




Hepatic nodules with increased portal venous flow are rare, and no distinct status has been established for them. We present here a case of idiopa-thic portal hypertension (IPH) with multiple hyperplastic nodules supplied by portal venous flow.
A 30-year-old Japanese man with esophageal varices was admitted to our hospital. Arterial phase computed tomography (CT) revealed multiple low-attenuating nodules of 2 to 3 cm in diameter in both lobes. However the contrast of the multiple nodules had become indistinct on portal phase CT. Multiple nodules showed strongly high-attenuation on CT during arterial portography (CTAP) (Figure 1A) and low-attenuation on CT during hepatic arterio-graphy. Single-level dynamic CTAP (S-CTAP) was also performed as described previously1 (Figure 1B-1E). Regions of interest (ROIs) were placed on the images of the nodules and adjacent liver parenchyma, and their density was measured and plotted to construct a time-density curve. S-CTAP clearly showed the contrast material in the small portal branches in the nodules, which spread throughout the entire nodule. The peak value of the time-density curve was 246 HU for the ROIs placed on the nodule, which was extremely high in comparison with the value on a normal parenchyma. Histologically, the nodules showed neither cellular nor structural atypia, but showed liver cell hyperplasia. Inside the nodule, dilated venous-like vessels were observed (Figure 2A). Most of them were seen to distribute in lobules without coexistence of artery or bile duct, but some were with only bile ductile by investigation of serial thin sections (Figure 2B-2D). These findings indicated that they originated from the portal vein.2
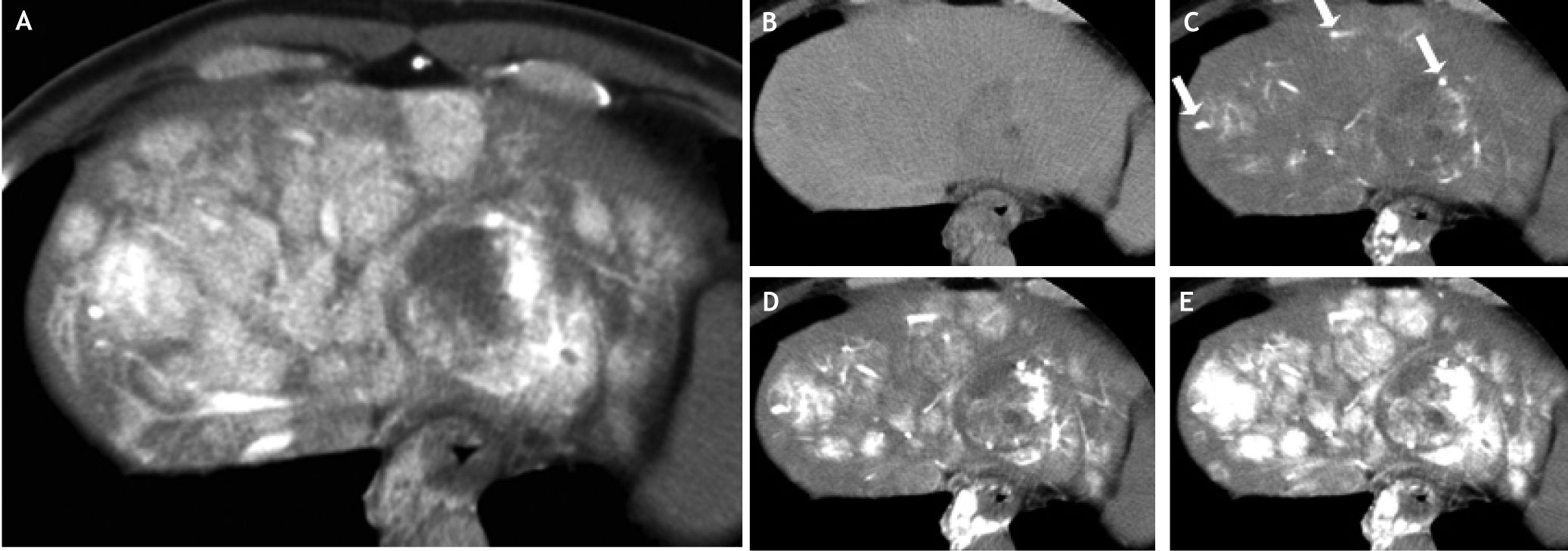
 and histopathology of the nodules. Multiple nodules showed strong high-attenuation on CTAP (A). The nodules were a few centimeters in diameter and distributed throughout the liver. Single-level dynamic CTAP images were obtained at 6 s (B), 14 s (C), 18 s (D), and 22 s (E) after injection of contrast material from the superior mesenteric artery. Within 14 s (C), the feeding vessels and partial enhancement in the nodules had become visible (arrows). The contour of the nodules became evident in 18 s (D), and the entire nodule became highly enhanced in 22 s (E).")
