




Abstracts from XVII Mexican Congress of Hepatology
More infoLeft-sided portal hypertension occurs due to obstruction, stenosis, or thrombosis of the splenic vein. The most common causes are pancreatic, including chronic pancreatitis (31.8%-53.8%), pancreatic pseudocyst, and neoplasms.
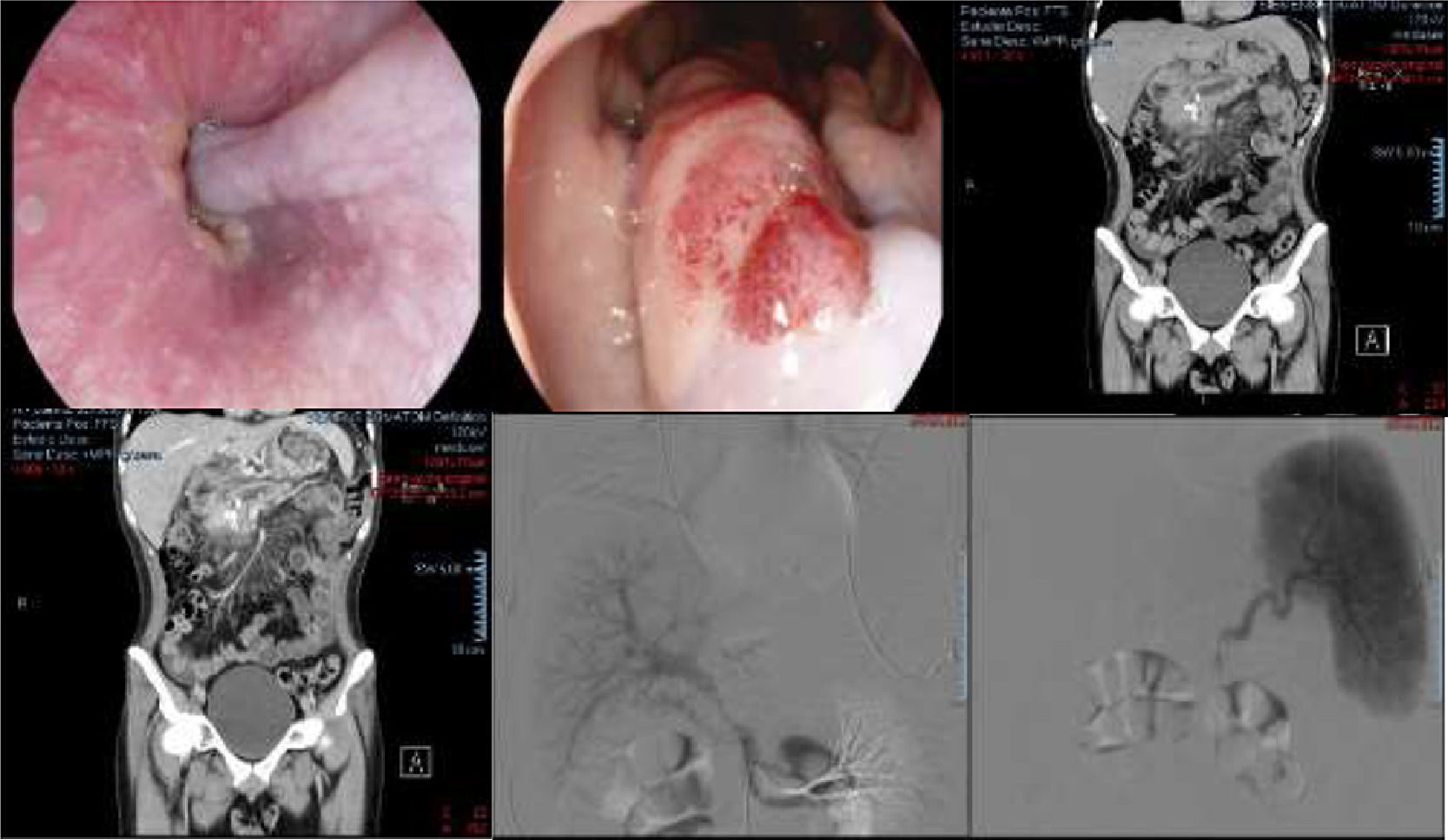
Clinical CaseA 22-year-old man with an 11-year history of transflective pain episodes every three months, without any other symptoms. In the last six months, increased frequency and intensity. He was admitted to the emergency room for mild acute pancreatitis, amylase 181u/l, lipase 230u/l, CRP 35.7mg/L, Procalcitonin 0.04ng/ml, INR 2.4. Abdominal USG is performed with pancreatitis and intra and extrahepatic bile duct dilatation; Contrast-enhanced CT: pancreas with dilation of the main duct of 12 mm and intraductal and intraparenchymal calcifications, portal vein with a diameter of 11.8 mm with stenosis of 80% of its lumen, perigastric, periesophageal and perisplenic collateral veins, stomach with thickening of its folds (14.3 mm) and splenomegaly. He developed hematemesis and melena, panendoscopy showed a large esophageal varix which was ligated, gastric varix GOV 1. Bleeding persists, so arterography and portography were performed, which was ligated, gastric varix GOV 1. Bleeding persists, so arterography and portography were performed, which showed: splenic vein occlusion data and partial portal vein stenosis in its proximal segment. Figure 1.
DiscussionLeft portal hypertension is an etiology related to pancreatic pathologies. It should be suspected if there is a history of pancreatitis coupled with de novo digestive bleeding, splenomegaly without data of cirrhosis or hematological diseases and in a patient with IGV.
ConclusionIt should always be considered regardless of the age of the patients, especially with gastrointestinal bleeding, in order to provide proper treatment.
FundingThe resources used in this study were from the hospital without any additional financing
Declaration of interestThe authors declare no potential conflicts of interest.

Figure 1. Endoscopy A) esophageal varix B) Thickened gastric folds with areas of subepithelial hemorrhage. Contrast-enhanced CT c) Intraductal calcifications and dilation of the main duct. d) Gastric enhancement is observed after contrast administration of perigastric veins. Arteriography and portography E) proximal portal vein stenosis F) splenic vein stenosis.



