





Pelvic fractures due to high energy trauma present a high risk of associated injuries that compromise the functional and vital prognosis of the patients. The objective of this study was to analyze the relationship between traumatic pelvic fractures and their associated injuries according to the Tile classification.
MethodsRetrospective observational study of patients who suffered traumatic pelvic fractures (Type A, B or C of the Tile classification) with concomitant associated injuries, analyzing hemoglobin levels, between 6/2013 and 1/2016.
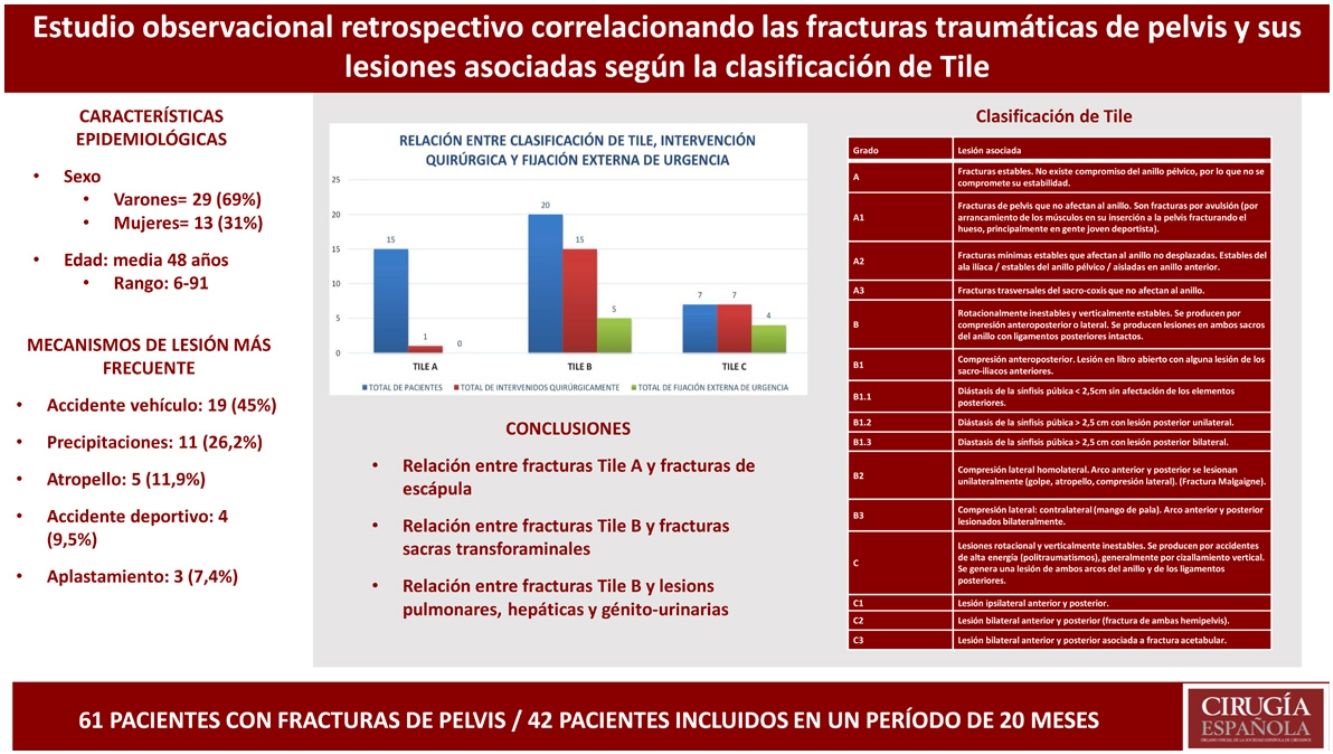
ResultsA total of 42 patients were included; of those 69% (n = 29) were males, mean age was 48 years. 45% (n = 19) suffered traffic accidents and 26.2% (n = 11) falls. There was a different proportion in pelvic injuries: Tile A (n = 15, 35.7%), B (n = 20, 47.6%), and C (n = 7, 16.6%) of cases. 54.8% (n = 23) underwent surgery, 21.4% (n = 9) needed temporary or definitive external fixation. Significant differences were found between Tile A type and scapula fractures (P = .032), and Tile B with sacral fractures (P = .033) and visceral injuries (P = .049), while there is a tendency without a statistical significal between Tile C and costal fractures. 61.9% (n = 26) needed blood transfusion; 9.5% (n = 4) presented hypovolemic shock.
