




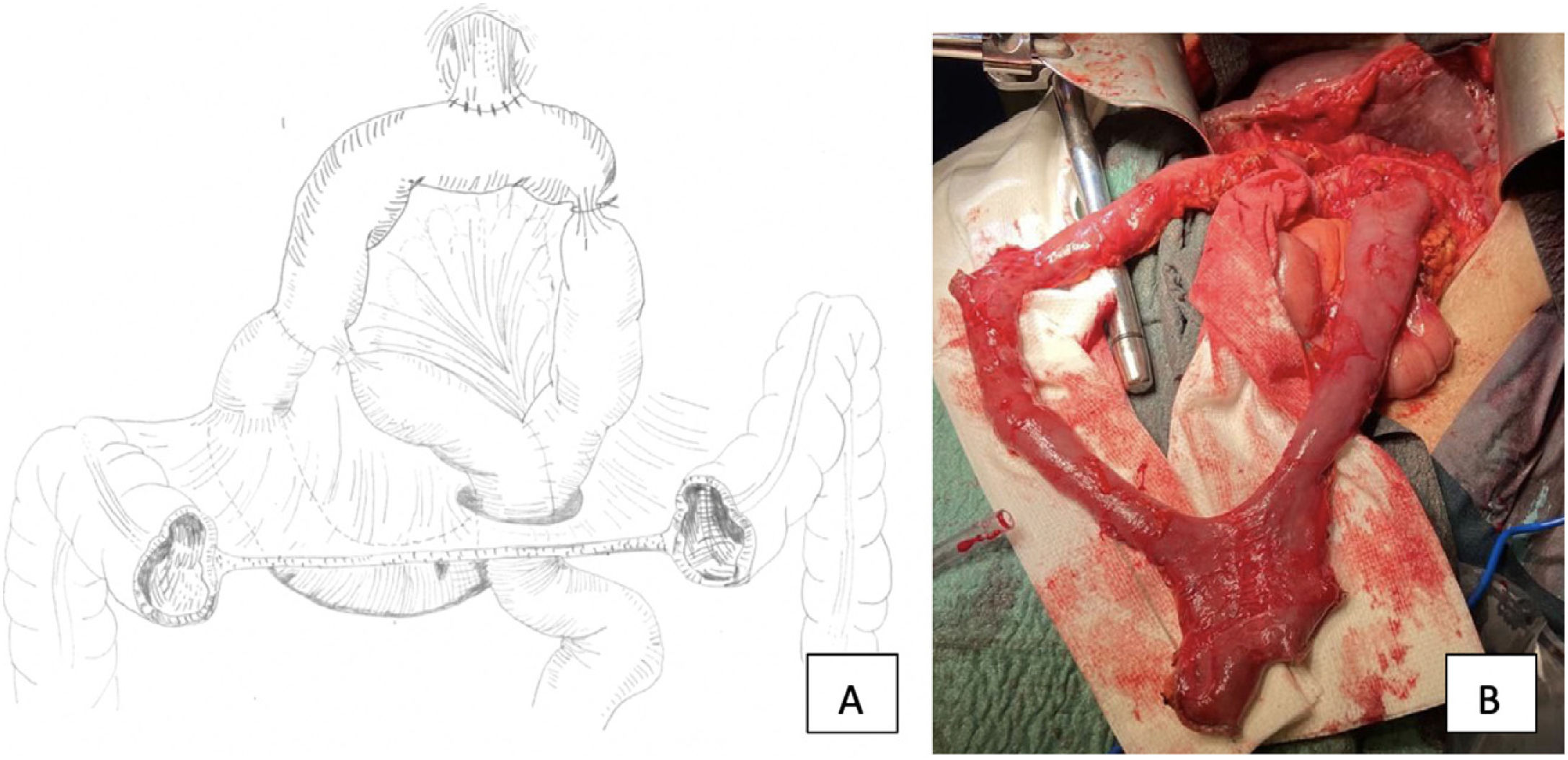
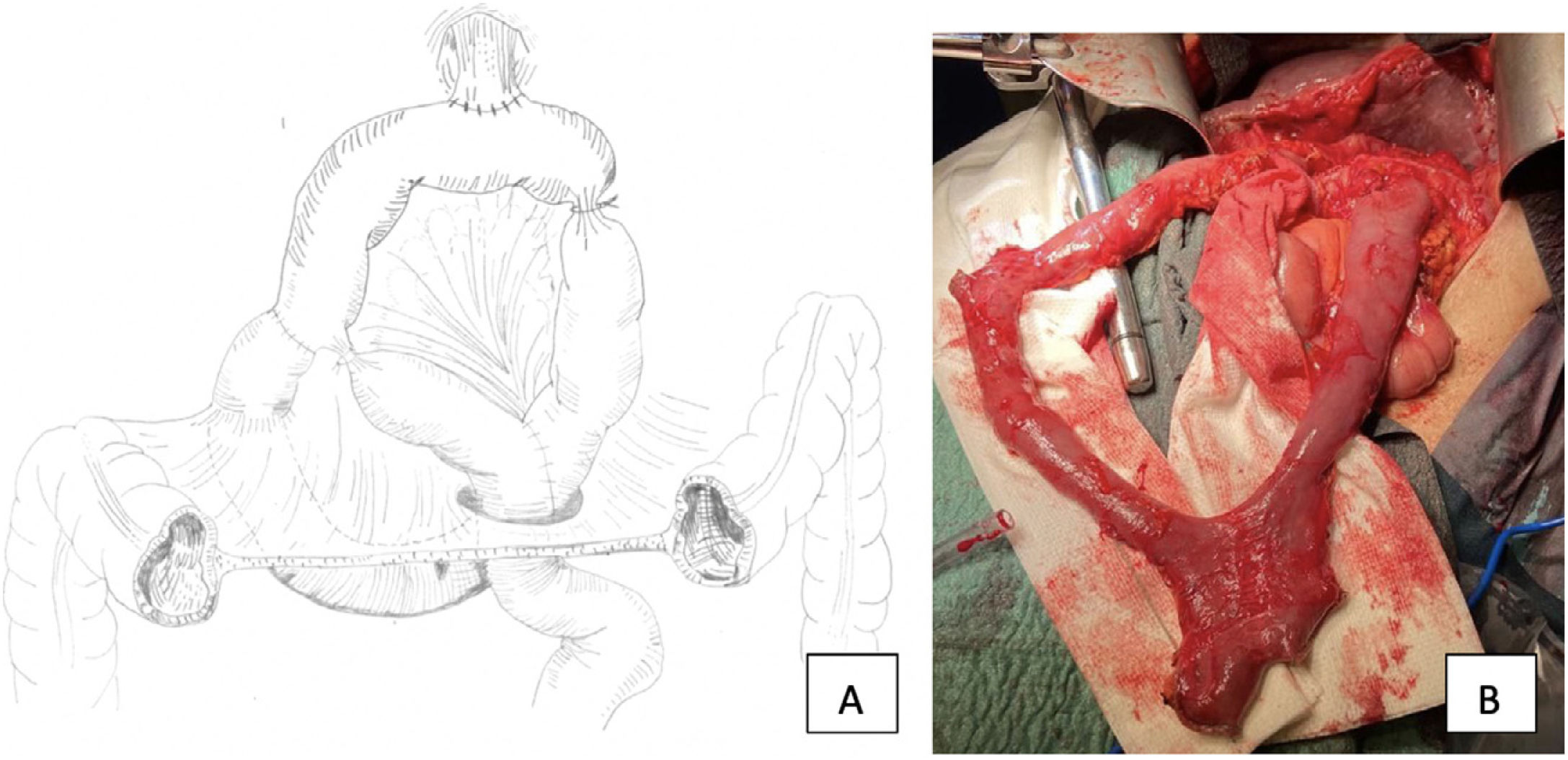
A 72-year-old patient with a history of total gastrectomy (1975) for gastric lymphoma. As a result of dysphagia, a diagnosis of moderately differentiated infiltrating adenocarcinoma of the middle third of the oesophagus (cT3N1M0) was made. He was treated with neoadjuvant chemotherapy (FLOT scheme) and McKeown type oesophagectomy with coloplasty. Intraoperatively, a transit reconstruction was performed using the Massabotu-Tomoda procedure (Fig. 1), which consists of creating a neo-stomach, placing the first jejunal loop in a transmesocolic position and performing an end-to-lateral oesophagojejunal anastomosis, an end-to-lateral duodenojejunal anastomosis and a wide side-to-side anastomosis that forms the foot of the loop. The Tomoda was resected, and a Roux-en-Y reconstruction was performed, avoiding biliary reflux.
Please cite this article as: Lucas Guerrero V, Luna A, Rebasa P, Nve Obiang E, Navarro S. La importancia de conocer técnicas quirúrgicas históricas. Cir Esp. 2022;100:512.
