




Medullary thyroid carcinoma (MTC) is a rare tumor that is sporadic in most series (more than 75% of cases). However, in areas where there is a concentration of patients with multiple endocrine neoplasia (MEN) syndrome, familial tumors may be more common.1–3 Surgery is the only potentially curative treatment option for these tumors, but the recurrence rate is high (30%-65% in most series), even despite adequate radical surgical technique.1,4 For the management of recurrent MTC, surgery is the most effective treatment and the only potentially curative one. However, there is no consensus on when it should be done, or which surgical technique is best.5 As a general rule, surgery seems to be more effective for local recurrence, while the treatment of choice for disseminated disease is palliative medicine.5 The objective of this study is to evaluate the results of surgical treatment in recurrent cervical MTC.
Our study population included patients with MTC who were treated surgically, met the criteria for cure, but who later presented tumor recurrence during follow-up. The patient was considered to meet cure criteria when, 6 months after treatment, there were no symptoms or signs of disease, serum calcitonin (Ct) levels were below 10 pg/mL in 2 consecutive determinations between the 3rd and 6th months after surgery, and absence of elevated Ct levels after stimulation with pentagastrin or calcium. Recurrence was determined by patients who, after 6 months of treatment, and after meeting criteria for cure, presented Ct levels above 10 pg/mL and/or elevated Ct levels after stimulation with pentagastrin or calcium. Patients with incomplete follow-up or less than 2 years after the initial surgery were excluded from the study.
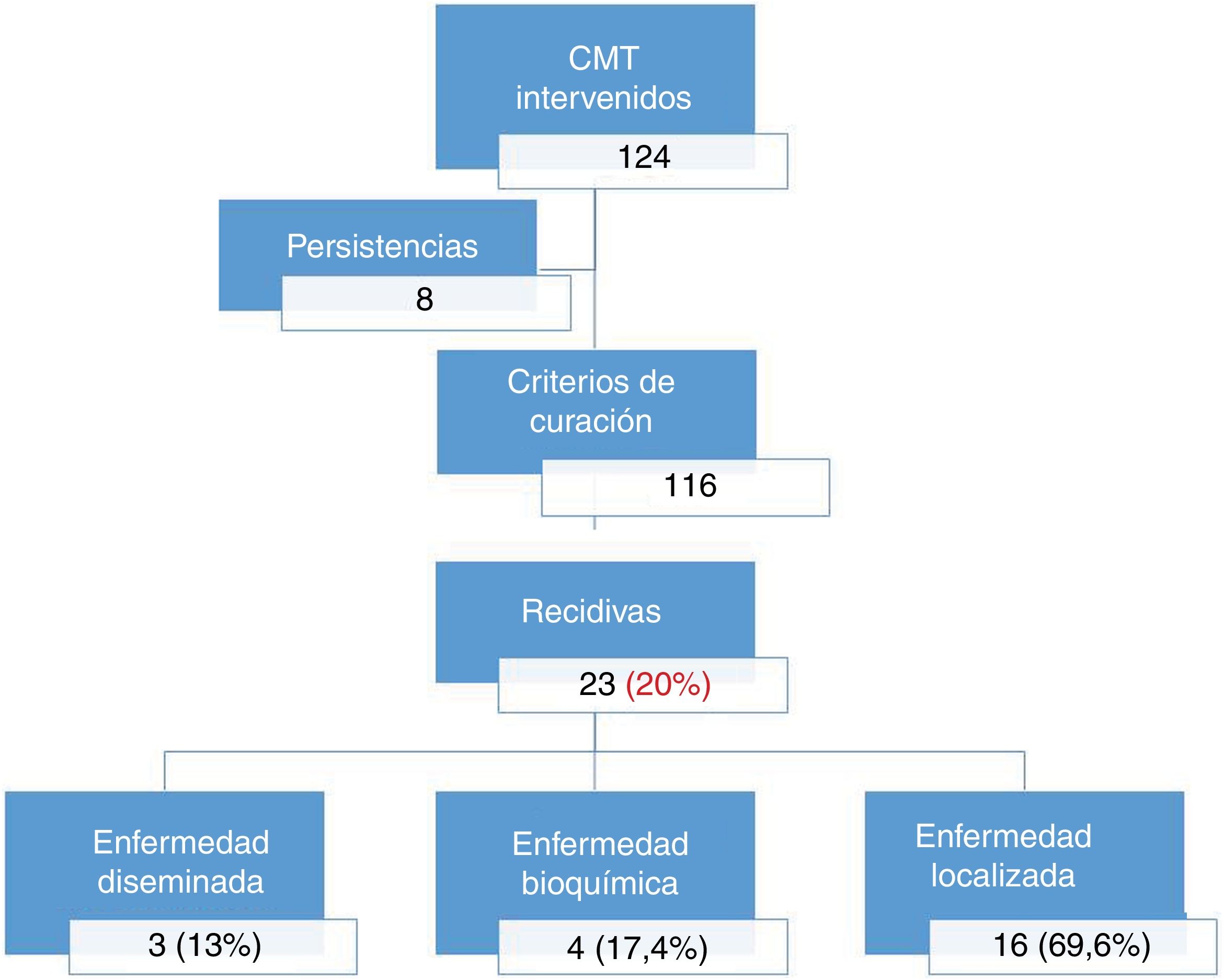