ConclusionsTile A pelvic fractures were associated with scapular fractures, and Tile B with transforaminal fractures of the sacrum and with visceral injuries (lungs, liver and genitourinary). The small number of Tile C prevent us to confirm an association with any pathology, although they are the ones which presnt more hemodynamically instability and thoracic injuries.
Las fracturas de pelvis por traumatismo de alta energía presentan un alto riesgo de lesiones asociadas que comprometen el pronóstico funcional y vital. El objetivo de este estudio fue analizar la correlación entre las fracturas traumáticas de pelvis y sus lesiones asociadas según la clasificación de Tile.
MétodosEstudio observacional retrospectivo de pacientes que sufrieron fracturas traumáticas de pelvis (tipo A, B o C de la clasificación de Tile) con lesiones asociadas concomitantes, analizando los niveles de hemoglobina, entre 6/2013 y 1/2016.
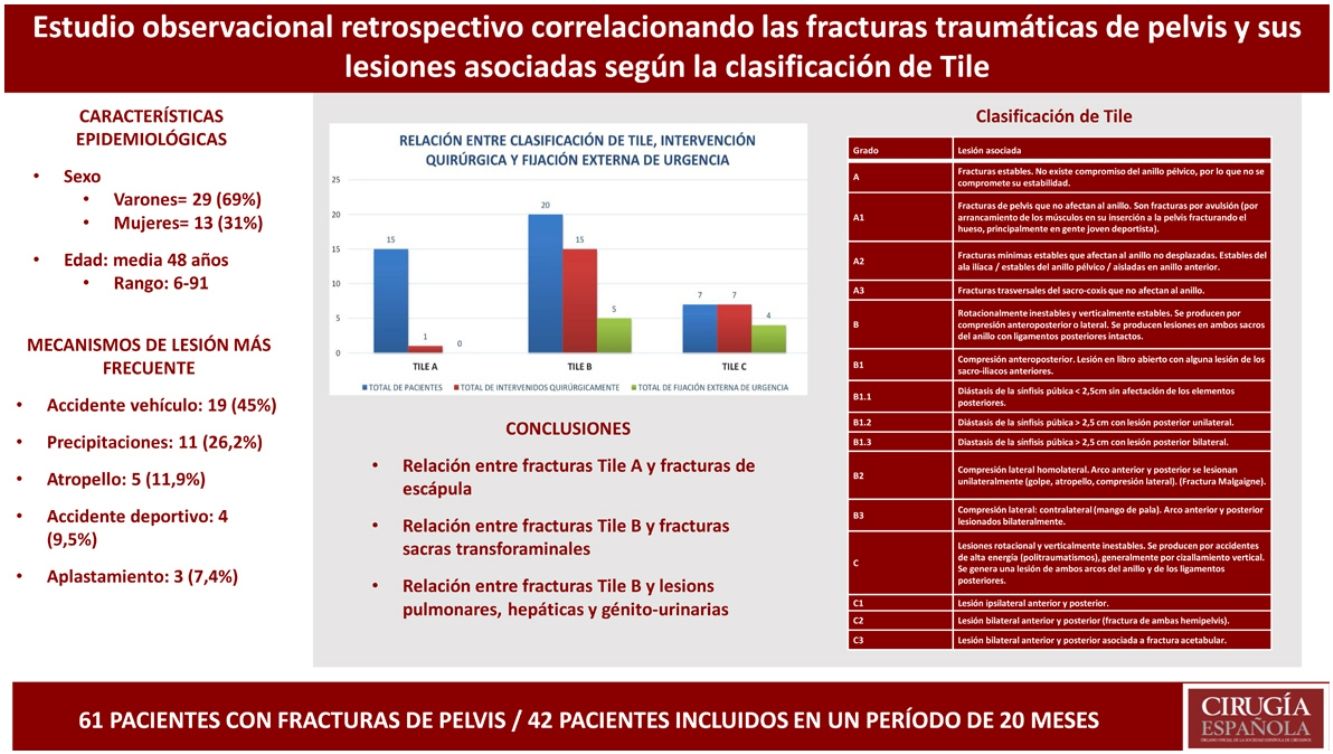
ResultadosSe incluyeron un total de 42 pacientes; de ellos, el 69% (n = 29) eran varones, la edad media era de 48 años. El 45% (n = 19) sufrió accidentes de tránsito; el 26,2% (n = 11) caídas. Hubo una proporción diferente en las lesiones pélvicas: Tile A (n = 15, 35,7%), B (n = 20, 47,6%) y C (n = 7, 16,6%) de los casos. El 54,8% (n = 23) fueron intervenidos quirúrgicamente, el 21,4% (n = 9) necesitó fijación externa. Se encontraron diferencias significativas entre las fracturas Tile A y de escápula (p = 0,032), y las Tile B con fracturas sacras (p = 0,033), y con lesiones viscerales (p = 0,049), mientras que existía solo una asociación sin significación estadística entre Tile C y fracturas costales. El 61,9% (n = 26) necesitó transfusión de sangre; el 9,5% (n = 4) presentó shock hipovolémico.
