





Small bowel prolapse through a spontaneous perforation of the rectum is an extremely rare condition. Since Benjamin Brodie1 documented the first case in 1827, around 70 cases have been reported in the scientific literature. Rectal perforations with evisceration of intestinal content can have multiple etiologies, which are traditionally classified into 2 groups, trauma-related and spontaneous, whose etiologic mechanism is uncertain.2
We present the case of a patient who developed transanal intestinal evisceration secondary to spontaneous rectal perforation.
The patient is a 34-year-old male who came to the emergency room due to abdominal pain and prolapse of small bowel loops though the anus, which had occurred during the effort of defecation. The patient reported no pathologic history of interest and denied having had a history of rectal trauma, rectal instrumentation, anal sexual activity or constipation. Physical examination detected the protrusion of small bowel loops through the anus with signs of congestion. Following aseptic measures and after having performed lavage with warm saline, the loops were reintroduced into the abdominal cavity to avoid ischemia. The abdomen was soft, with pain upon deep palpation in the hypogastrium and no rebound tenderness. Upon rectal examination, an interruption in the anterior wall of the rectum was palpated. Urgent abdominal CT scan with endorectal contrast agent demonstrated a rectal perforation located approximately 9–10cm from the anal margin.
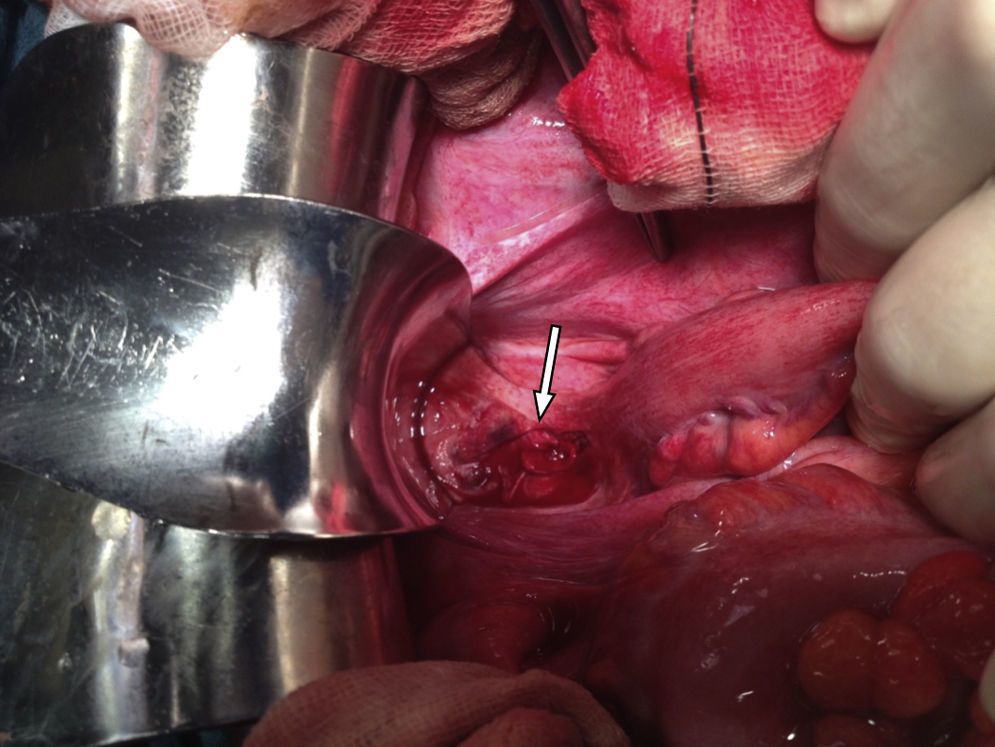
Emergency laparotomy was indicated, which demonstrated a laceration on the anterior side of the rectum, above the perineal flexure, and purulent liquid in the pelvis. The laceration was approximately 4cm long, extending from 1cm below the flexure to approximately 3cm above, with no signs of ischemia. The ileal loops were congestive and edematous, with signs of viability. The sigmoid colon and upper rectum were mobilized, and we proceeded with anterior resection of the rectum, creating an end colostomy in the left iliac fossa. The procedure was completed with lavages of the abdominal cavity.
The patient's condition progressed correctly, and he was discharged on the 6th day post-op. The patient is currently awaiting surgical reconstruction of the intestinal tract (Figs. 1 and 2).


Spontaneous perforation of the rectum with transanal prolapse of intestinal content is a very rare pathology that requires urgent surgical treatment. Most clinical cases described in the literature are elderly, and more than 70% present a history of rectal prolapse.3,4
Unlike traumatic perforations, the etiology of spontaneous presentations is unknown. Certain findings, such as the location of the perforation on the anterior side of the rectum and its association with difficult defecation, suggest a spontaneous rupture,5 as we suspected in the case of our patient. The main risk factor is rectal prolapse, but other risk factors have been described, such as increased depth of the rectovesical and rectovaginal spaces.6
There are several hypotheses that may explain the mechanism of spontaneous rectal perforation and intestinal evisceration. Wrobleski and Dailey report that, regardless of the mechanism involved, the sudden increase in intra-abdominal pressure seems to be the main contributing factor, violently pushing the ileal intestinal loops in the rectovesical or rectovaginal space and pressing on the anterior wall of the rectum.1 Additionally, the antimesenteric border of the rectum presents poorer irrigation. The traction generated by rectal prolapse can favor ischemia in this region and, consequently, perforation.7 Other etiological hypotheses include situations associated with excessive tension at the anterior side of the rectum or pre-existing rectal disease, such as diverticulosis, colitis, ulceration, adhesions or irradiation.8
Management of transanal bowel evisceration requires urgent surgery. The surgical procedure used to treat the rectal perforation and prolapsed bowel segment will depend on the contamination of the peritoneal cavity, intestinal viability, comorbidities and the hemodynamic state of the patient. The treatment of choice is resection of the perforated rectal segment and rectosigmoid anastomosis in a single operation.9 The alternative is a Hartmann's procedure with end colostomy and reconstruction of the tract in a second operation. In the case we present, we decided not to perform colorectal anastomosis because, at the time of surgery, the etiology of the perforation was unknown and we suspected the cause had been trauma-related.
In conclusion, transanal evisceration is an unusual surgical emergency. Elderly patients with chronic rectal prolapse and increased intra-abdominal pressure present higher risk. Evisceration usually occurs during the effort of defecation and involves abdominal pain and transanal protrusion of the bowel. As described in this case report, this pathology can also appear in young patients with no associated risk factors.
Please cite this article as: Salvador Rosés H, Falgueras Verdaguer L, Marinello F, Farrés Coll R, Codina Cazador A. Perforación rectal espontánea con evisceración transanal del intestino delgado. A propósito de un caso y revisión de la literatura. Cir Esp. 2017;95:299–301.