Out of the 124 patients who underwent MTC surgery with curative intent, 8 with persistent disease were excluded (Fig. 1). After a mean follow-up of 89 ± 49 months, out of the 116 patients who fulfilled the criteria for cure, 23 presented tumor recurrence, with a recurrence rate of 20%. The most frequent type of MTC was familial associated with MEN 2A syndrome (70% cases). The types of recurrence were: disseminated metastatic disease in 13% (n = 3); localized disease in 69.6% (n = 16); and non-localized biochemical disease in 17.4% (n = 4).

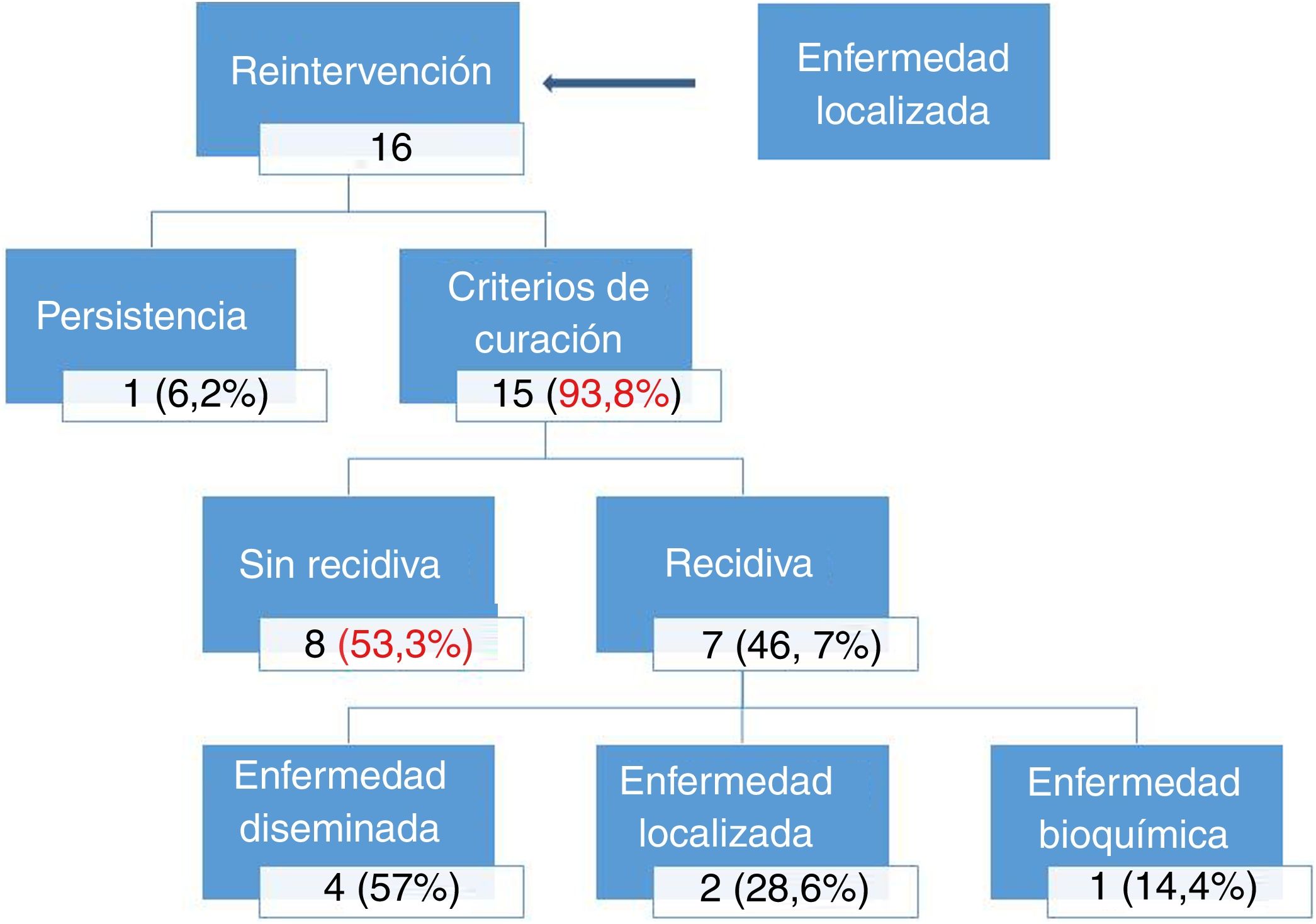
The 16 patients (69.6%) with cervical recurrence (relapse time 60 ± 32 months) underwent surgical treatment, and the initial surgery was completed in all patients with total thyroidectomy, bilateral central lymph node dissection, and bilateral jugular cervical lymph node dissection. After surgery, 15 of the 16 patients (93.6%) met criteria for cure 6 months after surgery, and the remaining case presented persistence of the disease. With a mean follow-up of 196 ± 116 months after surgery, 53.3% (n = 8) continue to meet the criteria for cure, while the remaining 46.7% (n = 7) have had a second recurrence (Fig. 2). The most frequent clinical form of the second recurrence was the disseminated form. In 2 of the recurrences, the disease was located at the cervical level, requiring successive reoperations over the years without achieving cure criteria. One of the recurrences was biochemical.

Medullary thyroid carcinoma is sporadic in approximately 75% of cases, although in endemic areas of MEN syndrome, such as ours, this percentage is inverted.1,3 This factor means that our recurrence rate is lower than reported in most series. This is due to the early diagnosis of familial cases by genetic screening after the initial familial case has been diagnosed. Therefore, younger patients are treated at earlier stages of the disease, resulting in a better prognosis and lower recurrence rates. In the same stage of the disease, however, the prognosis is the same for the sporadic and familial varieties.1–5