ConclusionesLas fracturas pélvicas Tile A se asociaron a las fracturas de escápula, y las Tile B con fracturas transforaminales del sacro y con lesiones viscerales (pulmonares, hepáticas y génito-urinarias). El número reducido de fracturas Tile C no permite realizar asociación estadística con ninguna enfermedad, si bien son las que presentan mayor alteración hemodinámica y lesiones torácicas.
Pelvic fractures should be separated into two groups: the first consisting of injuries that do not involve the pelvic ring, and the second including injuries to the pelvic ring. The latter are more complex because they are associated with serious trauma. Unstable pelvic ring injuries have significant mortality (4%–28%), and patients may present associated or secondary vascular, neurological, genitourinary and gastrointestinal lesions, as well as pain syndromes. Thorough clinical examination detects pelvic fractures with a sensitivity approaching 100%.1 In young patients, pelvic ring fractures are frequently caused by high-energy trauma. Pelvic fractures are also susceptible to large vessel injuries, and these patients may therefore present hypovolemic shock, possibly even resulting in death.2
The morbidity and mortality of several types of pelvic fractures have already been described in the current literature. However, little is known about their joint impact with associated injuries, or the role played by patient hemodynamic status upon admission to the Emergency Department. The objective of this study was to review and correlate different types of pelvic fractures according to the Tile classification with musculoskeletal, visceral, vascular and nerve injuries. We also analyze the impact on the hemodynamic status of these patients by studying hemoglobin levels at admission, before surgery, and at discharge from the intensive care unit.
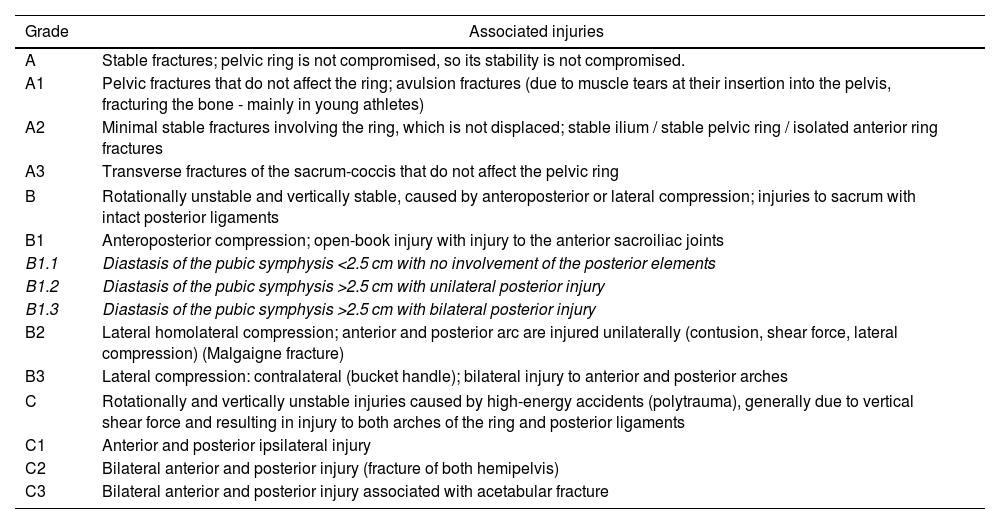
MethodsWe conducted a retrospective observational study of patients who had traumatic pelvic fractures (Type A, B or C of the Tile classification;3Table 1) with concomitant associated injuries, analyzing hemoglobin levels. The study was conducted from June 2013 to January 2016 and included patients who had consulted at or were referred to the Marqués de Valdecilla University Hospital.
