




Neuroblastoma originates in the undifferentiated cells of the neural crest and forms the most frequent extracranial solid tumours in children.1 In adults, however, these tumours are uncommon, and less than 10% are diagnosed in patients over the age of 10.2 In patients between the ages of 30 and 39, the incidence is 0.2 cases per million.2,3 As there are no treatment protocols for adults, therapies are based on paediatric guidelines.4 We present an adult case of retroperitoneal neuroblastoma, along with an analysis of its diagnosis and treatment.
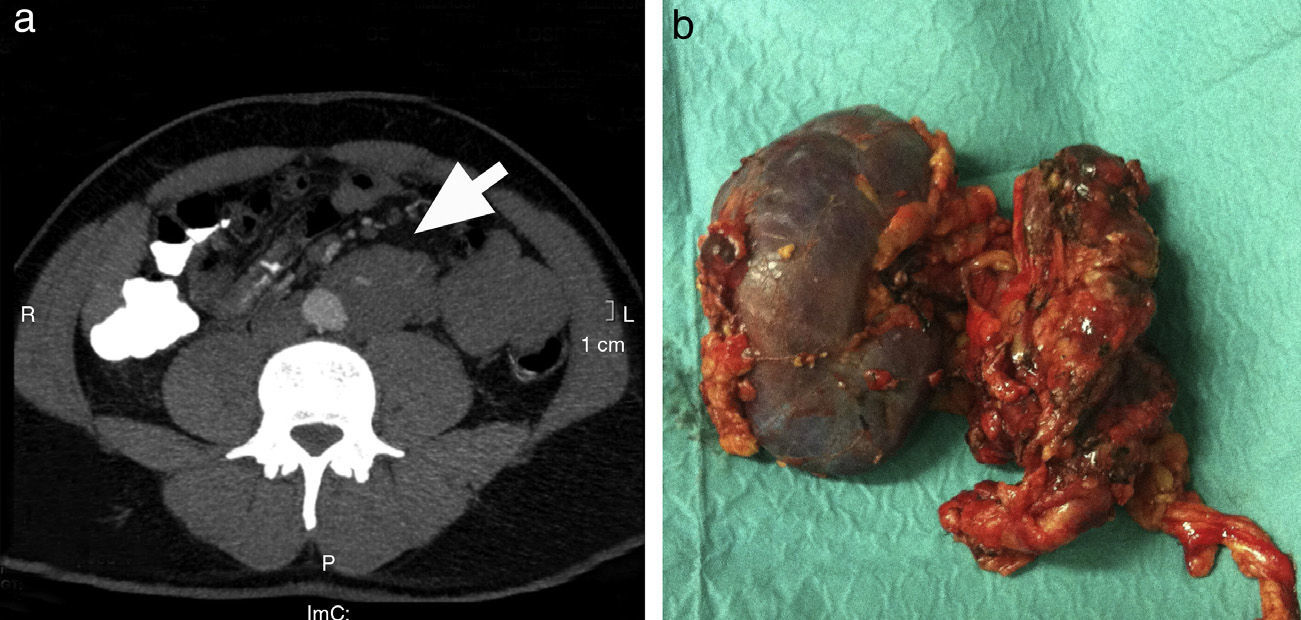
A 39-year-old male presented with persistent left lumbar pain, with no exacerbations, that had been progressing for several weeks. Physical examination was normal. Computed tomography (CT) detected a retroperitoneal mass (Fig. 1a). Cytology of the fine needle aspiration (FNA) biopsy was compatible with neuroblastoma. Fluorodeoxyglucose positron emission tomography (FDG-PET) showed no distant metastasis. Urine catecholamines were normal. A midline laparotomy was performed, and we found a large mass measuring 4cm×4cm×11cm. The lesion was resected in association with left nephrectomy, because of tumour infiltration of the ureter (Fig. 1b), and retroperitoneal lymphadenectomy. The histology study defined the mass as poorly differentiated neuroblastoma with lymph node involvement. The patient was administered chemotherapy (3 cycles of carboplatin and ectoposide, alternating with 3 cycles of cyclophosphamide, adriamycin and vincristine) and external radiotherapy. Twenty-four months after the procedure, the patient is asymptomatic and no recurrence was detected on the follow-up PET-CT or metaiodobenzylguanidine (MIBG) scan.
