



Round ligament cysts are rare lesions, often diagnosed as irreducible inguinal hernias. Most patients are in the third to fourth decade of life, but they can occur in younger patients. They are usually clinically asymptomatic or tend to produce subtle symptoms such as pain, discomfort, or a feeling of heaviness, and swelling. Cysts should not be resized with the Valsalva manoeuvre. Ultrasound is the diagnostic method of choice. The definitive diagnosis is made during surgery, and confirmed by pathological examination.
ObjectiveTo present a case of round ligament cyst, initially diagnosed as an incarcerated inguinal hernia, and a review of the literature.
Clinical caseA 19 year-old female, who was admitted to the emergency department due to her current condition of 5 days of onset. She had an increased volume in right inguinal region that increased with physical exertion, throbbing pain, and nausea without vomiting. A right inguinal mass of approximately of 6cm in diameter was found, which was painful on mid-superficial palpation, reaching a pre-surgical diagnosis of incarcerated right inguinal hernia with an indication of surgical intervention.
ConclusionRound ligament cysts are a rare pathology, often confused with incarcerated inguinal hernias. Although ultrasound is the study of choice, the final diagnosis is usually made during surgery and confirmed by histopathology.
Los quistes de ligamento redondo son lesiones raras, frecuentemente diagnosticados como hernias inguinales irreductibles. La mayoría de los pacientes están entre la tercera y la cuarta décadas de la vida, aunque pueden presentarse en pacientes más jóvenes. Clínicamente son, en general, asintomáticos o tienden a producir síntomas sutiles tales como dolor, molestia o sensación de pesantez y abultamiento. Los quistes no deben cambiar de tamaño con la maniobra de Valsalva. El ultrasonido es la modalidad de elección diagnóstica. El diagnóstico definitivo se realiza durante la cirugía y se confirma con el examen anatomopatológico.
ObjetivoPresentamos el caso de un quiste de ligamento redondo diagnosticado inicialmente como una hernia inguinal encarcelada, así como la revisión de la literatura.
Caso clínicoPaciente femenina de 19 años, quien ingresa al Servicio de Urgencias por padecimiento de 5 días de evolución, con aumento de volumen en región inguinal derecha ante el esfuerzo físico, dolor punzante, náuseas sin llegar al vómito. A la exploración se encontró una masa inguinal derecha de aproximadamente 6cm de diámetro, dolorosa a la palpación medio-superficial, que se integró al diagnóstico prequirúrgico de hernia inguinal derecha encarcelada, por lo que se decidió su intervención quirúrgica.
ConclusiónLos quistes de ligamento redondo son una enfermedad rara, frecuentemente confundidos con hernias inguinales encarceladas. El ultrasonido es el estudio de elección. Generalmente se llega al diagnóstico definitivo durante la cirugía y se confirma por el estudio de anatomía patológica.
Round ligament cysts, also known as Teres ligament cysts of the uterus are rare lesions, about which only 10 cases1 have been reported in the literature in English, between 1980 and 2013.
Round ligament cysts of the uterus are generally misdiagnosed as inguinal hernias, are accidentally detected during examination of the groin during the perioperative period and are often associated with minor inguinal hernias which are clinically insignificant in 30%–50% of cases.1–3 Most patients are in the third to fourth decade of life, but they can occur in younger patients.1 The round ligament of the uterus begins in both uterine horns, which project from the pelvis through the deep inguinal ring, passing through the inguinal canal and continuing up to the labia majora.3,4
During the 7th week of gestation, the foetal inguinal fold is differentiated from the gubernaculum, which descends from the lower end of the gonads, to the protuberances forming the round ligament.1
Embryologically it is the female equivalent of the testes gubernacula in the male,5 which is primarily composed of smooth muscle fibres, connecting tissue, blood vessels and nerves with a mesothelial coating.3
Two theories regarding the pathogenesis have been described and it is believed that they form during the embryology of the round ligament and the histological appearance of the lesions. The first theory is based on the defective obliteration of the Nuck canal.1,3,4 In 1691 the Dutch anatomist Nuck described for the first time a minor outpouching of the vaginal peritoneum which accompanied the round ligament in women through the inguinal ring, which was later called the canal of Nuck. This outpouching regularly disappears during the first 8 months of gestation and, when it persists, may give rise to the appearance of inguinal hernias or Nuck canal cysts (if there is any passing of peritoneal fluid).2 Closure usually occurs during the first year of life. Depending on the extent of the fault, cysts may form at any point throughout the round ligament. According to this theory, a mesothelial cyst is the same medical condition as a Nuck canal cyst.6
The second theory attributes the formation of cysts to the inclusion of embryonic mesenchymal and mesothelial elements or the remains of these, during the development of the round ligament.1,3,4 Several minor mesothelial cystic inclusions inside the round ligament were reported in support of this theory.1
ObjectiveWe present the case of a round ligament cyst, initially diagnosed as an incarcerated inguinal hernia, and a review of the literature.
