


INTRODUCTION
Bronchial asthma is a chronic disease with high prevalence during childhood, being the leading cause of hospital admission in children with chronic disease1-3.
It is a major cause of absenteeism with repercussions on quality of life, and a high socio-economic impact, for which it should be considered as a Public Health problem2,3.
In order to know the prevalence of allergic disease worldwide an international project involving more than 150 countries has been developed during the last ten years. This is the International Study of Asthma and Allergies in Childhood (ISAAC), which comprehends 3 different phases. Phase I was designed to know the prevalence and severity of asthma and other allergic diseases (rhinitis, eczema) worldwide, using questionnaires; Phase II was designed to study etiological factors, evaluating bronchial hypereactivity and atopy, and finally Phase III which was a repetition of Phase I in order to verify the evolution of those diseases regarding their prevalence4-6.
This multicentric study aimed to study the prevalence of allergic diseases in children of two different age groups: 6-7 and 13-14 years old, using questionnaires and videos (for the younger ones)5,6.
The higher prevalence was obtained in Great Britain, New Zealand and Australia, and the lower in China and Indonesia, with an intermediate position for Portugal (Phase III: Actual asthma- 12,9 %: 6-7 yrs old/ 21,8 %: 13-14 yrs old)5-8.
Castelo Branco is a portuguese countryside town with 70.000 inhabitants and 7,7 newborn/1000 inhabitants. There are no studies about the prevalence of asthma in these region of Portugal.
School absenteeism has been commonly used as a marker to evaluate the social repercussions due to asthma, with a large number of studies proving to be higher among asthmatics comparing to healthy children1,7,9.
Chronic diseases may affect self-esteem and cause familiar conflicts10. It is accepted the association between severe asthma and anxiety, depression and lower self-esteem11.
Their families tend to adopt an attitude that limits the child physical activity and overprotection rising in their children feelings of anger and denial of the disease12.
Asthma has implications on children's life in several domains such as physical, psychological and social areas, disturbing their development and the construction of their personality and self-concept12,13.
The evaluation of Self-concept has been proposed as an important tool to achieve a global impression of a subject's personality12-14.
There are several scales and models to evaluate it, underlying different models and conceptions of Self-Concept, which can be divided in unidimensional and multidimensional15-18.
The unidimensional models define Self-Concept as the sum of several specific competences regardless the analysed competence (Coopersmith Self-Esteem Inventory or Piers-Harris Self-Concept Scale) while the multidimensional ones consider the existence of interrelation and hierarquization between specific domains19,20.
The authors used the Self-Concept Scale of Susan Harter based on a multidimensional model, in which there are five specific domains that contribute to Self-Concept and an independent and superior domain: Self-esteem. This scale is adapted for children in school age22-24.
The five specific domains are: School competence, Athletic Competence, Social Acceptance, Physical Appearance and Behaviour, interdependent between them24.
It is assumed that although a child might have a low perceived competence in one specific domain it might not interfere with the global self-esteem because it might be a domain not considered important to the child24.
Among the specific domains, School Competence is highly related to Behaviour and the remaining domains are highly related between them24.
Physical appearance is the specific domain most related with Self-Steem in opposition to Athletic Competence, even in specific groups such as athletes or brillant students, being present after 4 years old, particularly in girls24.
It is very important to evaluate Self-Concept in children with chronic diseases to perceive lower competences in specific domains and establish individual programs to improve them and make possible a healthy construction of personality as well as integration with their peers.
The purpose of this study was to calculate the prevalence of asthma in a Portuguese countryside town among all children of the 5th-6th grade in school and to establish the possible correlation of its presence on absenteeism and self-concept.
MATERIAL AND METHODS
Our study population included 950 children whose ages ranged from 10 to 15 years old, in a countryside town in Portugal: Castelo Branco. This population corresponds to all students at 5th and 6th grades in the city.
Informed consent has been obtained from parents of all children participating in this study, after authorization of the four participating schools.
The researchers have been present during all days of research.
We used the portuguese version of International Study of Asthma and Allergies in Childhood's (ISAAC) questionnaire to know the prevalence of asthma, using the specific page of questions regarding asthma evaluation, in a total of 8 questions, comprehending questions to know the prevalence as well as the severity of the disease. Each question has two options for answer: Yes/No, with exception of those referring to severity of the disease5,6.
