








The robotic transabdominal preperitoneal approach (rTAPP) is a relatively recent technique for the treatment of inguinal hernia. To achieve optimal results, the 10 golden rules described must be followed. Surgeons in training often review videos to familiarize themselves with new techniques, YouTube being one of the most used platforms. The objective of this study is to carry out an evaluation of the 10 most viewed videos on YouTube of inguinal hernia repair by transabdominal preperitoneal approach (rTAPP) to determine if the 10 golden rules are met.
MethodsIdentify and evaluate the 10 videos with the highest number of views related to rTAPP. Three experienced Surgeons evaluated compliance with the 10 golden rules using a Likert scale. Data were analyzed in Excel (Microsoft) and plotted with Tableau (Tableau Inc). The consistency between evaluators was determined using Cronbach's alpha, considering a value >0.7 acceptable.
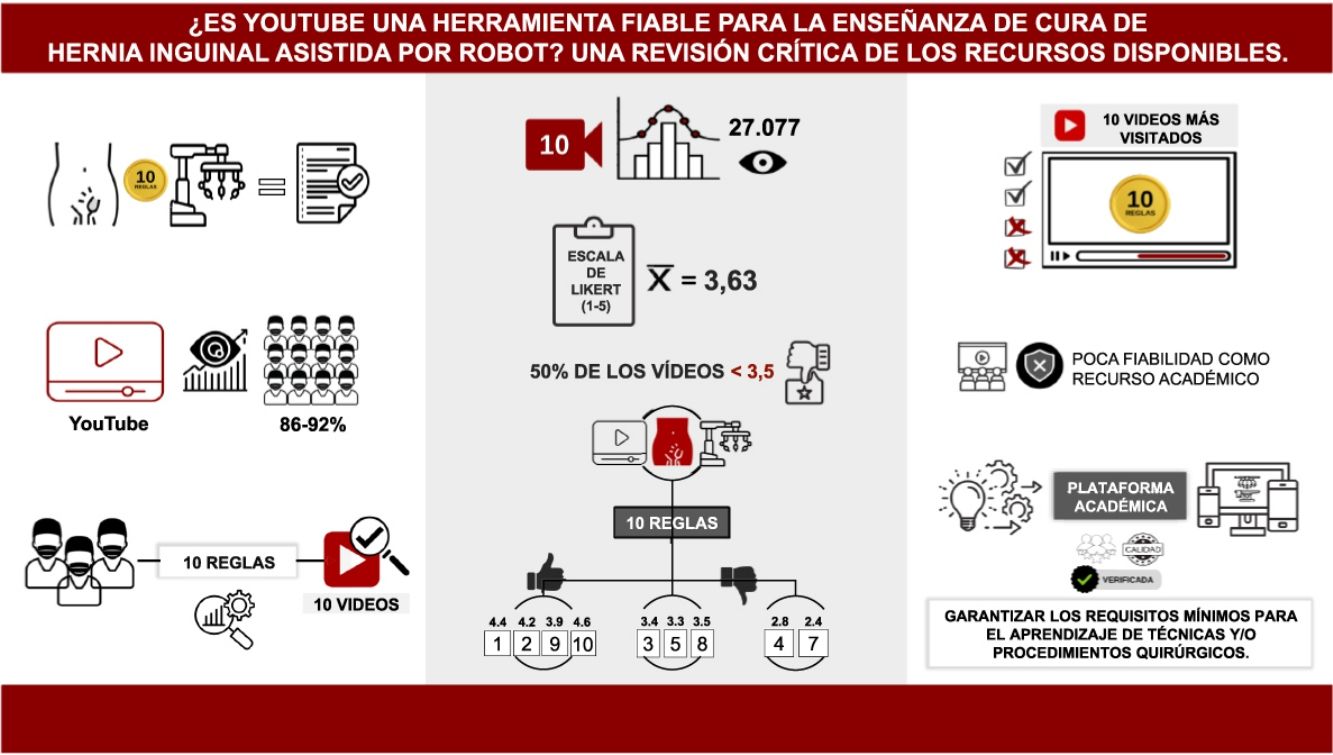
ResultsThe average overall evaluation was 3.63 with a range of 2.6 to 4.9. The scores related to compliance with the rules 1, 2, 9, 10 were satisfactory; on the other hand, rules 3, 4, 5, 7 and 8 were weak, particularly rule number 7. Internal consistency was observed between raters with a Cronbach's alpha of 0.98.
