, Research and Biosafety Committees from HIMFG (protocol number HIM/2015/045) following the rules of the institution.
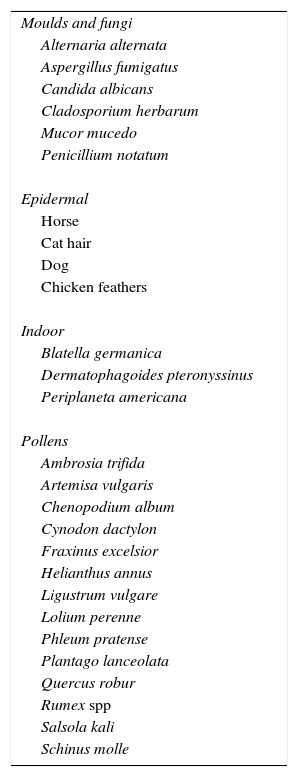
Skin tests were done during the entire time of the study with IPI Assac® extracts which have been standardised in the same way since 1999 and commercialised as UBE/ml (equivalent biologic unit). We used the same protocol for skin prick test SPT suggested by the Global Allergy and Asthma European Network, The European Academy of Allergy and Clinical Immunology and The American Academy of Allergy, Asthma and Immunology (AAAAI).16,17 Allergen extracts were stored at +2 to +8°C when not in use. Before the SPT, we recorded medications taken by the patient in the previous week to avoid false positives. Tests were applied on the upper back or in the volar aspect of the forearm, at least 2–3cm apart from the wrist and the antecubital fosase; histamine (10mg/ml) and saline solutions were used as positive and negative controls, respectively, in each patient. We previously marked the skin area with a pen, tests were placed 2cm apart from each other. A drop of each test solution was placed on the skin in identical order for all subjects tested and immediately pricked with a single-head metal lancet, without causing bleeding. Results were recorded after 15min. The largest and perpendicular diameter of the wheal was measured and the following value calculated: largest+perpendicular diameter/2. A wheal ≥3mm was considered to be a positive reaction with respect to the negative control. Each panel was comprised of a total of 27 environmental allergens, which included six moulds, four extracts from animal skin, 14 pollens including seven weeds, three grasses, and four trees, as well as cockroach and mite extract (only Dermatophagoides pteronyssinus – Der p. was used) (Table 3).
Panel of 27 airborne allergens tested.
| Moulds and fungi |
| Alternaria alternata |
| Aspergillus fumigatus |
| Candida albicans |
| Cladosporium herbarum |
| Mucor mucedo |
| Penicillium notatum |
| Epidermal |
| Horse |
| Cat hair |
| Dog |
| Chicken feathers |
| Indoor |
| Blatella germanica |
| Dermatophagoides pteronyssinus |
| Periplaneta americana |
| Pollens |
| Ambrosia trifida |
| Artemisa vulgaris |
| Chenopodium album |
| Cynodon dactylon |
| Fraxinus excelsior |
| Helianthus annus |
| Ligustrum vulgare |
| Lolium perenne |
| Phleum pratense |
| Plantago lanceolata |
| Quercus robur |
| Rumex spp |
| Salsola kali |
| Schinus molle |
Note: For the purposes of this review we only show the Dermatophagoides pteronyssinus results.
For the purposes of our goals, descriptive statistics were carried out to obtain a frequency and 95% CI of immediate hypersensitivity tests to Der p. analysed by intra- and intergroup χ2 with reported frequencies as in other studies in the country. We also analysed the differences that occurred in each during the 11 years studied.
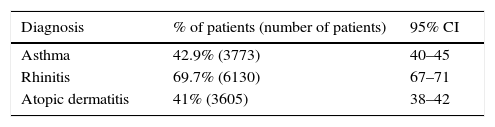
ResultsA total of 8794 patients were included with ages between 2 and 18 years old with a mean of 7.9 years (±3.7); 41.6% of the patients (95% CI 40–42) were from Mexico City, 51.6% Estado de México (95% CI 50–52) and 6.7% came from the remaining areas of Mexico (95% CI 6–7). The most frequent diagnosis was rhinitis (69.5%). Table 4 shows the distribution of the patients according to diagnosis where we can observe the overlap of these diseases as expected in atopic patients.