Single-level dynamic computed tomography during arterial portography (CTAP) and histopathology of the nodules. Multiple nodules showed strong high-attenuation on CTAP (A). The nodules were a few centimeters in diameter and distributed throughout the liver. Single-level dynamic CTAP images were obtained at 6 s (B), 14 s (C), 18 s (D), and 22 s (E) after injection of contrast material from the superior mesenteric artery. Within 14 s (C), the feeding vessels and partial enhancement in the nodules had become visible (arrows). The contour of the nodules became evident in 18 s (D), and the entire nodule became highly enhanced in 22 s (E).
![Liver biopsy specimens taken from the nodular regions showed neither cellular nor structural atypia, but did reveal liver cell hyperplasia (A-C). There were many dilated thin-walled vessels without coexistence of arteries or bile ducts. Some of them were accompanying only bile duct (B) (arrow). Some dilated vessels distributing into lobules were observed in serial sections (B-D). CD34 immunostaining showed the existence of endothelial cells on the lumens of this dilated vessels and that these were not dilated sinusoids. [H&E staining (A); Reticulin Silver impregnation staining (B); Azan Mallory staining (C); CD34 immunostaining (D)].](https://static.elsevier.es/multimedia/16652681/0000001100000004/v1_201906191936/S1665268119314760/v1_201906191936/en/main.assets/gr2.jpeg?xkr=ue/ImdikoIMrsJoerZ+w997EogCnBdOOD93cPFbanNeKOJqKH5+Za6P+RA5Vq9DlAjZTXha78JQ+5B73uOl1XbIOPCS4aaL+723pxU1HAKwxRS12Fa1HJn80K6xp93N3RxpFcXBdNkBLu33zkYD1ZULfjQEqhj0E2I2hMOMm3/QQeYteQ59Cer5ozlvhZlFyhuPV20q3ylKP6mTDFjCWZB6Gpx193xupyAoL+m4+ZtGu4/Vzf3Q3pkazB7OcyE3HVWI7cQ1Qre4s3Nk1rVwO2USTJNV8weWnjz+wQayu2G4= "Liver biopsy specimens taken from the nodular regions showed neither cellular nor structural atypia, but did reveal liver cell hyperplasia (A-C). There were many dilated thin-walled vessels without coexistence of arteries or bile ducts. Some of them were accompanying only bile duct (B) (arrow). Some dilated vessels distributing into lobules were observed in serial sections (B-D). CD34 immunostaining showed the existence of endothelial cells on the lumens of this dilated vessels and that these were not dilated sinusoids. [H&E staining (A); Reticulin Silver impregnation staining (B); Azan Mallory staining (C); CD34 immunostaining (D)].")
Liver biopsy specimens taken from the nodular regions showed neither cellular nor structural atypia, but did reveal liver cell hyperplasia (A-C). There were many dilated thin-walled vessels without coexistence of arteries or bile ducts. Some of them were accompanying only bile duct (B) (arrow). Some dilated vessels distributing into lobules were observed in serial sections (B-D). CD34 immunostaining showed the existence of endothelial cells on the lumens of this dilated vessels and that these were not dilated sinusoids. [H&E staining (A); Reticulin Silver impregnation staining (B); Azan Mallory staining (C); CD34 immunostaining (D)].
There are two possible reasons for hyper-attenuation on CTAP; one is that portal blood flow to the nodule increases absolutely, and the other is that portal blood flow to the nodule increases relative to the surrounding parenchyma adjacent to the nodule.3 In this case, S-CTAP and the time-density curve clearly indicated that portal venous flow to these nodules showed an absolute increase. It was also supported by the presence of dilated vessels within the nodules.
These indicated that increased portal venous flow was distributed into the hyperplastic nodules by the dilated vessels originated from portal vein. In summary, we reported a case of IPH with multiple hepatic hyperplastic nodules supplied by the portal venous flow. S-CTAP and the time-density curve were very useful to confirm the portal venous flow.
Statement of Conflicts of InterestI have none declared.