Tile classification.
| Grade | Associated injuries |
|---|---|
| A | Stable fractures; pelvic ring is not compromised, so its stability is not compromised. |
| A1 | Pelvic fractures that do not affect the ring; avulsion fractures (due to muscle tears at their insertion into the pelvis, fracturing the bone - mainly in young athletes) |
| A2 | Minimal stable fractures involving the ring, which is not displaced; stable ilium / stable pelvic ring / isolated anterior ring fractures |
| A3 | Transverse fractures of the sacrum-coccis that do not affect the pelvic ring |
| B | Rotationally unstable and vertically stable, caused by anteroposterior or lateral compression; injuries to sacrum with intact posterior ligaments |
| B1 | Anteroposterior compression; open-book injury with injury to the anterior sacroiliac joints |
| B1.1 | Diastasis of the pubic symphysis <2.5 cm with no involvement of the posterior elements |
| B1.2 | Diastasis of the pubic symphysis >2.5 cm with unilateral posterior injury |
| B1.3 | Diastasis of the pubic symphysis >2.5 cm with bilateral posterior injury |
| B2 | Lateral homolateral compression; anterior and posterior arc are injured unilaterally (contusion, shear force, lateral compression) (Malgaigne fracture) |
| B3 | Lateral compression: contralateral (bucket handle); bilateral injury to anterior and posterior arches |
| C | Rotationally and vertically unstable injuries caused by high-energy accidents (polytrauma), generally due to vertical shear force and resulting in injury to both arches of the ring and posterior ligaments |
| C1 | Anterior and posterior ipsilateral injury |
| C2 | Bilateral anterior and posterior injury (fracture of both hemipelvis) |
| C3 | Bilateral anterior and posterior injury associated with acetabular fracture |
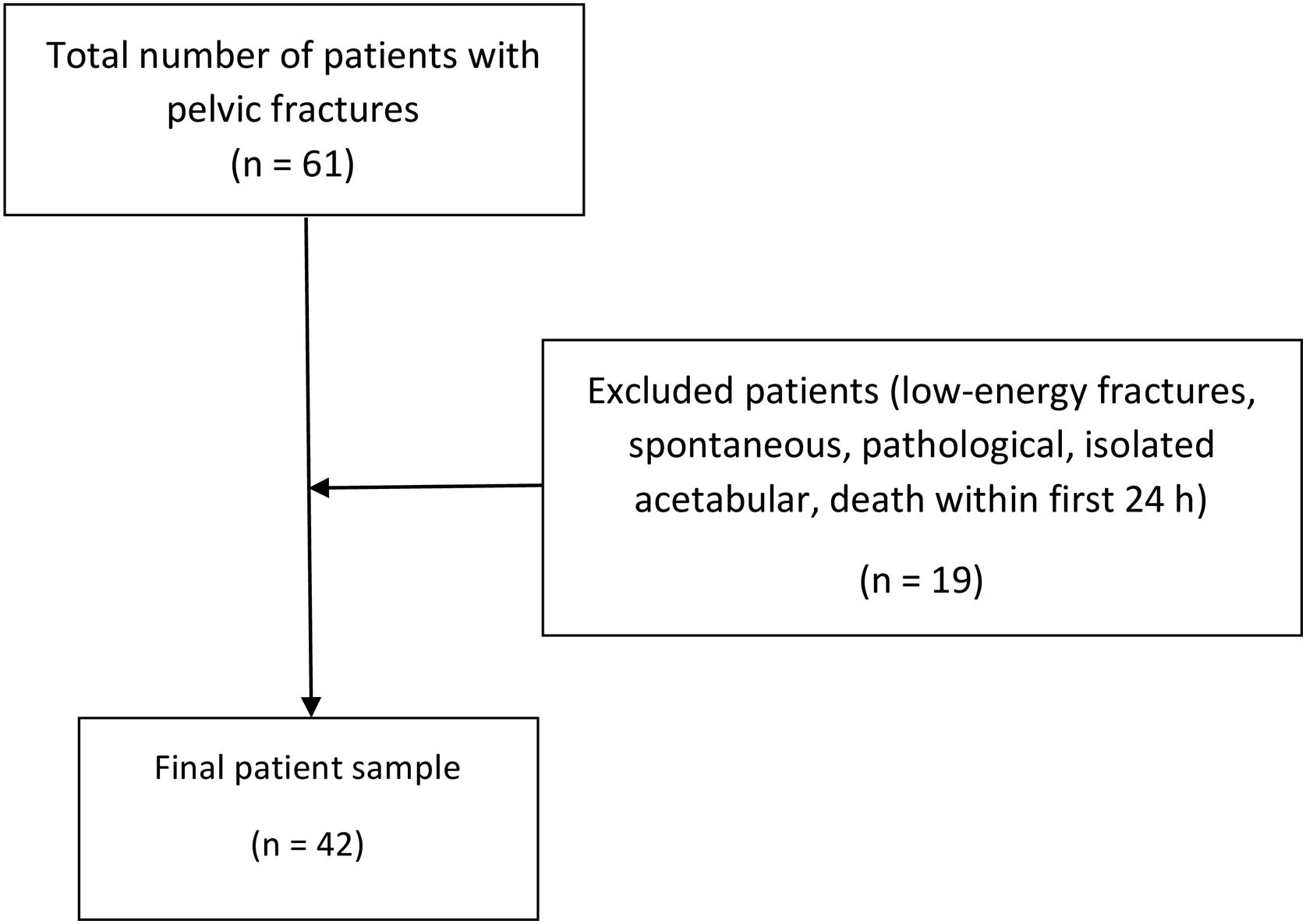
We identified all patients with pelvic fractures admitted to our hospital but only analyzed those that met the inclusion and exclusion criteria. Patients included in the analysis met at least one of the following inclusion criteria: high-energy pelvic fractures; associated musculoskeletal, visceral, and neurovascular injuries; diagnostic CT or MCT scans of the pelvis; surgical treatment or conservative management by the Trauma Unit. The exclusion criteria were: low-energy fractures (accidental falls from a standing position); spontaneous fractures; pathological fractures; patient death within 24 h after the event; and isolated acetabular fractures.