Distribution of patients according to reported diagnosis (n=8794).
| Diagnosis | % of patients (number of patients) | 95% CI |
|---|---|---|
| Asthma | 42.9% (3773) | 40–45 |
| Rhinitis | 69.7% (6130) | 67–71 |
| Atopic dermatitis | 41% (3605) | 38–42 |
Note: The diagnoses were made by a paediatric allergist according to ongoing guides:
Global Initiative for Asthma (GINA).
Allergic Rhinitis and its Impact on Asthma (ARIA).
Disease management of atopic dermatitis: Practice Parameter.
No differences found in patients’ gender.
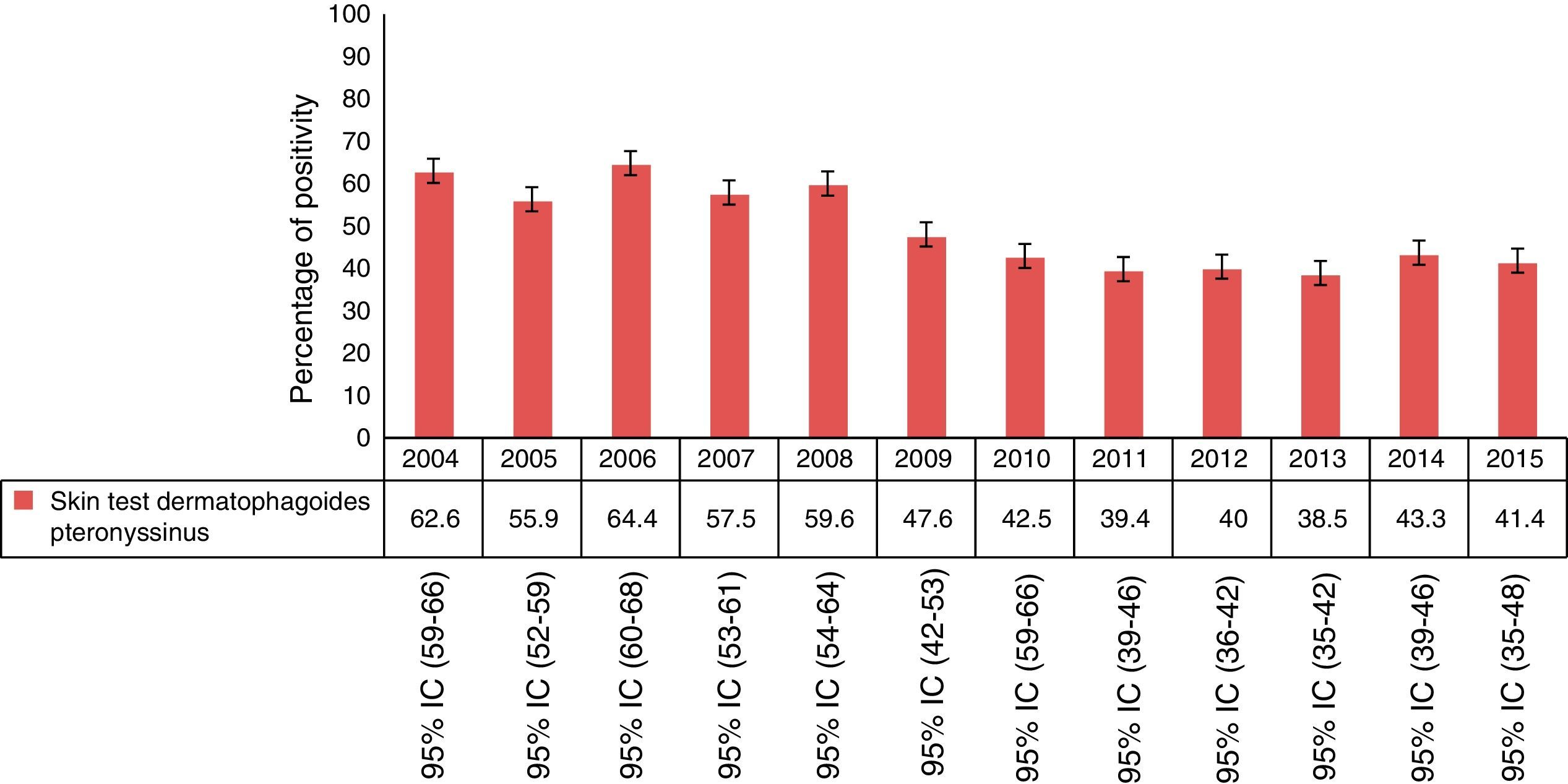
Within 8794 tests, 14% (95% CI 13–14.8) were negative to the entire panel and of the remaining 7565 tests, 49.3% (95% CI 48–50) were positive for Der p., of which 2.7% (95% CI 2–3) were monosensitised (Der p.). The year with the highest percentage of sensitisation was 2006. Analysis of the results of positive skin tests for each year is shown in Fig. 1.