The Susan Harter's Self-Concept Scale has been used to evaluate Self-Concept. This is a scale composed by 36 questions, with 6 questions for each specific domain (School Competence, Athletic Competence, Social Acceptance, Physical Appearance and Behaviour) and 6 questions to evaluate Self-esteem. Each question has four options for answer. The child has to decide, between two statements presented for each question, in which statement recognises more similarities to herself, and after that to decide if that similarity is total or partial. To each domain, 3 questions start with positive questions referring to high-perceived competence and the remaining three the other way around. The questions for each domain are distributed along the questionnaire. There is a final score for each domain, obtained after making the sum of scores in all 6 questions for each domain. The questions starting with positive statements are classified with 4-3-2-1 points, sequentially and the negative questions, the opposite way24.
The researcher spent two days at each school. The questionnaires have been distributed collectively in each classroom. All children had 5 minutes for the ISACC questionnaire and 20 minutes for the scale of Susan Harter. The researcher briefly explained the procedures to answer to both questionnaires, before distributing them. He has been present in every classroom during the study.
The information regarding absenteeism has been recruited by analysing school records. Demographic data (age, sex) were written on the questionnaires sheets. Each child had a code number. All information and questionnaires were anonymous.
The statistical analysis was performed by SPSS/PC (Version 10-2000), SPSS, Inc., USA. Pearson's correlation was used for the association of intervalar data, chi-square test to analyse the association of categoric data, and the nonparametric Kruskall-Wallis test for the association of categoric and continuous data. Statistical significance was accepted at p ≤ 0,05.