The percentage of patients with pelvic fractures according to the Tile classification was considered the main variable, and the percentages of musculoskeletal, visceral and vascular-nervous injuries associated with high-energy pelvic fractures were secondary variables.
Measurement parameters were age, sex, fracture mechanism, Tile pelvic fracture classification, surgical procedure or conservative approach, emergency external fixation, type of surgery (open reduction and internal fixation, or ORIF) if performed, traumatic brain injury (TBI), associated injuries (musculoskeletal, visceral, vascular, nervous), hypovolemic shock, neurogenic shock, hemoglobin (Hb) on admission to the ward or ICU, need for blood transfusion (red blood cells, polytransfusion), and blood pressure on admission to the emergency room or ICU.
Hemoglobin levels were measured at the time of hospital admission, discharge or before surgery (if performed), moments that were selected to avoid the appearance of lower Hb levels that could have been due to blood loss during surgery and not from the typical bleeding of a pelvic fracture.
Statistical analysisThe statistical analysis was performed using Pearson’s chi squared, Fisher’s test and logistic regression analysis for the study of qualitative data, and the Kruskal-Wallis analysis for the comparison of quantitative and qualitative data. We assessed the possible correlations between the type of pelvic fracture according to the Tile classification, mechanism of injury, treatment performed, associated injuries, hemodynamic status on admission and discharge, and the need for transfusion during hospital stay. Differences were considered statistically significant with a P value less than 0.05.
ResultsA total of 61 patients with pelvic fractures were identified. After applying the exclusion criteria, the final sample consisted of 42 patients (Fig. 1). In terms of distribution by sex, we found a greater number of male patients than females (males = 29, 69%; females = 13, 31%). Regarding age, the patients included had a mean age of 48 years (range: 6–91). Out of the total of 42 patients, 15 (35.7%) were type A according to the Tile classification, 20 (47.6%) were B, and 7 (16.6%) C.

Regarding the mechanisms of injury causing the fractures, the following data were recorded: 19 (45%) were traffic accidents (12 automobile and 7 motorcycle); 11 (26.2%) were falls (2 occupational accidents and 9 suicide attempts); 5 (11.9%) were pedestrians hit by a vehicle; 4 (9.5%) were due to sporting accidents (3 horseback riding and 1 surfing); and 3 (7.4%) had been crushed.
