





Outpouching of the left ventricle is a rare condition with heterogeneous causes ranging from congenital abnormalities, such as diverticula or muscle bands, to complications secondary to myocardial infarction, such as aneurysm and pseudoaneurysm. Distinguishing among these etiologies is challenging but of great clinical importance given the wide range of risks and implications involved.1–3
Double chambered is a term that has been used to describe the subdivision of a ventricle as a result of anomalous septum or muscle bundle. Subdivision of the left ventricular cavity is a rare cardiac anomaly compared with subdivision of the right ventricle.3
Cardiac magnetic resonance imaging (CMRI) is useful in the assessment of associated conditions and to better understand the disease, characterizing the diagnosis. CMRI can demonstrate changes in the ventricular contractility, presence or absence of fibrosis and is useful in the follow-up of patients with double-chambered left ventricle (DCLV).3,4
We describe a case of DCLV, highlighting the importance of CMRI, clinical evolution, and outcome.
CASE PRESENTATIONA 29-year-old sedentary man presented to the emergency room an hour after developing chest pain that radiated to the inner side of the left arm. The patient was administered acetylsalicylic acid and nitrate and symptoms soon improved. The patient had no family history of coronary artery disease (CAD), had smoked a pack of cigarettes a day for the past 10 years, and was obese and hypertensive (140/95 mmHg). Physical examination revealed no cardiac murmur and the electrocardiogram (EKG) was normal, but plasma cardiac necrosis markers were elevated. Although thoracic window acquisition was difficult, echocardiogram examination revealed no abnormalities and global LV function was normal. After the pain had subsided, the patient was discharged and directed to consult a cardiologist.
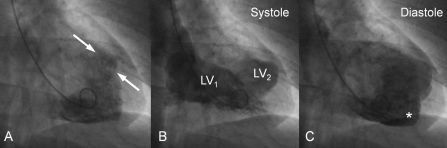
Based on the necrosis marker changes and presence of type-B pain on that day, the cardiologist recommended a stress test, but the patient was unable to meet the physical requirements for accurate evaluation. In the absence of a stress test, an invasive coronary angiography (ICA) was requested. ICA revealed normal coronary arteries, but ventriculography showed an outpouching on the left ventricle that was thought to be an aneurysm (Fig. 1).
 of the LV1.")
Further investigation was performed in a 1.5-Tesla MRI scanner (Avanto, Siemens Medical Solutions, Erlangen, Germany) with a four-element phased-array cardiac coil using perfusion, cine-Steady-state free precession (SSFP) and delayed-enhancement sequences. MRI results confirmed the presence of the pouch, appending to the posterior and lateral wall of the left ventricle (Fig. 2). It measured 5.8 cm in the long-axis view and 2.4 cm in the short axis.
 does not fill in with contrast. B, The second moment shows that the gadolinium fills the LV2 but with less concentration than LV1. C, The third moment both cavities has the same signal intensity. D, There is no perfusion defect on the lateral wall of the LV2 and also at the whole myocardium.")
Cardiac magnetic resonance imaging with the perfusion technique on the same slice position of one short axis view. A, The gadolinium is first inside of the LV1. LV2 (*) does not fill in with contrast. B, The second moment shows that the gadolinium fills the LV2 but with less concentration than LV1. C, The third moment both cavities has the same signal intensity. D, There is no perfusion defect on the lateral wall of the LV2 and also at the whole myocardium.
As seen in Fig. 3, the pouch was separate from the apex. The wall thickness of the thinner segment of LV2 was 5 mm in end diastole, a little bit less than the remaining left ventricular myocardium.
 with the cine (A, B, D, and E) and late enhancement (C and F) techniques. A, Cine-MRI, short-axis view at the apical portion of the left ventricle (LV) showing both cavities. B, Cine-MRI, short axis view at the middle portion of LV showing both cavities. C, Delayed enhancement, short-axis view at the middle portion of LV without scar/fibrosis. D, Cine-MRI four-chamber view at diastole showing both cavities. E, Cine-MRI, four-chamber view at systole showing the thickening of the lateral wall of the LV2. F, Delayed enhancement, four-chamber view without scar/fibrosis.")