ConclusionsThe lack of compliance with the 10 golden rules in most of the videos demonstrates that the use of videos (YouTube) is not an adequate resource for learning robot-assisted inguinal hernia cure.
El abordaje robótico transabdominal preperitoneal (rTAPP) es una técnica relativamente reciente para el tratamiento de hernia inguinal. Para alcanzar resultados óptimos se deben cumplir las 10 reglas de oro descritas. Los cirujanos en formación suelen revisar videos para familiarizarse con nuevas técnicas siendo YouTube una de las plataformas más utilizada. El objetivo de este estudio es realizar una evaluación de los 10 videos más vistos en YouTube de reparación de hernia inguinal por abordaje transabdominal preperitoneal (rTAPP) para determinar si se cumplen las 10 reglas de oro.
MétodosIdentificar y evaluar los 10 vídeos con mayor número de visualizaciones relacionados con la rTAPP. Tres Cirujanos con experiencia evaluaron el cumplimiento de las 10 reglas de oro utilizando una escala de Likert. Los datos fueron analizados en Excel (Microsoft) y graficados con Tableau (Tableau Inc). La consistencia entre evaluadores se determinó mediante el alfa de Cronbach, considerándose aceptable un valor >0,7.
ResultadosLa evaluación general promedio fue de 3,63 con un rango de 2,6 a 4,9. Las puntuaciones relacionadas con el cumplimiento de las reglas 1, 2, 9, 10 fueron satisfactorias; en cambio, las reglas 3, 4, 5, 7 y 8 fue débil, en particular la regla número 7. Se observó consistencia interna entre los evaluadores con un alfa de Cronbach de 0,98.
ConclusionesLa falta de cumplimiento con las 10 reglas del oro en la mayoría de los videos demuestra que el uso de videos (YouTube) no es un adecuado recurso para el aprendizaje de cura de hernia inguinal asistida por robot.
Inguinal hernia is one of the most common surgical conditions, with an incidence of 27%–43% in men and 3%–6% in women. Every year, more than 20 million inguinal hernias are operated on worldwide.1 Minimally invasive surgical management of the condition was introduced almost three decades ago. Although initial uptake was limited, its popularity has been gradually increasing over the last few years. Two minimally invasive approaches have been described, the totally extraperitoneal approach (TEP) and the transabdominal preperitoneal approach (TAPP).2
The effectiveness of a surgical procedure is closely associated with following the anatomical and technical precepts associated with it. Standardisation of surgical technique is undoubtedly key to obtaining optimal results.3
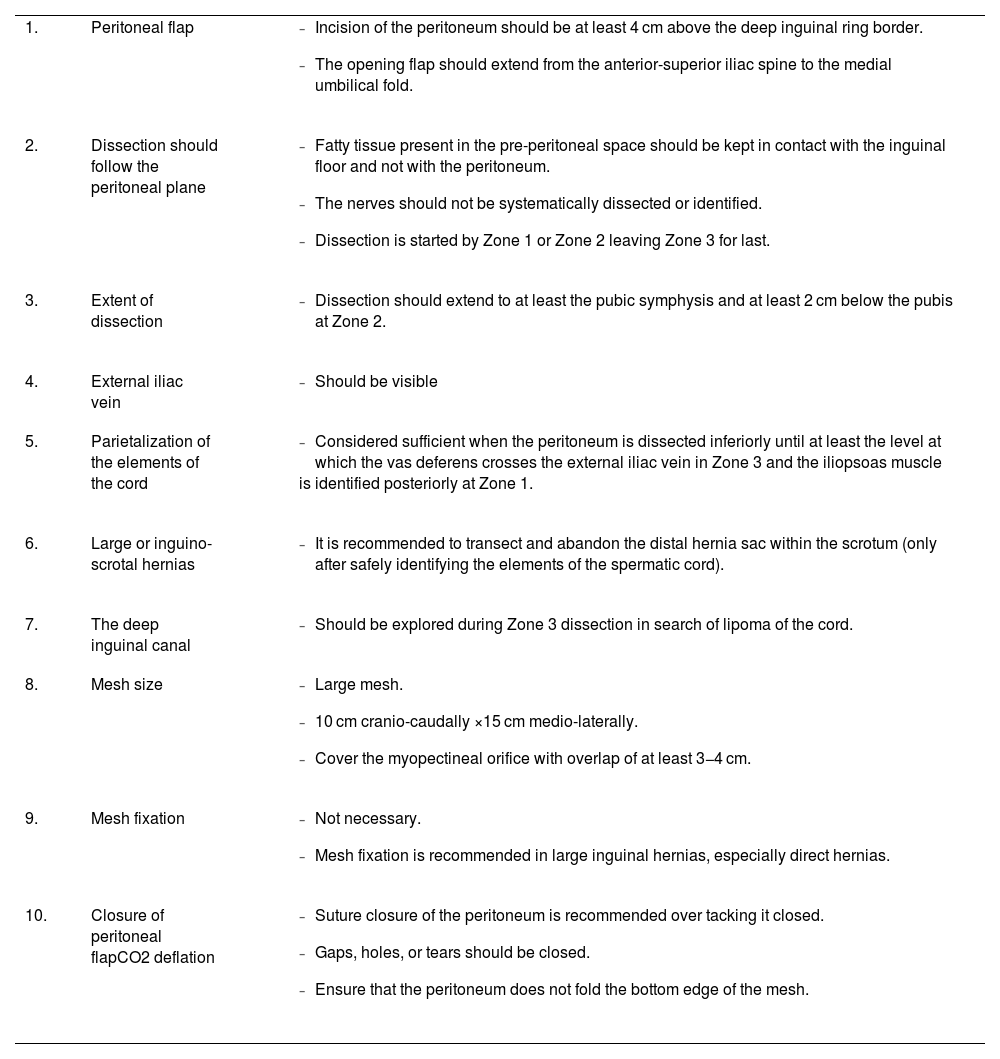