The present study was done during 2002, namely the data collection in April (field research) and the following analysis from May till November.
RESULTS
Prevalence of Asthma
We evaluated 818 children (399 girls, 419 boys) from the initial population (950), corresponding to 86,1 % of participation in the study. The mean age was 11 years old (10-15 years) and a M/F ratio of 1/1.
The prevalence of cumulative asthma was 11,86 % (table I), with a higher prevalence in male, with a statistical difference between sex (Kruskall Wallis: p = 0,008).
Among asthmatic children the median age was 11,34 years old (SD: 1,26). The majority of them (74 %) had symptoms during the last 12 months, being the prevalence of current asthma 8,8 %. Regarding the severity of asthma, 74 % of children with current asthma had 1 to 3 attacks during the last year and 30 % had nocturnal symptoms (including cough).
Absenteeism
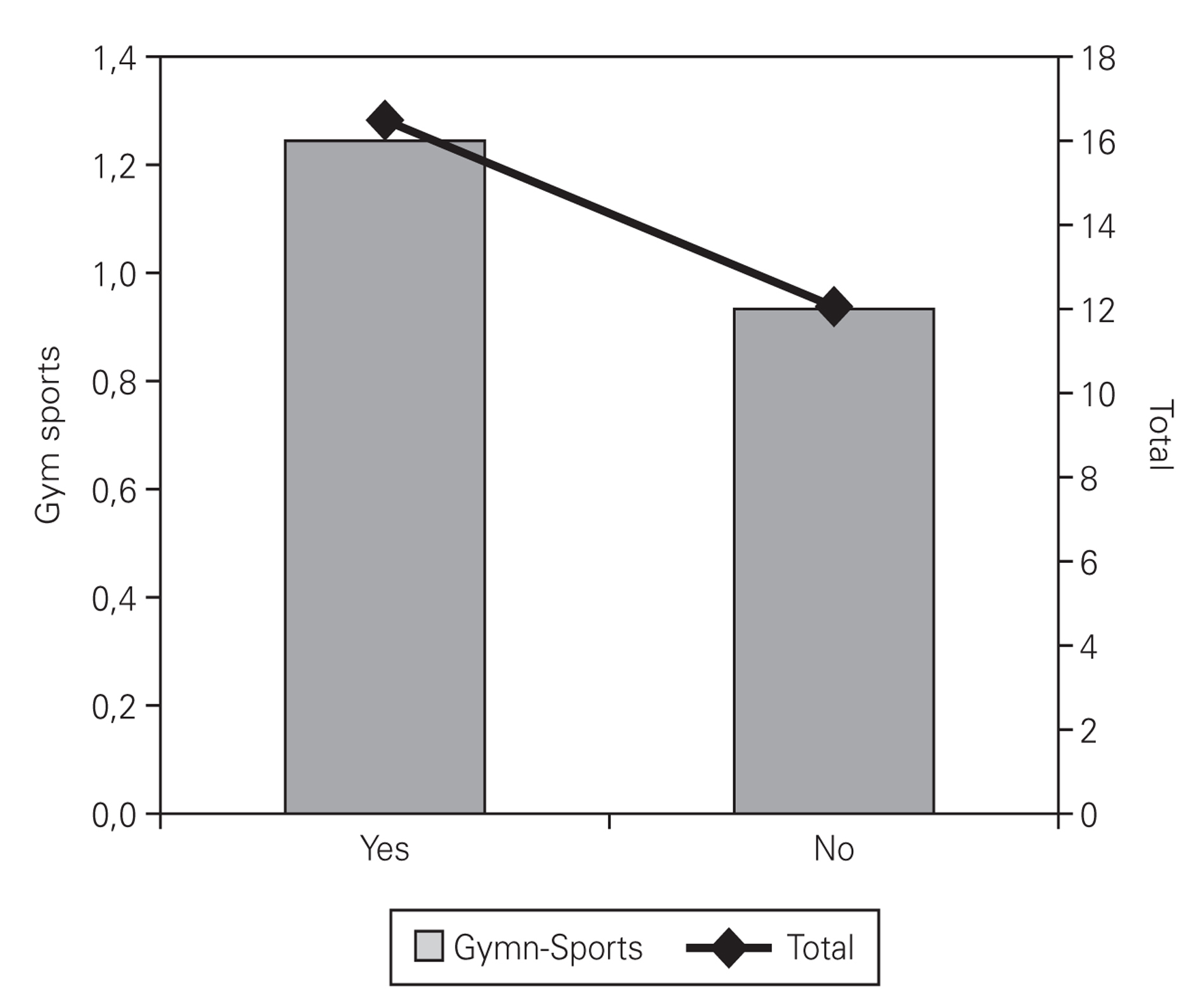
Asthmatic children had a higher absenteeism (5 days in average), statistically significant for all disciplines (p = 0.05) and for Gymnastic and Sports (p = 0.04), comparing to the remaining population (fig. 1), with girls having higher absenteeism than boys.

Figure 1.--Absenteeism distribution according to the presence of asthma in all disciplines and in Gymnastic and sports. Kruskal-Wallis, p = 0.05 (Gym-Sports) e 0.04 (Total).
Self-Concept
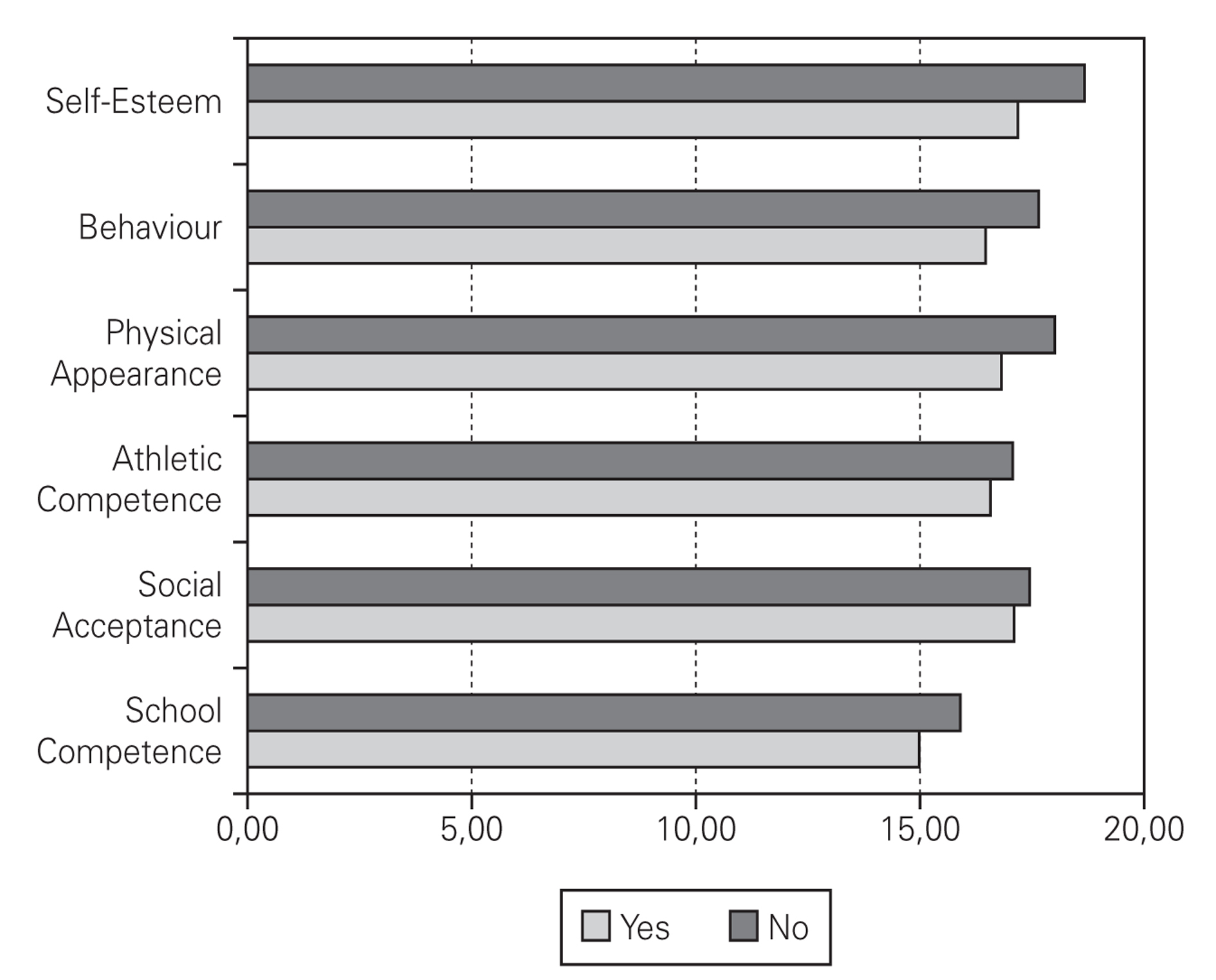
Regarding the analysis of Self-Concept, asthmatic children had lower scores in all specific domains (School Competence, Athletic Competence, Social Acceptance, Physical Appearance and Behaviour) as well as in Self-esteem, comparing to healthy ones, with the higher difference between them at Self-esteem and the lowest difference at Social Acceptance (fig. 2).