Cardiac magnetic resonance imaging (MRI) with the cine (A, B, D, and E) and late enhancement (C and F) techniques. A, Cine-MRI, short-axis view at the apical portion of the left ventricle (LV) showing both cavities. B, Cine-MRI, short axis view at the middle portion of LV showing both cavities. C, Delayed enhancement, short-axis view at the middle portion of LV without scar/fibrosis. D, Cine-MRI four-chamber view at diastole showing both cavities. E, Cine-MRI, four-chamber view at systole showing the thickening of the lateral wall of the LV2. F, Delayed enhancement, four-chamber view without scar/fibrosis.
The majority of the pouch was found to be contractile. In the short-axis view, the myocardium separating both chambers and a systolic flow jet leaving the pouch and entering the primary LV chamber were noted.
The cine sequences showed normal left ventricular contraction (ejection fraction 51%). The pouch exhibited normal systolic contraction without any regional wall motion abnormality.
After injection of Gadolinium - diethylenetriamine penta-acetic acid (Gd-DTPA), the first pass perfusion in the short-axis view displayed normal myocardial perfusion. Late enhancement of the short and long axes revealed no myocardial scarring.
The patient was diagnosed with a congenital DCLV. He was instructed to undergo diet and exercise and follow up with a cardiologist to ensure that symptoms and cardiac function remain under control.
DISCUSSIONDCLV is characterized by the division of the ventricular chamber into two chambers by abnormal muscular tissue. It is best differentiated from left ventricular aneurysms and pseudoaneurysms by the fact that the double-chambered ventricle exhibits contractile motion during systole. Ventricular aneurysm lacks complete layering of the ventricular wall, and thus expands slightly due to the increased pressure during systole.5,6
The differentiation between double-chambered left and right ventricles is clear as they have different pathophysiology. Double-chambered right ventricle (DCRV) is more common and often presents with murmur and exertional dyspnea. Studies have found that DCRV is associated with septal defects, tetralogy of Fallot, and transposition of the great arteries. Conversely, DCLV is commonly asymptomatic. DCRV is often caused by a progressive thickening of the right ventricular septum due to the presence of anomalous muscle bundles. This causes a pressure gradient, and two chambers in series develop. In contrast, the chambers of a DCLV are in parallel and present less of a pressure gradient, as both contract synchronously. The DCLV etiology is less well known, but the anomaly is thought to be congenital and non-progressive.4,7,8
Usually, DCLV is incidentally found in the course of an evaluation for other cardiovascular abnormalities. As this is an extremely rare finding, no definite data regarding the prognosis, outcomes and potential complications, such as risk of embolism, of DCLV are available. It is generally believed that DCLV poses little risk to the patient. Treatment, if any, is usually guided by the presence of other associated abnormalities.2,9,10
The CMRI with the normal delayed enhancement images suggested that the patient had not suffered a myocardial infarction. Additionally, there were no signs of fibrosis on the myocardium, even near the outpouching. This rules out the possibility that the pouch was formed as a result of trauma or infarction, and suggests that the pouch's origin is congenital. Through examination of the four-chamber sequence, the pouch is seen to have a fully developed myocardial wall that contracts synchronously with the rest of the myocardium. During systole, one area of the pouch's myocardial wall appears thinner, but the delayed enhancement image verifies that the wall muscle is in fact fully developed in that region. This excludes the possibility of one aneurysm.4,6,11,12
We believe the misdiagnosis was probably due to a poor thoracic window that did not yield proper diagnostic-quality images of this condition.
There is not too much data stating the importance of other non-invasive methods but it is reasonable to assume that echocardiography and computed tomography can aid in detection of double-chambered ventricles. However, MRI allows a better delineation of this condition because of its higher spatial resolution and the ability for tissue characterization, especially regarding the differentiation between fibrosis and normal myocardium, which would not be easily achievable on echocardiography and CT.
Because of the rarity of DCLV, few data exist on treatments and outcomes. Surgical excision of the accessory chamber with interposition patch reconstruction and cardiac transplant are two valid options.4,5
In the case presented, normal ejection fraction and wall motion are positive signs, suggesting that the patient's condition is not immediately life threatening, eliminating the need for surgical intervention. One concern is the possibility that a clot will form in the minor ventricle, although in the patient's case good blood flow through the communication gap lessens that risk. The patient was discharged and told to follow up with his cardiologist; 7 months of follow up have now passed without any clinical symptoms.