. 2004 n=718, 2005 n=870, 2006 n=641, 2007 n=653, 2008 n=379, 2009 n=319, 2010 n=759, 2011 n=769, 2012 n=646, 2013 n=788, 2014 n=801, 2015 n=222. Note: For this analysis we only included patients with at least one positive SPT.")
Percentage of skin test positivity to Dermatophagoides pteronyssinus by year (n=7565). 2004 n=718, 2005 n=870, 2006 n=641, 2007 n=653, 2008 n=379, 2009 n=319, 2010 n=759, 2011 n=769, 2012 n=646, 2013 n=788, 2014 n=801, 2015 n=222. Note: For this analysis we only included patients with at least one positive SPT.
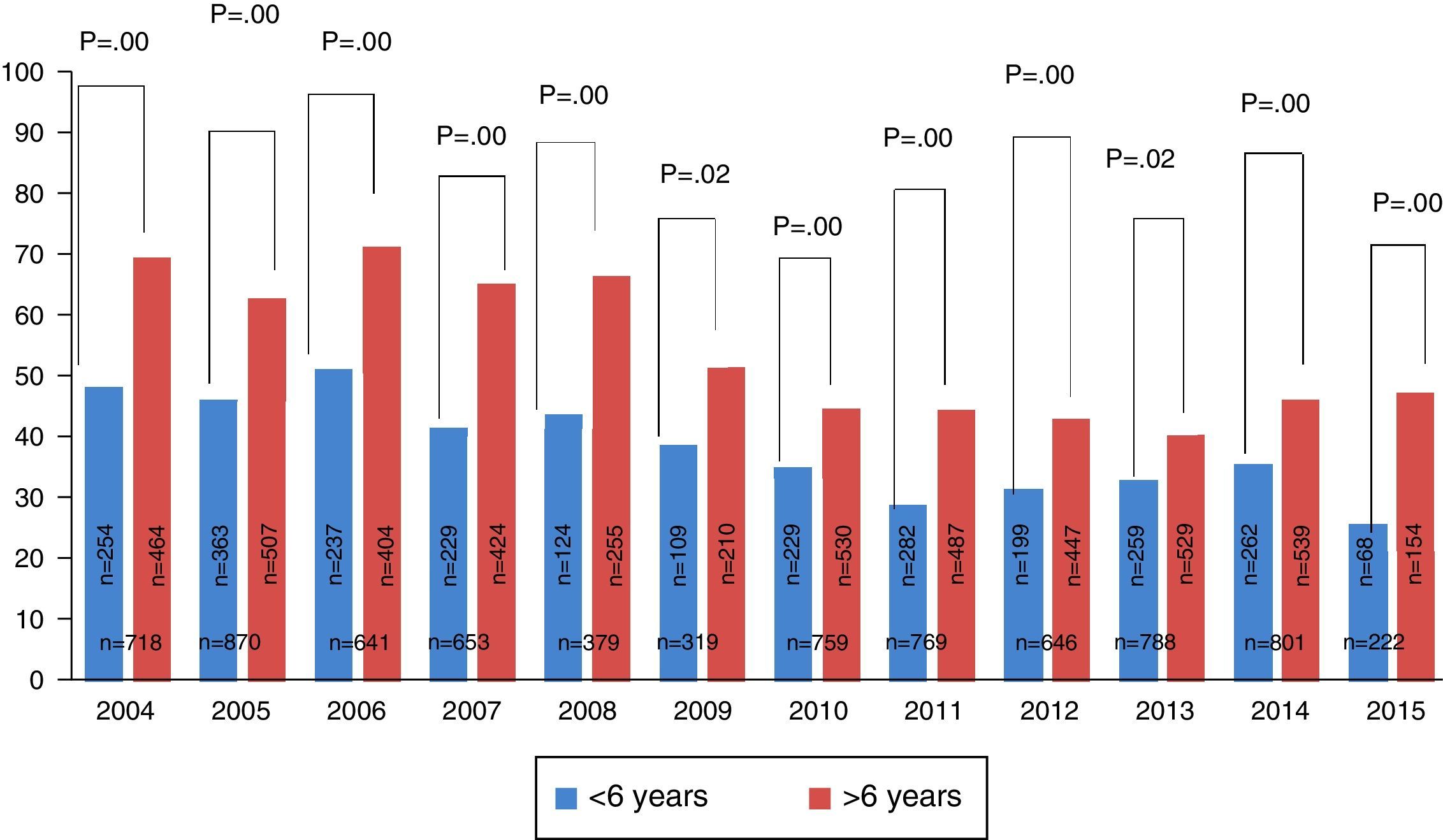
Of the tests conducted during the study, 34% (95% CI 33–35) were performed in children <6 years old, of whom 39% (95% CI 37–41) were positive for Dermatophagoides pteronyssinus. When the group of children >6 years old was studied, we found that the overall percentage of sensitisation was 54% (95% CI 52–55). Comparison between these groups was statistically significant (p=0.000). In all the years studied, we found a higher proportion of positive tests in children >6 years old (Fig. 2).