In 2017 Daes et al. introduced the concept of the critical view of the myopectineal orifice (critical view of safety) as a guide to achieving appropriate anatomical exposure in endoscopic inguinal hernia repair, following a set of sequential steps prior to placement of a suitable prosthetic material.4 Based on the critical view of safety, Claus et al. proposed ten golden rules for safe MIS inguinal hernia repair5 (Table 1). Adherence to the 10 golden rules has been considered essential for optimal results, irrespective of the surgical method used.
Ten golden rules for inguinal hernia repair with minimally invasive surgery.
| 1. | Peritoneal flap |
|
| 2. | Dissection should follow the peritoneal plane |
|
| 3. | Extent of dissection |
|
| 4. | External iliac vein |
|
| 5. | Parietalization of the elements of the cord |
|
| 6. | Large or inguino-scrotal hernias |
|
| 7. | The deep inguinal canal |
|
| 8. | Mesh size |
|
| 9. | Mesh fixation |
|
| 10. | Closure of peritoneal flapCO2 deflation |
|
Adapted from C. Claus et al. “Ten Golden rules for a safe MIS inguinal hernia repair using a new anatomical concept as a guide”.5
Trainee surgeons often review surgical videos to familiarise themselves with anatomy, details of surgical technique and new technologies.6 YouTube is the video platform most commonly reviewed by surgeons in training; 86%–92% of surgeons in training have used this platform to familiarise themselves with new surgical techniques.7 YouTube is easily accessible, free of charge, and offers extensive content on medicine and surgery. However, due to the lack of peer review or scientific verification, YouTube videos may be an unreliable source of medical information or educational material on surgical techniques for trainees.8
Although some previous studies have evaluated the YouTube platform for TAPP in inguinal hernia repair,9 this article differs by focusing on specifically evaluating compliance with the ten golden rules using the robotic-assisted approach. This critical evaluation provides valuable insight into the quality of educational videos available on this platform on this surgical technique, thus considering how useful they are as a learning tool.
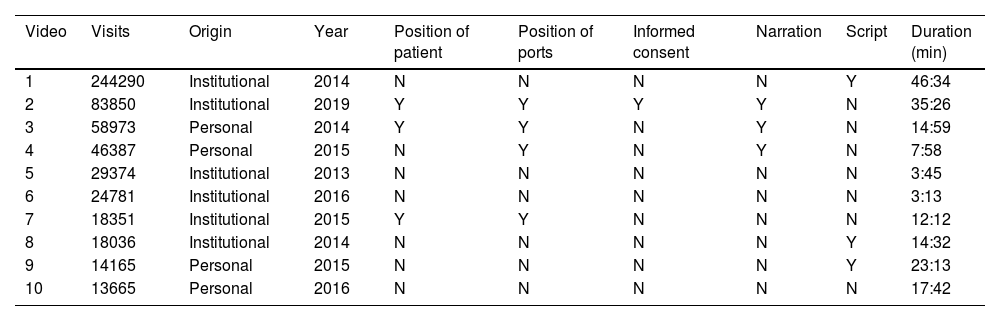
MethodsWe undertook a comprehensive search of the website www.youtube.com to identify the 10 most viewed videos relating to rTAPP. The search was performed using the following terms: "Robot-Assisted Transabdominal Preperitoneal Inguinal Hernia Repair", "robot-assisted hernia repair", "rTAPP inguinal hernia repair", "Hernia inguinal robótica", and "Robotic TAPP hernia". The videos were organised according to the number of views, and from the 10 videos with the highest number of views, the following data were collected for each of the videos: number of views, origin (personal vs. institutional), duration of the video, description of the surgical steps (narration/script) (Table 2).