Recurrences are a poor prognostic factor, since they lead to greater morbidity secondary to the disease, surgery, and the frequent subsequent effects of the medical treatment applied to these tumors.6 Cervical recurrences require early diagnosis and adequate surgical treatment to achieve good oncological results. Thus, in our series, 93.8% of the cases with cervical recurrence achieved criteria for cure after surgery, and more than half persist with cure criteria throughout follow-up (Fig. 2).2,6,7
In recent years, we have seen that it is essential for these patients to be managed by multidisciplinary teams at specialized hospitals to improve results. In this manner, patients with localized recurrences can be rescued for surgical treatment. Meanwhile, in patients who are not candidates for surgery, survival is significantly prolonged with new medical therapies.2,8,9
In conclusion, surgical treatment of local cervical recurrence of MTC achieves criteria for a cure in a high percentage of cases, and in more than half of these cases the criteria for cure persist for more than 10 years. Therefore, MTC should be initially treated in multidisciplinary referral units for adequate surgical treatment of initial presentations and recurrences, and multidisciplinary treatment should be personalized to achieve longer survival.
Please cite this article as: Ríos A, Mateu G, Torres M, Febrero B, Rodríguez JM. Tratamiento quirúrgico del carcinoma medular de tiroides recidivado en un centro con alta incidencia de carcinoma medular asociado al síndrome de MEN. Cir Esp. 2021;99:245–247.