Clinical caseA female patient aged 19, who presented at the emergency department of our hospital for consultation regarding the diagnosis of an incarcerated right inguinal hernia.
Background details of importance were that she was allergic to trimethoprim-sulfametoxazol and dextromethorphan, she smoked 3–4 cigarettes a week, consumed marihuana 3–4 times a week and was an occasional cocaine consumer. She stated she had never given birth.
She presented due to a 5-day onset of increased volume in the right inguinal region, which increased with physical exertion. She had also suffered for 3 days from a throbbing pain, 7/10 in intensity, which irradiated towards the right iliac fossa, and nausea without vomiting. She had self-medicated with butylhyoscine and sodium metamizole, with no improvements in symptoms, and she therefore presented at the emergency services.
During physical examination a right inguinal mass was found measuring approximately 6cm in diameter, with no changes in surface colouring and of a smooth consistency. It was painful on mid-superficial palpation, was not attached to any deep tissues, and which did not lessen in size through manual manipulation. Peristalsis was normal, there was no abdominal swelling nor signs suggestive of peritoneal irritation.
On admission the para-clinics reported: blood glucose level of 98mg/dl, BUN 10mg/dl, urea mg/dl, creatinine 0.8mg/dl, serum electrolytes Na 137mmol/l, K3.4mmol/l, Ca 9.10mmol/l, hermatological leucocyte biometry 9.8×103, neutrophils 59.4%, haemoglobin 16.40g/dl, red blood cells 49.3%, platelets 25×103, prothrombin time 11.3s, INR 0.9. Simple X-rays of the abdomen revealed with no presence of hydro-aerial levels.
Right incarcerated inguinal hernia was the preoperative diagnosis and the patient was referred for surgery.
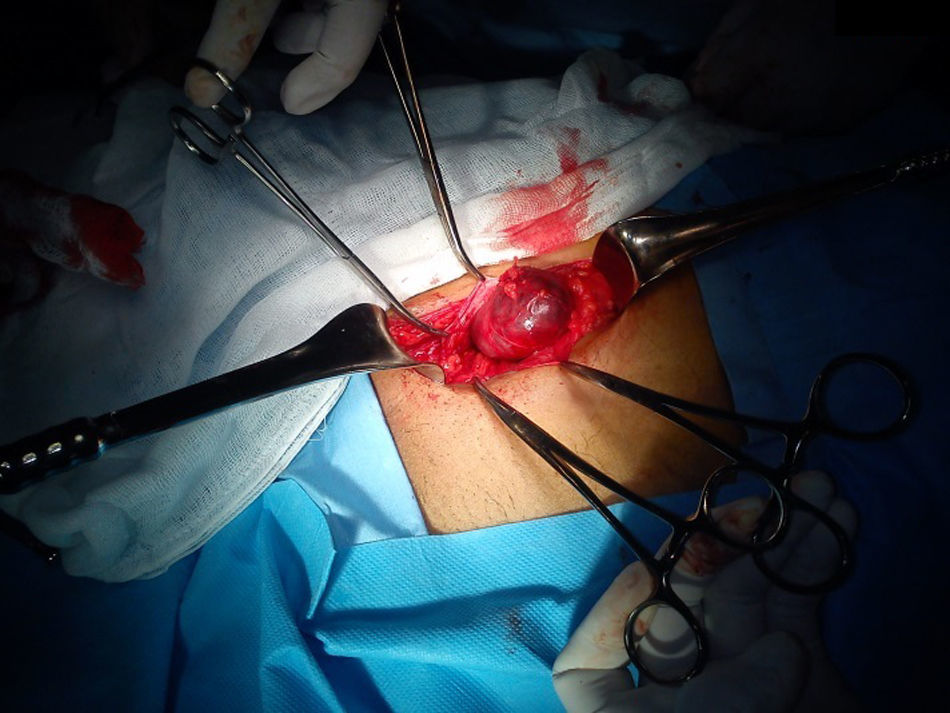
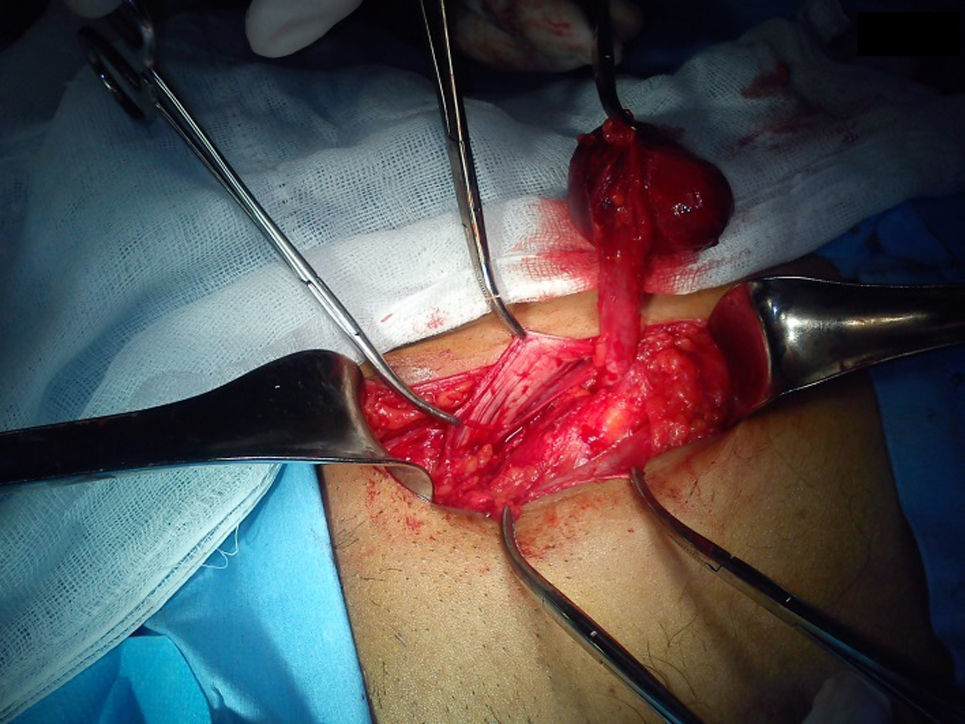
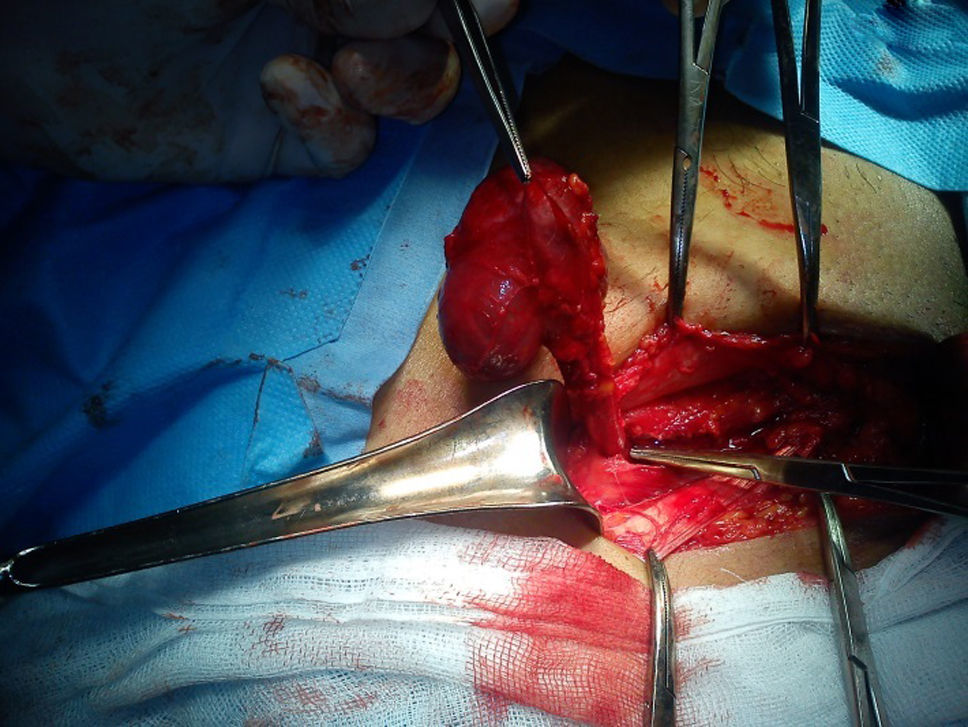
Under general balanced anaesthesia surgical examination of the right inguinal region was carried out (Fig. 1). A violet cystic lesion of approximately 5×6×4cm was found, which started in the round ligament (Fig. 2). The round ligament was removed, together with the cyst up to where it emerged on level with the deep inguinal orifice (Fig. 3). No evidence of protrusion from any indirect hernia sac was found. The cystic lesion was cut away and removed as a block with a segment of the round ligament as well (Fig. 4).