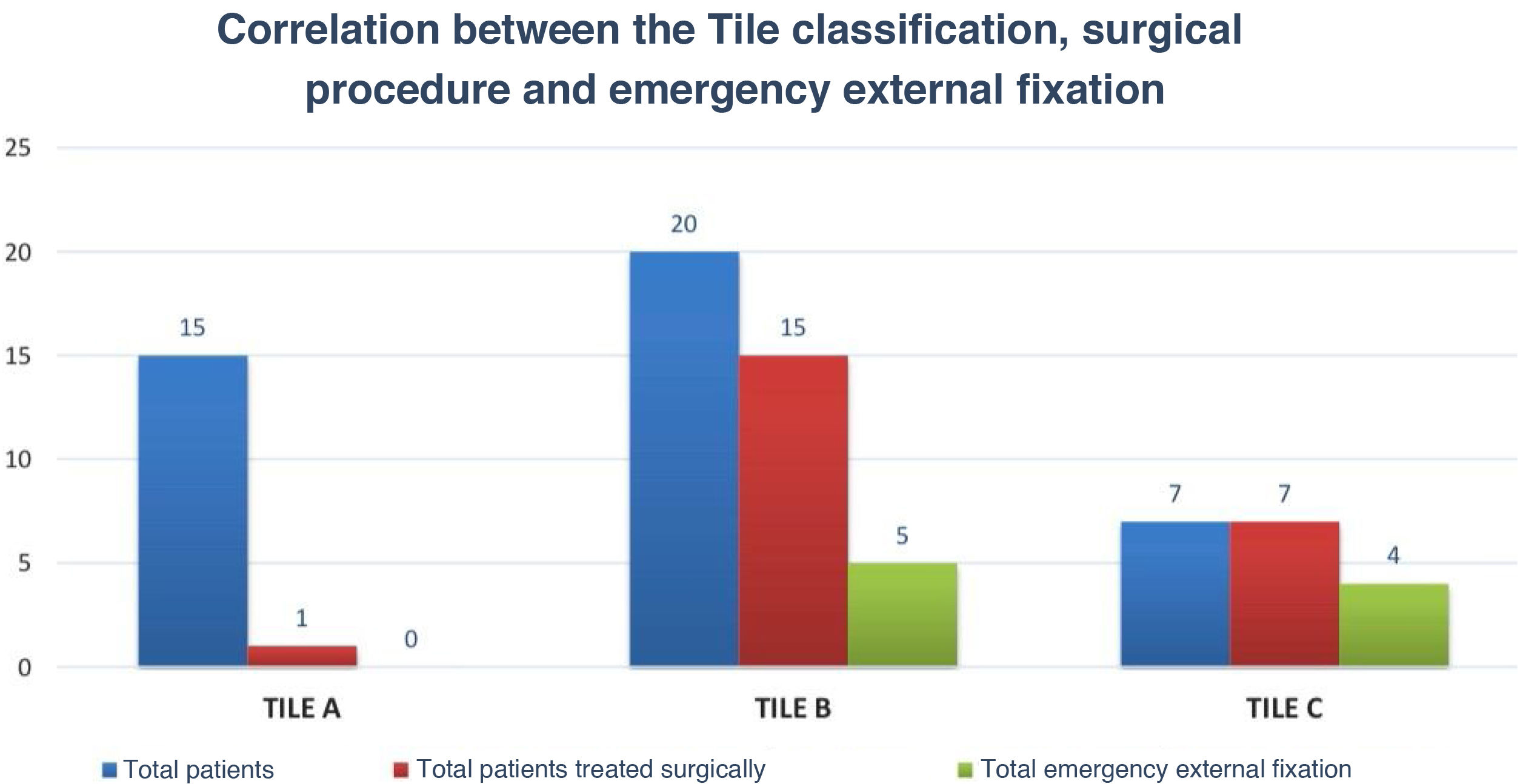
In the caseload reviewed from the years of the study period, no open fractures were found. In total, 23 patients (54.8%) underwent surgery, and 9 (21.4%) required temporary or definitive external fixation (Fig. 2). By tile classifications, out of all the 15 Tile A patients, only one underwent surgery; out of the 20 Tile B patients, 15 underwent surgery; and out of the 7 Tile C patients, all of them required surgery. When both groups were compared between the total of those who underwent surgery and the total of emergency external fixation in each type of Tile fracture, we found that only Tile C shows a statistically significant difference (Tile A: 1/15 [6.67%] vs 0/15 [0%], P < 1.00; Tile B: 15/20 [75%] vs 5/20 [25%], P < .0038; Tile C: 7/7 [100%] vs 4/7 [57.1%], P < .1923). Out of the 26 patients (61.9%) who required transfusion, only 4 (9.5%) suffered from hypovolemic shock. No relationship was found between the need for blood transfusion and the Tile classification, nor was any case of neurogenic shock found among the patients studied.

No statistically significant differences were found for sex, age, fracture mechanism or the presence/absence of TBI with respect to each Tile grade. Tables 2 and 3 show the relationship between injuries and fractures in general with each type of Tile fracture. Regarding vascular injuries, one Tile B type case presented a dissected left external iliac vein. The remaining vascular injuries were not located in the pelvic region but were instead related with associated fractures in other locations or with intraperitoneal hematomas due to bleeding caused by mesenteric or hypogastric artery injuries. In one of the Tile C cases, the patient had thrombosis of the left arterial axis in the femoropopliteal transition (arterial and venous dissection at the popliteal level). Most of the nerve injuries were at the S1 (2 cases), the external popliteal sciatic nerve (2 cases), T12-L2 (1 case), or injuries of the radial, median and ulnar nerves associated with fractures in other locations.