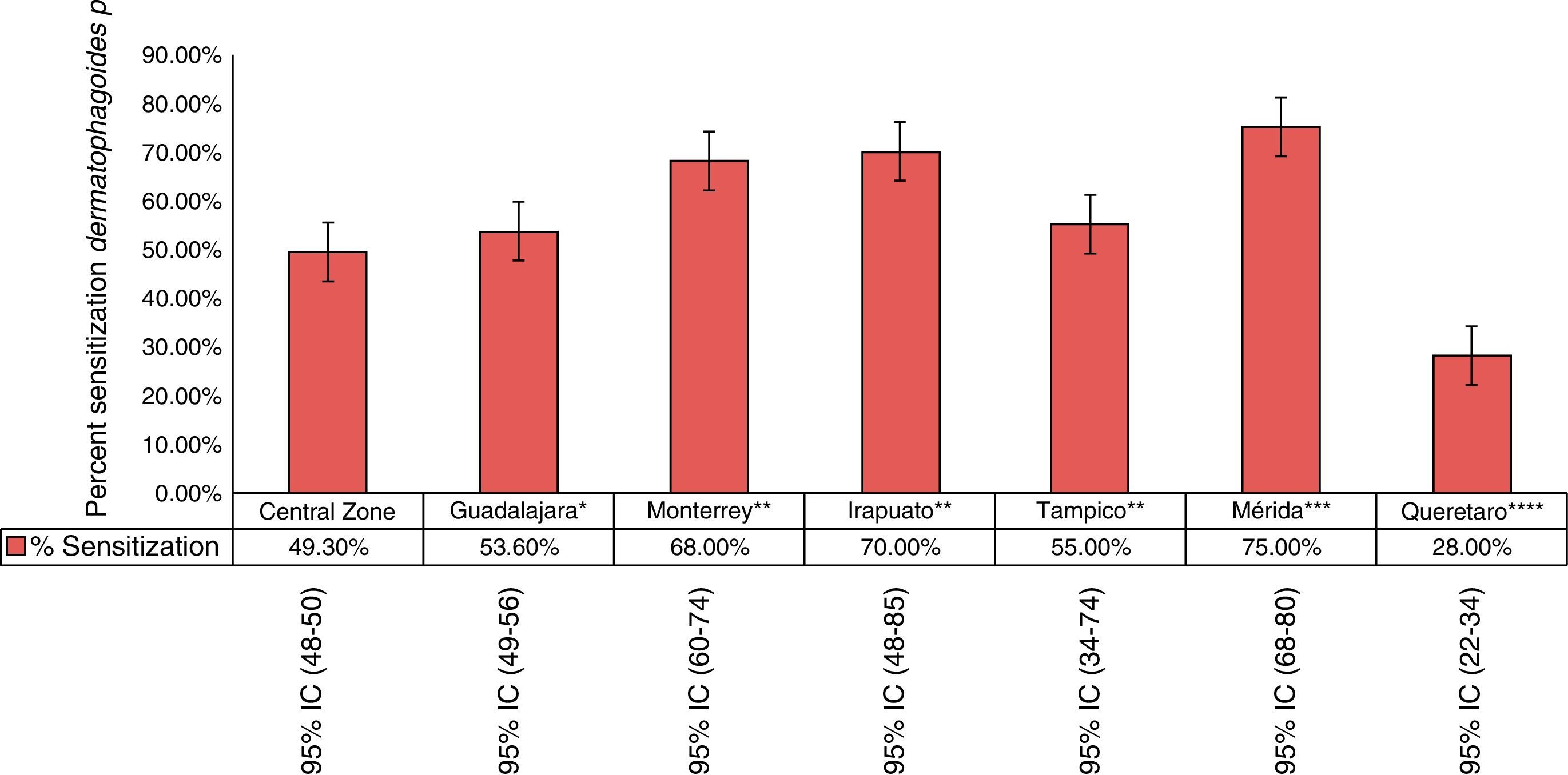
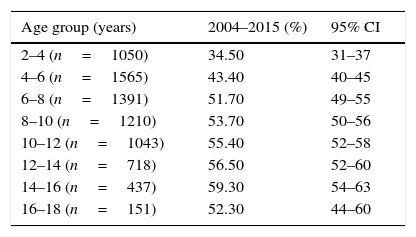
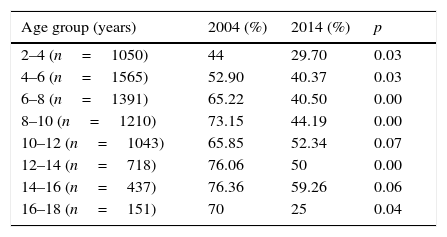
Stratifying the group, it was found that the ages with the highest percentage of sensitisation were 14–16 years old. From 6 to 18 years old, 50% of the children were sensitised to Dermatophagoides (Table 5). When compared by age and by years we found a general decrease in the sensitisation percentage in all ages (Table 6). In the rest of Mexico, the highest percentages were reported in Merida with 75% (95% CI 68–80%) followed by Monterrey and Irapuato. In the study by Larennas12 a lower reactivity was reported in Queretaro (28%) (Fig. 3).
Percentage of sensitisation to Dermatophagoides pteronyssinus separated according to age in the study population (n=7565).
| Age group (years) | 2004–2015 (%) | 95% CI |
|---|---|---|
| 2–4 (n=1050) | 34.50 | 31–37 |
| 4–6 (n=1565) | 43.40 | 40–45 |
| 6–8 (n=1391) | 51.70 | 49–55 |
| 8–10 (n=1210) | 53.70 | 50–56 |
| 10–12 (n=1043) | 55.40 | 52–58 |
| 12–14 (n=718) | 56.50 | 52–60 |
| 14–16 (n=437) | 59.30 | 54–63 |
| 16–18 (n=151) | 52.30 | 44–60 |
Note: For this analysis we only included patients with at least one positive SPT.
Comparison of the percentage of sensitisation to mites separated by age in 2004 vs. 2014 (n=7565).