.")

Postoperative evolution was satisfactory and the patient was discharged from hospital two days after the operation.
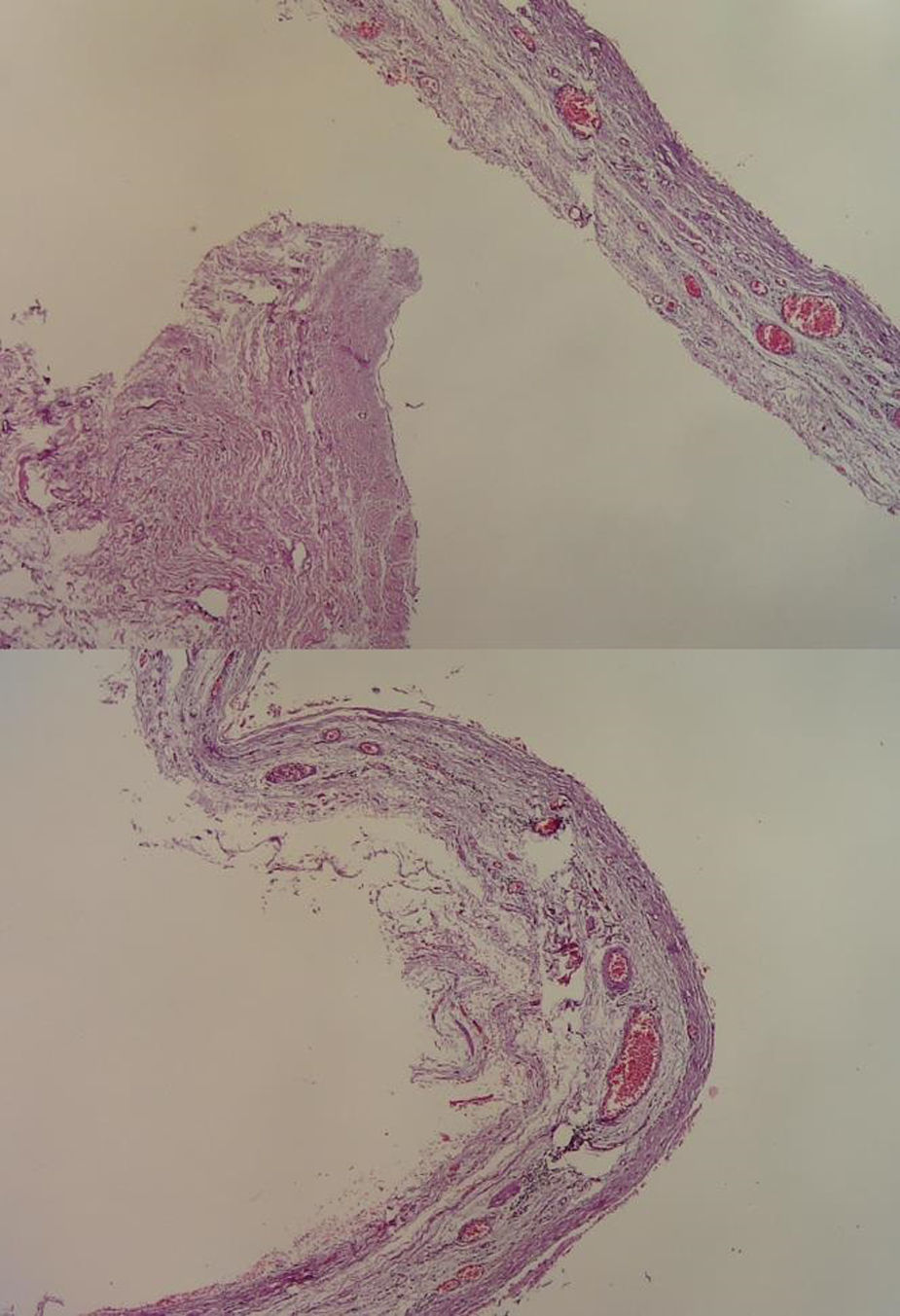
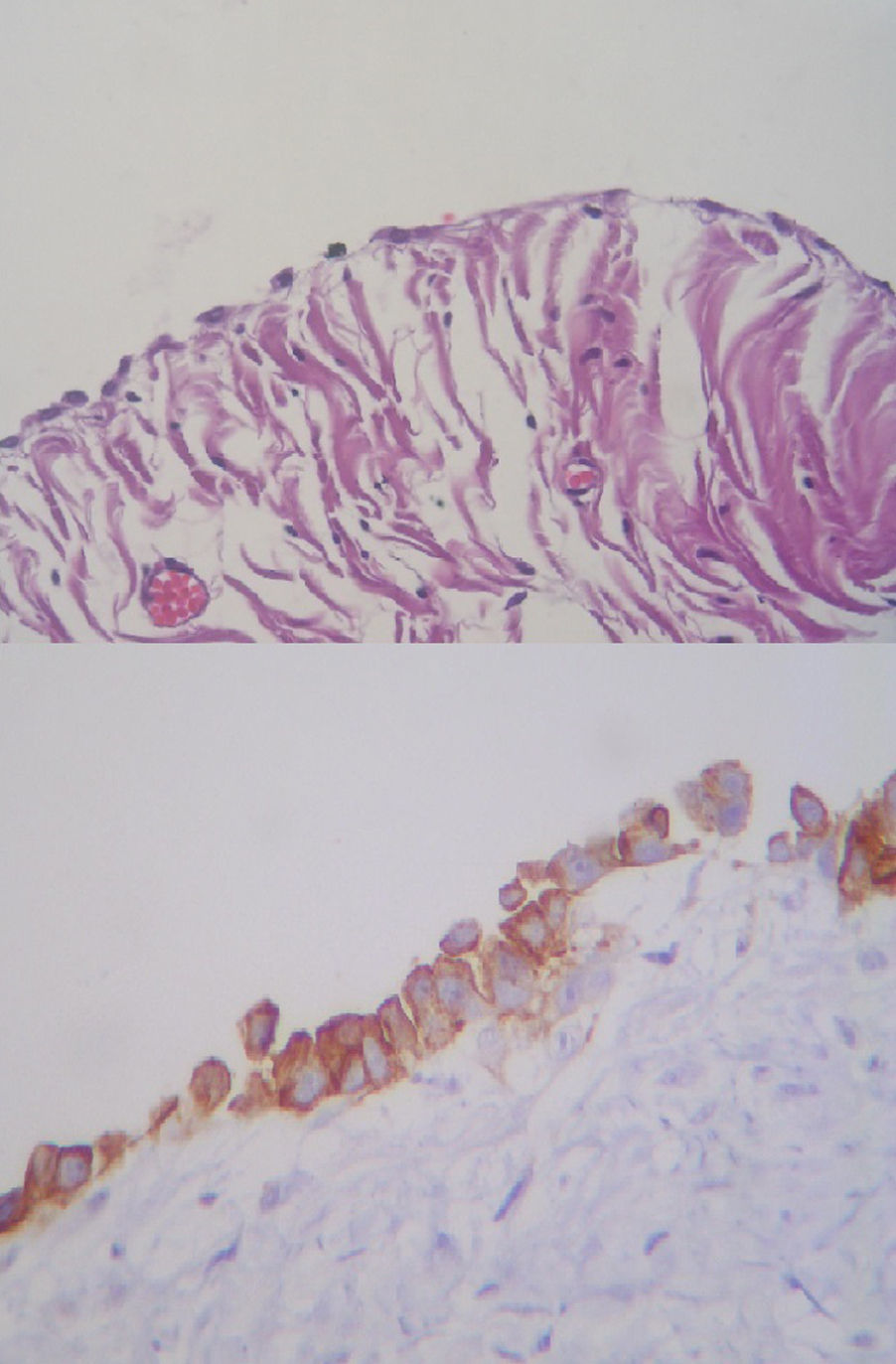
Histopathological findings reported an ovoid specimen measuring 6×5×5cm, with a smooth, solid and rubbery surface which was vascularised and greyish brown in colour. When dissected it was cystic, with a wall of 0.3cm, a smooth internal surface and greyish brown in colour. Microscopic analysis showed a cyst wall with the presence of blood vessels and smooth muscle fibres (Fig. 5), and in the cystic wall coating a cubic and simple flat mesothelial epithelium was noted. Serous cyst was the final diagnosis (Fig. 6).