General characteristics of videos evaluated.
| Video | Visits | Origin | Year | Position of patient | Position of ports | Informed consent | Narration | Script | Duration (min) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 244290 | Institutional | 2014 | N | N | N | N | Y | 46:34 |
| 2 | 83850 | Institutional | 2019 | Y | Y | Y | Y | N | 35:26 |
| 3 | 58973 | Personal | 2014 | Y | Y | N | Y | N | 14:59 |
| 4 | 46387 | Personal | 2015 | N | Y | N | Y | N | 7:58 |
| 5 | 29374 | Institutional | 2013 | N | N | N | N | N | 3:45 |
| 6 | 24781 | Institutional | 2016 | N | N | N | N | N | 3:13 |
| 7 | 18351 | Institutional | 2015 | Y | Y | N | N | N | 12:12 |
| 8 | 18036 | Institutional | 2014 | N | N | N | N | Y | 14:32 |
| 9 | 14165 | Personal | 2015 | N | N | N | N | Y | 23:13 |
| 10 | 13665 | Personal | 2016 | N | N | N | N | N | 17:42 |
Compliance with the 10 golden rules was assessed to evaluate the videos (Table 1). To do so, we created a google form where each parameter was evaluated using a Likert scale. Rule 6 (distal sac section) was not assessed as it only applies to a certain type of inguinal hernia (large or inguinoscrotal hernias). This form together with the links to each of the videos was sent to three surgeons with experience in minimally invasive techniques for the treatment of inguinal hernia by transabdominal preperitoneal approach in three different centres around the world (Venezuela, Chile, Spain). Surgeons with more than 100 cases of inguinal hernia repair by laparoscopic or robotic approach were considered expert surgeons.
Statistical analysisData were analysed in Excel (Microsoft®) and plotted with Tableau (Tableau Inc®). Inter-rater consistency was determined by Cronbach's alpha, with a value >.7 considered acceptable.
ResultsFrom the main characteristics of the videos evaluated, the average number of views of the 10 videos selected for the study was 27,077 (13,665−244,290). Most of the videos (60%) are of institutional origin. Forty percent of the videos contain a narrative or script describing the surgical steps or technical aspects of the surgery, and 60% did not describe relevant data on patient positioning or portal placement.
We assessed compliance with the 10 golden rules in minimally invasive treatment of inguinal hernia using the transabdominal preperitoneal approach (Fig. 1). Internal consistency between raters was observed with a Cronbach's alpha of .98.

The mean overall evaluation of the videos was 3.63 (Fig. 2), with a range of 2.6 to 4.9. It should be noted that 50% of the videos were evaluated below 3.5; this was considered unsatisfactory. No relationship was found between the overall evaluation of the video and the number of views, the length of the video, the presence of narration/script, or the origin of the video.

As for the analysis of compliance with the golden rules (Fig. 3), the scores relating to the initial (rule 1 and rule 2) and final (rule 9 and rule 10) steps of the procedure were quite satisfactory. In contrast, compliance with rules 3, 4, 5, 7, and 8 was rather weak, in particular the mean evaluation of rule number 7, which was 2.4.
Discussion
YouTube is an accessible, easy-to-use, and free platform offering a wide range of information at our fingertips, making it one of the most visited video platforms in the world. In recent years, its use in the scientific community has been increasing, because it offers a wide variety of videos related to medicine and surgical interventions. Several studies have demonstrated the use of this platform by residents of different surgical specialties.7,10–12
Despite the accessibility and popularity in the medical community, videos relating to surgical procedures available on YouTube are not peer-reviewed, and therefore often lack the academic rigour necessary to be a reliable source of medical education.9 Furthermore, anyone can share videos on this platform without restrictions. This sometimes affects the quality of the videos, which is compromised in terms of photography, editing, and recording.