| Age group (years) | 2004 (%) | 2014 (%) | p |
|---|---|---|---|
| 2–4 (n=1050) | 44 | 29.70 | 0.03 |
| 4–6 (n=1565) | 52.90 | 40.37 | 0.03 |
| 6–8 (n=1391) | 65.22 | 40.50 | 0.00 |
| 8–10 (n=1210) | 73.15 | 44.19 | 0.00 |
| 10–12 (n=1043) | 65.85 | 52.34 | 0.07 |
| 12–14 (n=718) | 76.06 | 50 | 0.00 |
| 14–16 (n=437) | 76.36 | 59.26 | 0.06 |
| 16–18 (n=151) | 70 | 25 | 0.04 |
Note: For this analysis we only included patients with at least one positive SPT.
. n=752 patients with rhinitis 16–78 years old.18 **Cavazos-Galvan et al. (2008) n=58 patients 27–31 years old.10 ***Baeza M. 2005 n=176 patients with rhinitis and/or asthma 2–5 years old.19 ****Larenas-Linneman et al., 2011 n=4169 2–65 years.")
Comparison of the sensitisation to Dermatophagoides p. in different centre in Mexico. *Bedolla et al. (2010). n=752 patients with rhinitis 16–78 years old.18 **Cavazos-Galvan et al. (2008) n=58 patients 27–31 years old.10 ***Baeza M. 2005 n=176 patients with rhinitis and/or asthma 2–5 years old.19 ****Larenas-Linneman et al., 2011 n=4169 2–65 years.
Indoor allergens represent one of the most important factors in causing allergic diseases as well as in arousing symptoms. From these, house dust mites have been considered as the most important factor associated with rhinitis and asthma.