Figure 2.--Self-Concept scores using Susan Harter scale according to the presence of asthma.
The lower scores in asthmatic children were statistically significant in School Competence, Physical Appearance, Behaviour and Self-esteem (table II).

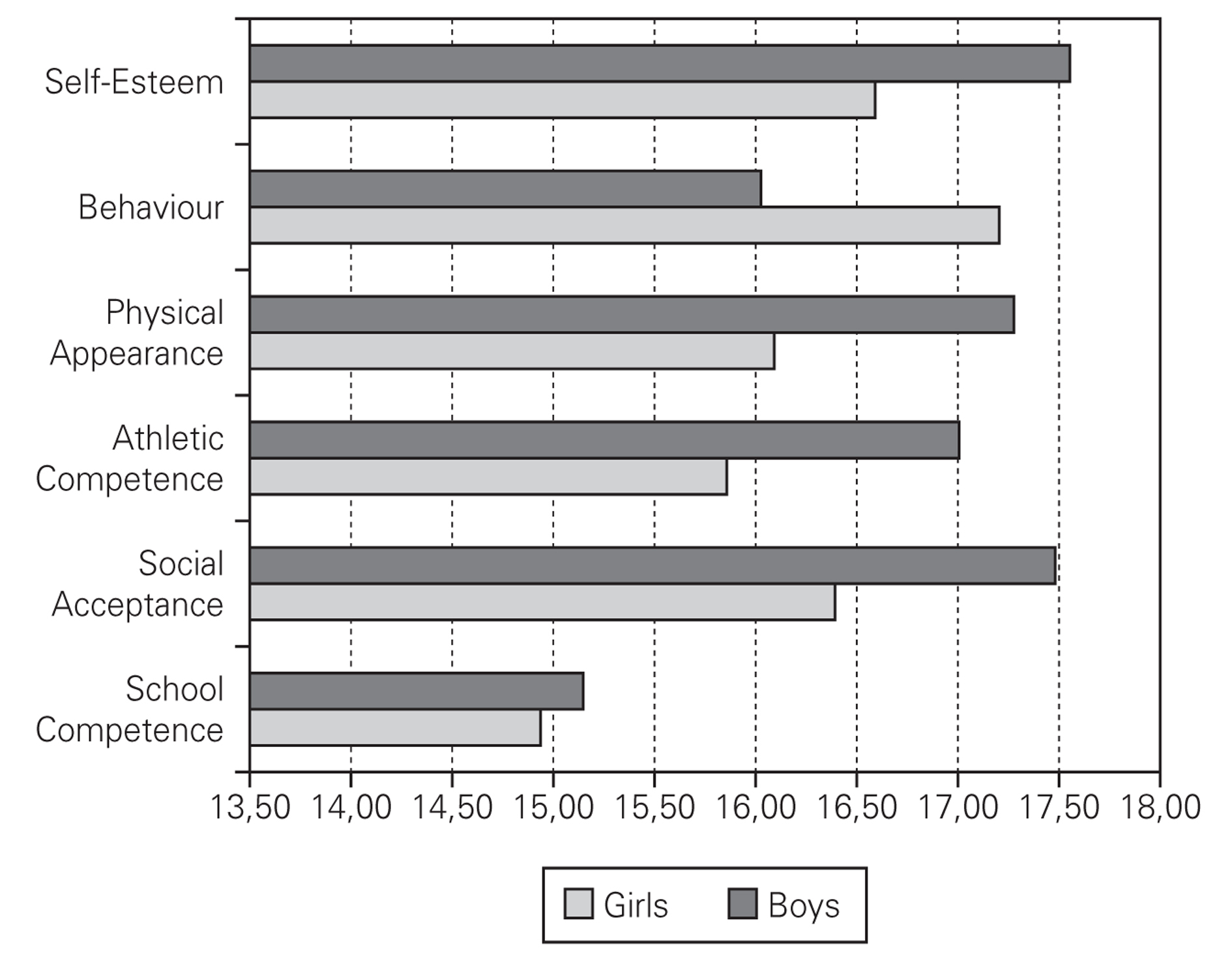
Among asthmatic children, as well as in total population, boys had higher scores than girls in all domains of Self-Concept with exception of Behaviour. Those differences had maximum expression on Physical Appearance scores (fig. 3), and were statistically significant (p = 0,04).

Figure 3.--Self-Concept scores using Susan Harter's scale, according to sex, in asthmatic children.
There were no statistically significant differences on Self-Concept domains between children with and without current asthma (0,08 ≤ p ≤ 0,96).
DISCUSSION
The cumulative prevalence of asthma was 11,9 %, being 8,8 % the prevalence of current asthma, enhancing this disease as one of the most frequent chronic diseases in children. To calculate the prevalence of asthma, we used the ISAAC questionnaire. This instrument is commonly used internationally, allowing the comparison of different populations in different countries.As expected, the obtained data are lower than data from New Zealand, England or Australia, and higher than the ones from China or Indonesia5,6.
The response rate was 86,1 %. It can be considered a reliable rate comparing to the commonly 80 % achieved in a large number of countries participating in the ISAAC project5,6.
Although the previous data were supported by a previous study made in Portugal by Rosado Pinto et al (1996), in several portuguese cities (Lisbon, Coimbra, Porto, Portimão, Funchal) using the same methodology in children between 13-14 years old25,26. These authors stress the raise of prevalence of asthma in Portugal during the last years, as previously quoted, which lead us to consider the disease as a major public health problem.