Robotic-assisted transabdominal preperitoneal repair (rTAPP) has emerged as a strong option for the surgical management of inguinal hernia. Robotic surgery offers multiple benefits such as improved visualisation and dexterity, while being ergonomic for the surgeon, especially in difficult locations.13 However, the use of the robot is conditional on surgeons trained on the platform or system, who must reach a high level of the learning curve to master this technique.13 Many surgeons, unfamiliar with the use of the robot or this technique, rely on YouTube videos as an academic learning aid. In this study, we evaluated the academic quality of the 10 most viewed YouTube videos relating to rTAPP surgery available until 1 December 2021.
After a rigorous review by a panel of experts, we found that 50% of the videos had a rating below 3.5 (out of 5); only one video had a rating above 4.5, demonstrating compliance with the steps and categorising it as a good resource for students to use. Regarding the characteristics of the evaluated videos, most do not provide solid information about portal placement, docking of the robot, or even a description - in written or narrated form - of what the surgeon is doing in the different stages of the surgery. It follows from these considerations that the evaluated videos might be categorised as a poor academic resource.
Table 1 describes in detail the golden rules for inguinal hernia repair, it was striking that rules 1 and 2 (initial part of the surgery) and rules 9 and 10 (final part of the surgery) had a mean score above 3.9, while rules 3, 4, 5, 7, and 8 had a score below 3.5. It is worth noting that rule 7 had a mean score of 2.4.
Rule 7 involves exploration of the deep inguinal canal for lipoma of the cord. If a lipoma is found at this level, it must be dissected because, if left untreated, it can be a cause of recurrence of hernia.5 Therefore, this rule is essential during surgery, and this rule is all the more important because only after having completed this step, should the surgeon proceed to mesh placement.5
Obviously, a low mean overall score should warn us about the unreliability of the most viewed videos (related to rTAPP) that can be found on YouTube, as an academic source. We believe that videos and audiovisual materials are a valuable academic resource for surgeons in training, but an alternative site with a higher academic standard would be desirable. Videos published on the platform should be regulated, so that peer review is mandatory and minimum requirements are established in terms of audiovisual quality and academic information provided during the video.
Video education is a valuable tool in the training of surgeons and other medical professionals, however, the need for structured training including familiarisation with the system, simulation, and supervised procedures should not be overlooked. In relation to the videos, the quality and reliability of the content presented must be ensured, implementation of a pre-review of content, similar to the review process for academic articles, would ensure that the information presented is accurate and reliable and thus help to improve medical education.
Until this is achieved, trainees should focus on the official educational platforms. The addition of the Intuitive HUB (Intuitive Surgical®) system to robotic surgery will provide an excellent alternative for storing and accessing videos. This system is integrated into the da Vinci Robot; it allows video or images to be recorded directly from the console. It will automatically place markers of relevant moments of the surgery (stapling, activation of Firefly, use of autosutures etc.), facilitating the editing of videos to be shared on an academic platform, also offered by this system, where they can be stored for either on-demand consultation or for streaming.
The implementation and adoption of an educational platform with these characteristics would be revolutionary in promoting the massive use of surgical videos among surgeons in training; use of this platform will reassure students that the information published is verified and reliable for surgical education. This will contribute to the knowledge needed by the trainee when performing new surgical techniques and/or procedures.
One of the limitations of this study was that the videos were evaluated by only three reviewers who are experts in the field. Although the reviewers were carefully selected and have extensive experience, the opinion of a limited number of reviewers may influence the variability of the ratings given to the videos.
Analysis of the most viewed videos on YouTube demonstrated a lack of compliance with the golden rules in the critical steps of minimally invasive, robotic-assisted inguinal hernia repair and should not be considered a suitable learning resource. An academic platform with established peer review is needed to ensure the minimum requirements for learning new techniques and/or procedures.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sector.
Conflict of interestsThe authors have no conflict of interests to declare.
DeclarationsThe authors declare that they have received no funding, donations, or other support in drafting this manuscript. Dr. Alexis Sanchez and Dr. Omaira Rodriguez have been proctors of robotic surgery. The other authors have no relevant financial or non-financial interests to declare. All authors contributed to the conception and design of the study. Data preparation and analysis were performed by Alexis Sanchez, Omaira Rodriguez, Cristina Inchausti. The first draft of the manuscript was written by Alexis Sánchez, Francisco Couto, and Iván Mogollón. All authors commented on the previous version of the manuscript. All authors read and approved the final manuscript. This work did not involve research on human subjects; therefore, it is exempt from bioethics committee approval.
