






At all meetings of both the Abdominal Wall and Laparoscopy Groups in recent years, one of the topics being debated has always been what technique to use for mesh fixation during laparoscopic ventral hernia repair. This paper presents a combined fixation technique (mechanical suture/adhesive), based on the preliminary results obtained.
It is logical to accept that the natural tendency of abdominal wall surgery is to replace traumatic fixation devices (staples, tacks, transmural sutures, etc.), although there still is not enough scientific evidence available to do so.1 Currently, despite the fact that the use of adhesives in open or laparoscopic (totally extraperitoneal) inguinal hernia surgery can be viable and very attractive, in the laparoscopic approach to ventral hernia repair it seems very difficult to accept, a priori, due to the conditions of the technique itself.2–4 During open surgery, surgical glue can easily be distributed on a surface with maintained contact (muscle-mesh), providing total control of the quantity applied and direct verification of its effect. Meanwhile, in laparoscopic surgery, the glue has to be applied in a dome-shaped work area that is affected by gravity and provides no direct manual control. The pneumoperitoneum hinders the contact between the posterior abdominal wall and the mesh, which means that the glue applied to the mesh is not in contact with the abdominal wall for enough time (15–30s) to become effective (if we do not use direct pressure with a clamp). Furthermore, due to the effect of gravity, the adhesive material can drip directly onto the bowel loops, which may cause undetermined complications (obstruction, fistulas, perforations?) in the future.
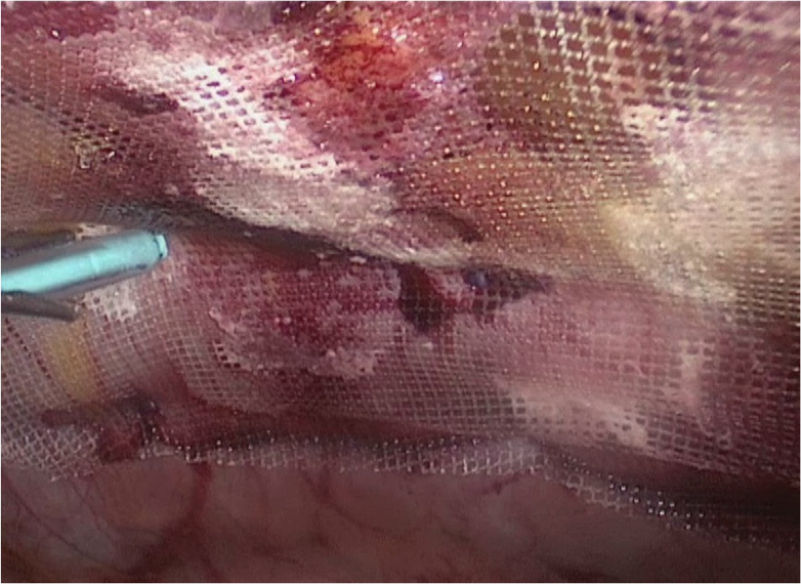
To avoid these problems, I have been modifying the standard fixation technique (double crown) for a combined technique that reduces the need for sutures to 4–6 anchors (Secure Strap™, Ethicon, USA) (Fig. 1) with the added use of surgical glue (Ifabond®, Fimed, Quincié-En-Beaujolais, France). This modification makes the procedure less expensive and improves the postoperative wellbeing of patients (Fig. 2). For the safe application of the glue (n-hexyl-α-cyanoacrylate), the mesh is always kept taught and in place with the standard 4 traction sutures at the vertices; it is later sutured at 4–6 equidistant points and later, with the help of a hepatic retractor, the mesh is kept in contact with the posterior abdominal wall and between the metal fingers of the retractor a thin film of surgical glue is applied (Fig. 3).5 Beforehand, one must be sure of having adequate omentum to cover the intestinal loops during the application of the product. The synthetic tissue adhesive used is a long-chain monomer with high purity and low viscosity that is polymerized in seconds and is completely reabsorbed within three months with no residues or peritoneal inflammation.
 to ensure contact of the mesh with the posterior abdominal wall.")
 guided by forceps, using a small amount that is well distributed to prevent it from dripping freely within the abdominal cavity.")
.")
This combined technique has been used by the author in 10 cases in the last 18 months in moderate mid-line ventral hernia repairs. There have been good results and no intra- or postoperative complications in a 6-month follow-up period (no postoperative ileus or obstructions, seromas, etc.), nor any recurrences. The effectiveness of the technique has been assessed in 3 ways: intraoperatively with manual traction before reducing the pneumoperitoneum, in the early post-op (one month) using dynamic ultrasound, and late post-op (6 months) by means of physical examination in order to rule out recurrence and tomography in case of doubt.
All patients were video-taped for postoperative follow-up and verification. Satisfaction during the postoperative period was very good, with hospital discharge between days 1 and 3. During the follow-up, no recurrences related to the new technique were observed. While we await better Velcro-type adhesives already incorporated into the mesh (without adding external elements) to avoid intra-abdominal manipulation, the variation of the technique presented herein has been demonstrated to be safe in the laparoscopic treatment of small-moderate mid-line ventral hernias, reducing the need for suture material and lowering the final cost of the procedure. We will analyze future results in order to verify whether this technique improves long-term recurrence rates and quality of life.
Please cite this article as: Moreno-Egea A. Sobre el uso de pegamento en la cirugía de las hernias. Técnica de fijación combinada en la eventroplastia laparoscópica. Cir Esp. 2014;92:57–58.