More updated results regarding the ISAAC project phase III (2002), report higher levels for cumulative asthma (21,8 %) as well as for current asthma (11,8 %), among children with 13 to 14 years old, in Portugal27.
In the referred age group, the obtained data are lower than the national average (cumulative: 21,8 %; current: 11,8 %), as well as lower than data obtained from different Portuguese cities by the seaside, such as Lisbon (current: 14,6 %), Portimão (cumulative: 18,2 %; current: 9,7 %), Porto (cumulative: 22,1 %; current: 13,1 %), Madeira (cumulative: 19,3 %; current: 9,0 %) or in the countryside such as Évora (cumulative: 19,8 %; current: 12,8 %)27.
In all studies there was a higher prevalence of asthma in boys, similarly to what we obtained in this study.
The majority of children (74 %) had mild asthma (1-3 attacks), as it is commonly accepted in international studies and in accordance to published data by Mario Morais Almeida et al, in ISAAC study phase II in Lisbon (70 %). Regarding nocturnal symptoms, including cough, the obtained data (30 %) are similar to the ones obtained in ISAAC study phase III in all cities mentioned earlier27.
In our study, asthmatic children had higher absenteeism than their peers, in average 5 days, namely in boys. This differrence was statistically significant.
The obtained results are supported by some studies but not by other ones. In fact, in 1998 a study made in United States of America including 7465 children, from 10 to 17 years old, concluded that asthmatic children had in average 4,6 days of absenteeism per year due to their disease. This was higher than the absenteeism of healthy children12.