Sensitisation to house dust mites is common and relatively constant; however, there are two important factors that have an influence on this sensitisation: the first corresponds to the geographic variation of the region studied and includes: weather, vegetation, altitude, etc.; the second corresponds to the characteristics inherent to the population: socioeconomic status, activity, exposure, etc. With this, we can understand why a different prevalence of sensitisation is reported in different populations, even in the same country and in the same city. An example of this is the prevalence reported in Europe and Asia—up to 75.5% in Israel,20 52.8% in Korea21 and 19.2% in the UK.22 In Latin America, a sensitisation—in decreasing order—of 82.1% in Argentina,23 76.9–81.5% in Cuba,24 80% in Chile25 and 69.9% in Ecuador.26 Another important point to understand when the sensitisation to house dust mites is studied, is the change in climate and air quality that has occurred the past years and it impacts not only on morbidity, but also on mortality of patients with allergic diseases.27 Different authors have attempted to show the effect that this climate change has had on the sensitisation of patients with allergic diseases by examining differences between population groups.
We reviewed the results of skin tests; therefore, our study provides valuable information about the variations in the frequency of sensitisation throughout this period. The study found a higher frequency of sensitisation to Dermatophagoides pteronyssinus in patients 6–16 years old compared with younger and older ages, the decision of selecting a cut-off of six years of age was made based on Moral et al.,28 who report an increase of mites sensitisations after six years old, our results are similar to this author who found a progressive increase in sensitisation which ranged from 16% at 0–2 years to 87% at 6–14 years.28 Subsequently, this trend inverts itself with a gradual decrease in the reactivity according to age, with lower values demonstrated close to 70 years of age.22 However, there are reports about the cut-off age in which this change in the pattern of sensitisations takes place. Dottorini29 and Pallasaho30 found, in a cohort of patients 14–64 years of age, that the decrease occurred after the fifth decade of life, whereas other authors showed a decrease at 30 years of age.31 Those investigators, who studied populations that included children as well as adults, found cut-off values even lower at ∼14 years old,32 similar to our results.
Another important point is that we found a decrease in general sensitisation to mites in the group >10 years old, both in the analysis group and the group stratified by ages. Warm33 and Francis34 obtained similar information in comparisons carried out from 1999 to 2009 and from 1986 to 2001, respectively; however, these results are not reproduced in all series such as the Copenhagen Allergy Study,35 which found an increase from 12.2 to 14.1% in the frequency of positive tests to this indoor allergen between 1990 and 1998 in subjects 15–41 years old and in the study by Ronmark36 who also reported an increase in sensitisation from 0.5 to 1.4% from 1996 to 2006. These differences can point to diverse factors such as the ages of the group included and type of allergens used, because in some series the extract varied from one year to another. In this regard, the fact of having used the same extracts with a relatively similar population represents a strength of our study.
We found a decrease in sensitisation prevalence in the group of 16–18 years old from 2004 to 2014 as in all patients, but we saw this trend exacerbated in this group, perhaps as we said, it is a trend manifested in all groups we recognised this specifically group has less participants.
When compared with similar studies in the rest of the country, we see variations in sensitisation according to the location where the tests were performed, type of extract used and the study population. Locations in Mexico with the greatest sensitisation were (in descending order) Merida, Irapuato, Monterrey and Queretaro. In our case the percentage of positivity corresponds to an intermediate value compared to the rest of Mexico. This is explained by the diversity of the population we have in our institution. We only review the frequency of Dermatophagoides pteronyssinus sensitisation, and perhaps this is a study limitation; according to Fernández-Duro et al., who evaluated the mite species found in Mexican homes of different regions, Dermatophagoides pteronyssinus is the predominant mite and was found in 100% of the samples.
Finally, we found that the frequency of sensitisation to Dermatophagoides pteronyssinus increases with age until adolescence. In the past 11 years there has been a general tendency to a decrease in sensitisation to this indoor allergen in our population.
Ethical disclosuresConfidentiality of dataThe authors declare that they have followed the protocols of their work centre on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consentThe authors have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence is in possession of this document.
Protection of human subjects and animals in researchThe authors declare that no experiments were performed on humans or animals for this investigation.
FundingNo external funding sources were used for carrying out this study.
Conflict of interestThe authors declare no conflict of interest.
The authors thank Maria de Lourdes Lerma Ortiz (chemist), Allergy Laboratory, Hospital Infantil de México Federico Gómez, for excellent collaboration.