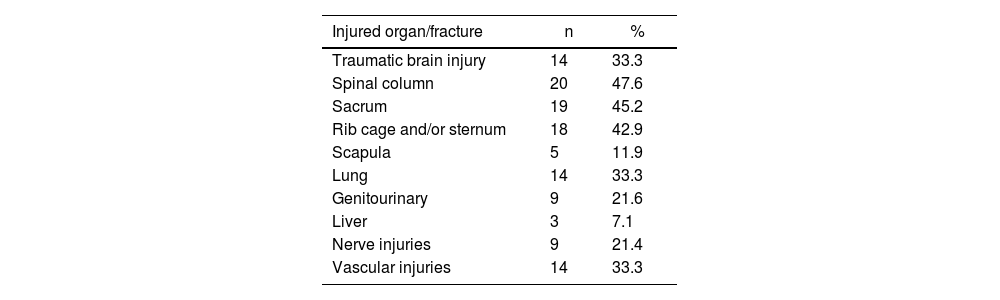
Injuries associated with pelvic fractures, regardless of type.
| Injured organ/fracture | n | % |
|---|---|---|
| Traumatic brain injury | 14 | 33.3 |
| Spinal column | 20 | 47.6 |
| Sacrum | 19 | 45.2 |
| Rib cage and/or sternum | 18 | 42.9 |
| Scapula | 5 | 11.9 |
| Lung | 14 | 33.3 |
| Genitourinary | 9 | 21.6 |
| Liver | 3 | 7.1 |
| Nerve injuries | 9 | 21.4 |
| Vascular injuries | 14 | 33.3 |
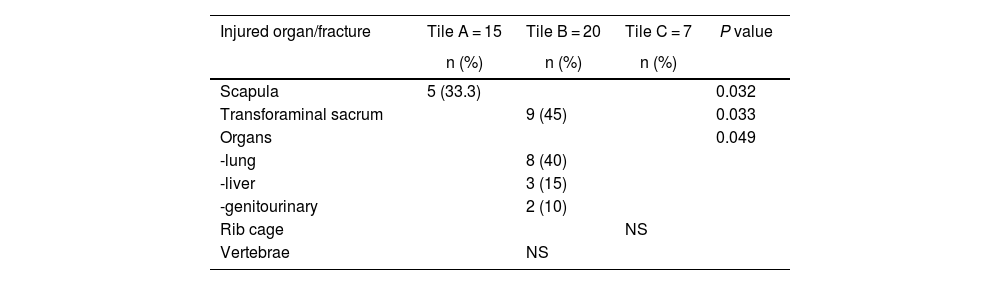
Injuries associated with pelvic fractures according to type.
| Injured organ/fracture | Tile A = 15 | Tile B = 20 | Tile C = 7 | P value |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Scapula | 5 (33.3) | 0.032 | ||
| Transforaminal sacrum | 9 (45) | 0.033 | ||
| Organs | 0.049 | |||
| -lung | 8 (40) | |||
| -liver | 3 (15) | |||
| -genitourinary | 2 (10) | |||
| Rib cage | NS | |||
| Vertebrae | NS |
NS: not statistically significant.
Table 4 shows the mean Hb values of the patients in each group (Tile A, B, or C) at the time of admission and at discharge or preoperative, as well as the ranges of minimum and maximum Hb values recorded for each patient, with standard deviations.
Mean hemoglobin levels at hospital admission and discharge or pre-op, and range.
| Tile classification | n | Mean Hb on admission | Min | Max | SD | Mean Hb at discharge or pre-op | Min | Max | SD |
|---|---|---|---|---|---|---|---|---|---|
| Tile A | 20 | 11.8 | 6.7 | 16 | 2.33 | 9.4 | 7.6 | 13.5 | 1.48 |
| Tile B | 15 | 11.6 | 7.5 | 15.2 | 1.93 | 11.2 | 8 | 14.9 | 1.73 |
| Tile C | 7 | 10.4 | 7.6 | 13.3 | 1.43 | 9.3 | 7.7 | 13.3 | 1.4 |
Hb: hemoglobin; Min: minimum; Max: maximum; SD: standard deviation; pre-op: preoperative.
When we analyzed the correlation between the associated musculoskeletal injuries and each type of Tile fracture grade (A, B or C), our study showed statistically significant results between Tile A fractures and scapular fractures. Likewise, Tile B fractures were related to transforaminal sacral fractures. As for Tile C fractures, a statistical trend was found between these and rib injuries. The same is true for Tile B fractures and vertebral fractures. Regarding visceral injuries, a statistical association was found with Tile B fractures and pulmonary or hepatic contusions and genitourinary injuries.