By contrast, a study made in Scotland in 10868 children from 1-15 years old, found no differences among asthmatic children compared to healthy ones, despite using a similar metodology of the study mentioned above9.
During 1998 a study made by Leiria Pinto et al in a Portuguese countryside town Lourinhã, concluded that among 1879 children, half of the asthmatic ones had in average 6 absent days per year28.
According to Professor Bousquet at ARIA (Impact of Allergic Rhinitis on Asthma) the majority of patients with asthmahave rhinitis, which in conjunction may conduce to impairment of quality of life and higher absenteeism year29.
Paul Cawenberg, also estabilishes the relation between asthma and allergic rhinitis, and their relation to impairment of quality of life and absenteeism30.
There are no studies in Portugal regarding the relation asthma-self-concept, using the multidimensional model of Susan Harter, which gives a unique characteristic to the present study.
The obtained data, with lower scores for asthmatic children than healthy ones, are in accordance to published studies31-35, particularly in Physical Appearance36. Nevertheless, other studies found no differences between groups37.
Among healthy children Physical Appearance is the specific domain with higher scores revealing the importance attributed to this domain during adolescence. It is well know the importance of appearance in modern societies, particularly for teenagers, once the acceptance inside a group among peers depend on it.
Asthmatic children tend to be less developed achieving puberty later than healthy ones38,39, which has tremendous implications on their physical perception and self-esteem, domains traditionally connected in all children since 4 years old, even in special groups such as athletes, as mentioned previously, explaining the lower scores obtained and the biggest difference between them in this domain24.
Regarding the lower scores obtained for School Competence, the authors enhance the presence of mild asthma, usually neglected by children and respective parents regarding the need for treatment, as well as the nocturnal symptoms, which, in combination may lead to attention disorders, particularly during morning compromising the intellectual skills. Moreover the higher absenteeism compromises the educational commitment40.
As mentioned before, Paul Cawenberg states that the majority of asthmatic children have rhinitis, being the former responsible for sleep disturbances and daytime fatigue, leading to intellectual and attention impairment30, which may compromise the learning process.
Another possible explanation was the tendency for asthmatic children to be more demanding with themselves regarding intellectual skills once they have physical limitations in the presence of uncontrolled asthma.
The classical association of School Competence and Behaviour, as well as for the possible tendency to anger and denial facing an uncontrolled disease with feelings of inferiority, disability and stress may lead to lower Behaviour scores24.
There were no statistical differences regarding Athletic Competence and Social Acceptance, domains usually linked, according to Susan Harter24.
Asthmatic children's families and teachers usually spare them to do physical exercise leading to the common neglect of the importance of physical skills, explaining way this specific domain isn't valorised by them. They assume that they shouldn't be compared with healthy children regarding athletic skills and therefore any skill achieved is best valorised. Another possible explanation is that asthmatic children are usually encouraged to swim since infancy achieving high scores in this sport during Gym classes31,34,36,41.
As expected, boys have higher scores in all specific domains as well as in Self-esteem, except in Behaviour. It is not surprisingly at all, once boys usually have worse behaviour than girls, and it is usually expected to be so24,34,41.
The higher differences among sex are seen at Athletic Competence, but among asthmatic children are at Physical Appearance. The authors couldn't find any explanation for this fact in the literature.
Children with current asthma had no differences regarding to Self-Concept scores, comparing to the remaining asthmatics, which can be explained by the fact that the construction of self-concept takes several years, as it is a long process, not being so much affected by recent events.
A positive self-concept is essential for personal happiness, adaptation among peers and success42. Children with lower self-concept, often express anxiety and relation problems35.
The knowledge of the association between personal success and self-concept as well as the effect of chronic disease on it, stress the responsibility of all health and education professionals for the need of evaluation of self-concept in children with chronic diseases in order to improve it.
CONCLUSIONS
Asthma is one of the most frequent chronic diseases in childhood and adolescence, with a high impact on absenteeism and self-concept, namely in the construction of personality. It has implications on biological, psychological and social maturation of the adolescence.
It is very important to establish intervention school programs in order to develop an in depth knowledge about asthma implications and emphasise the equality of asthmatic children comparing to healthy children, in all domains, as long as the disease is well controlled.
These programmes should include doctors, psychologists, teachers, parents, asthmatic students and their peers.
The authors stress the importance of a good understanding of the disease to allow for the real inclusion of the asthmatic children in school and society.