 Preoperative abdominal computed tomography demonstrating a retroperitoneal mass in the left infrarenal space (arrow), which is in close contact with the circumference of the aorta; (b) Surgical specimen of the en bloc exeresis of the mass (4cm×4cm×11cm) next to the left kidney.")
Neuroblastoma tumours are rare in adults, and they appear more aggressively and at more advanced stages than in children.1,6 Their location in the extraadrenal medullary tissue, as in our patient, is more frequent in adults. Neuroblastoma usually has an insidious clinical course and presents with fast-growing abdominal masses that cause abdominal pain as they usually reach large sizes,7 as in our case, as well as pain secondary to bone metastasis.1,7 Synchronous metastases appear in 70% of cases.5
Regarding diagnostic imaging techniques, the study with the greatest utility is CT scan, which identifies a mass that is predominantly retroperitoneal and more heterogenous with contrast enhancement.8 Magnetic resonance (spinal tumors1,2) and MIBG are also useful. FDG-PET is also very suitable for the diagnosis of metastases and recurrence.2
The indication of FNA is arguable because, as these tumours are sympathetic in origin, they can cause a hypertensive crisis due to the release of catecholamines into the blood stream. In this case, catecholamines were negative. It should be noted that only 40%–57% of cases in adults present elevated urine catecholamines, compared with elevation in 95% of cases in children, and therefore normal catecholamine levels do not exclude diagnosis.4,5 In this case, MIBG scintigraphy was not done as there was already a cytology diagnosis. This test can also aid diagnosis, although it may occasionally give false negatives.2 FDG-PET showed no metastasis.
There is no consensus about the treatment of neuroblastoma in adults. In general, paediatric therapeutic guidelines are used,4 which follow the classification of risk groups by the International Neuroblastoma Staging System (INSS), histology and genetic characteristics.9
The INSS classifies neuroblastoma into 4 stages, depending on the location of the tumour, surgical margins and invasion of other structures. The few cases that have been reported usually present at advanced stages (stages III and IV), and recurrences are frequent.1–6 Treatment is based on the combination of chemotherapy, surgery (including lymph node dissection, which is also useful for staging) and radiotherapy. Nonetheless, surgical treatment is only performed in a few cases due to the advanced stage of the disease.3–5
In stages I and II,the treatment of choice is surgery with adjuvant chemotherapy and radiotherapy in some cases of stage II. Adjuvant therapy has not been established in stage I paediatric patients.7,9 Due to the poor prognosis, in adults this treatment could be considered in the initial stages.7,9 In the last decade, new genome sequencing techniques for neuroblastoma have led to the identification of genes related with the progression of the disease as well as new target drugs, which may change adjuvant therapy in adults in the future.4,10
In our patient, R0 resection was performed with affected ipsilateral lymph nodes (stage II-B). Chemotherapy and radiotherapy were administered after surgery and postoperative evolution has been positive, including biannual follow-ups with PET-CT and MIBG studies.
In conclusion, neuroblastoma tumours are uncommon in adults. They are usually diagnosed at advanced stages and require surgery and intensive oncologic treatment. In the few cases that have been reported, there is a high rate of recurrences, so close patient monitoring is recommended. Because of the limited data published in the literature, multi-centre studies are necessary to merge and compare experiences.
Please cite this article as: Febrero B, Ríos A, Rodríguez JM, Flores B, Parrilla P. Neuroblastoma retroperitoneal en el adulto. Una entidad infrecuente. Cir Esp. 2015;93:e147–e148.