Since no association was found between Hb levels at admission and the type of fracture, nor between Hb levels before surgery or at discharge and the fracture type, a relationship between Tile fracture type and blood volume loss cannot be confirmed.
Several studies4–8 have reported on the importance of managing polytrauma patients with pelvic fractures and other injuries. Others compare the different surgical techniques performed for these fractures and also the impact of associated injuries on short- and medium-term mortality, but there are very few that specifically focus on the correlation between the severity of pelvic fractures and the other associated injuries of these patients. This may be influenced by the progressive decline in the incidence in recent years, which is due in part to the increase in prevention plans for both occupational and traffic accidents in various countries.
In this type of fractures in polytrauma patients, the importance of early action has been demonstrated when associated injuries are suspected in other areas, depending on symptoms and the Tile pelvic fracture grade. Sánchez-Tocino et al7 retrospectively studied 1274 severe polytrauma patients between 1993 and 2005, 192 of whom (15%) had pelvic fractures, and 93.3% of which were associated with other injuries. The age range of these patients was from 15 to 91 years; 64% were male and 36% female. The most frequent injury mechanism was traffic collisions of varying types, followed by falls. In very few cases did patients undergo digital rectal examinations or the placement of a non-invasive pelvic device, such as a sheet or similar for temporary closure of the pelvis. The pelvic fractures were classified according to the Tile classification as: 126 (65.5%) type A, 40 (21%) type B, and 26 (13.5%) type C. Similar to our results, musculoskeletal injuries and specifically chest trauma (70%) were the most frequent associated injuries and, among these, rib fractures accompanied by pneumothorax and/or massive pulmonary contusion were most common. Abdominal injuries (55%) were next in frequency, and the liver was the most frequently damaged solid organ followed by the spleen, genitourinary injuries (21%, vesicourethral rupture in 8%), long bone fractures (52%) and TBI (40%). In addition, 23% of the patients presented retroperitoneal hematoma.
Demetriades et al.9 described the liver as the most frequently affected intra-abdominal viscera in stable pelvic fractures, and the bladder-urethra when only unstable pelvic fractures were analyzed. In the series by Rieger et al.,10 the spleen, followed by the liver, were the most frequently injured organs. Kwon et al11 conducted a study at the Ulsan University Hospital in Korea between 2000 and 2011, including 386 patients with pelvic fractures, and observed that the liver was the most frequently affected solid abdominal organ, followed by the spleen and kidneys.
Chien-Lung et al.,1 however, described lower-extremity fractures (21.5%) as being most frequently associated with pelvic fractures, followed by vertebral and thoracic fractures (20.9%), upper extremity fractures (18.2%), TBI (17.6%), abdominal and pelvic organ injuries (11.1%) and thoracic organ injuries (7.2%). Similar to our results, Frawley et al12 found no statistically significant differences between fracture mechanisms (traffic collisions, falls, etc) and fractures recorded (P = .36).
Marini et al.,13 in their study of 979 patients with pelvic fractures stratified according to the presence or absence of solid organ injury, described solid organ injuries as the most frequently associated, specifically (in decreasing order) the spleen, liver and kidney, followed by chest injuries.
Giannoudis et al14 went further by correlating the associated injuries with the survival of the groups, finding a higher incidence of thoracic, abdominal and TBI injuries in the group of patients who died compared to those who survived the event, results which were statistically significant. Furthermore, the study correlated the associated injuries with patient severity and risk of death, thereby demonstrating the importance of their early detection.
We have found no studies comparing the Tile Classification with associated injuries. Two authors, Starr15 and Black16, correlated these associated injuries with the Young classification and not Tile, which has prevented a comparison with our study, in addition to the exclusively open fractures of the Black study.
Limitations of this studyThe sample size has been one of the limitations of this study, especially the low number of Tile C fractures, compared to the large number of variables studied. We believe that this has affected the statistical significance of the results, finding instead a statistical trend in some cases.
ConclusionsIn our study, we have found a relationship between Tile A pelvic fractures and scapular fractures, as well as between Tile B and transforaminal sacral fractures and lung, liver, and genitourinary injuries. As for Tile C, only a trend was observed with chest wall injuries, which did not reach a statistically significant difference. Further studies would be recommended with a greater number of Tile C type fractures to arrive at conclusive results. These findings allow us to direct our examination and diagnostic methods towards this type of associations, which would result in the selection of the correct methods and the appropriate treatment for this type of patient.
FundingNo public or private funding was received.
Conflicts of interestThe authors have no conflicts of interest to declare.