.")
Round ligament cysts and Nuck canal cysts have the same histological characteristics. However, several of the symptoms during physical examination pathological findings should be considered for differential diagnosis.4
The Nuck canal cyst presents as a painless inflammation. It is most common in infancy and usually presents as a unilocular cyst. Ultrasound imaging presents it as comma shaped, with the tail pointing towards the inguinal canal and the canal where the fluid passes collapses during the Valsalva manoeuvre. In contrast, the round ligament cyst is usually painful, is more frequent in women of middle age or in reproductive age as in the case we present, where the patient was 19. The cyst is usually multiloculated and ultrasounds shows that it is close to the abdominal cavity when the Valsalva manoeuvre is performed.4
82% of round ligament cysts are located on the right side, compared with the Nuck canal cysts, which are mostly found on the left side, with no explanation in this regard reported in the literature.4
Mesothelial cysts are generally asymptomatic or tend to produce subtle symptoms compared with hernias. Pain, malaise or a sensation of heaviness and swelling are the main symptoms. The cysts should not change size with the Valsalva manoeuvre. If the inguinal mass stands out with Valsalva and disappears in the supine position, hernia is the most probable diagnosis. During pregnancy hernias tend to disappear and no constriction is expected because the intestine is pushed by the enlarged uterus.1,2
Increase in size after stimulation with gonadotrophins for in vitro fertilisation in a clinical case was attributed to changes in size of the round ligament and not to the cyst itself, whilst oestrogen and progesterone markers tested negative.1,7
Association has also been made with a history of prior abdominal surgery, pelvic intra-abdominal inflammation or endometriosis.1
Ultrasound is the method of choice because there is no danger of radiation, particularly in children and young women as the population most prevalent to this condition. This is a real time study which offers information on the intestinal peristalsis, vascular supply and changes in size with the Valsalva manoeuvre. Several ecographic aspects have been described, such as the fusiform comma shape or the oval cystic mass, with inner septa if it is multi-nodular and without peristalsis, pedunculated. These lesions are associated with a structure which is similar to a stalk, and this is its connection to the peritoneal cavity.3,8,9
Computed tomography reveals a cystic mass with an irregular enlarged wall and with reinforcement of its solid parts with intravenous contrast enhancement.1,3 The image may provide better anatomical orientation of the mass which arises from the round ligament and may be useful for differential diagnosis of several masses in the inguinal region.3,10
Definitive diagnosis is carried out during surgery and confirmed by histological analysis, where the existence of peritoneal tissue is shown.1,2 Round ligament cysts have a single layer coating of flat and cubic cells which look like mesothelial cells.3 In some cases modifications of the epithelium with the presence of endometriosis, angiomiofibroma and even one case of adenocarcinoma have been described.2
Given the benign nature of this condition, one reasonable option would be to observe the asymptomatic patient through periodic scans. The cysts become asymptomatic or increase in size over time and are better treated through surgical excision. Aspiration of the cyst using ultrasound guidance has also been described and offers temporary pain relief. However, fluid quickly re-accumulates. Posterior prognosis to excision is excellent and no recurrences were reported.1,9
ConclusionsRound ligament cysts rarely present and due to their aetiology and location should fall within the differential diagnoses of inguinal masses in women. They are often confused with incarcerated inguinal hernias due to the impossibility of reducing the palpable mass and the imprecise symptoms. A key aspect to be considered by the surgeon is whether there is an absence of volume increase when the Valsalve manoeuvre is performed. Ultrasound is the tool of choice for completing the pre-surgical protocol, and it is therefore important for the radiologists to be knowledgeable about ultrasound findings of the different conditions which may affect the inguinal region.
Differential diagnosis is clinically difficult and, in general, leads to a final diagnosis during the operation, and is confirmed by the pathological anatomical study.
Due to low incidence, and the before-mentioned facts, suspicions should be raised when a mass in the inguinal region presents.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Vargas-Ávila AL, Gómez-Montoya LE, Guidos-Gil JC, Ávila-Rivera JL, Huerta-García de León Ó, Medina-Tirado MA. Quiste de ligamento redondo que simula hernia inguinal encarcelada. Reporte de un caso. Cir Cir. 2017;85:334–338.