




Chemical pleurodesis is an important therapeutic tool to control recurrent malignant pleural effusion. Among the various sclerosing agents, iodopovidone is considered effective and safe. However, in a recent study, ocular changes were described after iodopovidone was used in recurrent pneumothorax. The aim of the study was to evaluate the efficacy and morbidity of iodopovidone pleurodesis in an experimental model.
METHODSNew Zealand rabbits were submitted to intrapleural injection of iodopovidone at concentrations of 2%, 4% and 10%. Biochemical (lactic dehydrogenase, proteins, triiodothyronine, free thyroxine, urea and creatinine) and immunological (Interleukin-8 [IL-8], VEGF and TGFβ) parameters were measured in the pleural fluid and blood. After 1, 3, 7, 14 and 28 days, groups of animals were euthanized, and macro- (pleura) and microscopic (pleura and retina) analyses were performed.
RESULTSAn early pleural inflammatory response with low systemic repercussion was observed without corresponding changes in thyroid or renal function. The higher concentrations (4% and 10%) correlated with greater initial exudation, and maximum pleural thickening was observed after 28 days. No changes were observed in the retinal pigment epithelium of the rabbits.
CONCLUSIONIodopovidone is considered to be an effective and safe sclerosing agent in this animal model. However, its efficacy, tolerance and safety in humans should be further evaluated.
Despite the preferential use of long-term catheters to control recurrent malignant pleural effusions, chemical pleurodesis persists as an important therapeutic tool. The ideal sclerosing agent should be inexpensive, widely available and easily managed, in addition to low morbidity and the absence of mortality. Although pleurodesis was first performed at the beginning of the 20th century using silver nitrate, talc progressively gained wide preference (1,2). Nevertheless, despite impressive results, the heterogeneity of talc particles has been implicated in causing undesirable side effects, sometimes culminating in respiratory failure and death (3,4).
These facts have stimulated clinical and experimental studies to reevaluate the effectiveness and safety of previously used sclerosing agents, such as iodopovidone, a topical antiseptic that is recognized as a safe (minimal side effects) and effective (>90%) (5), although visual loss has been reported by Wagenfeld et al. (6). It should be highlighted that the dose reported in this study was higher than the standard dose that has been used in other clinical studies (7–9).
The purpose of this study was to evaluate pleurodesis development in an animal model and to analyze the possible systemic effects after intrapleurally injecting iodopovidone.
MATERIALS AND METHODSThis project was developed at the Pleura Laboratory of the Pulmonary Division of the Heart Institute (HC-FMUSP) after approval by the Ethics Committee Board. New Zealand rabbits (2.0-3.0 kg) were randomized and subdivided into groups (five animals each) according to the time of euthanasia (1, 3, 7, 14 or 28 days).
As previously described, the animals were submitted to sedation and analgesia (35 mg/kg of ketamine hydrochloride [Cristalia, Brazil] and 5 mg/kg of xylazine hydrochloride [Bayer, Brazil]) (10–12). Next, trichotomy of the right hemithorax and antisepsis were performed; a 0.5 cm incision (hemiclavicular line) was then made over the projection of the sixth rib. A catheter (8 Fr) was then tunneled into the subcutaneous tissue, and after exposing the parietal pleura, it was inserted into the cavity and attached to the skin. Through the catheter, 2 mL of iodopovidone (Rioquimica, Brazil) was injected at 2%, 4% or 10% concentrations. The left hemithorax (not injected) was used as a control.
Every 24 hours, the drain was aspirated, and the pleural fluid was quantified and stored with concurrently collected blood samples. The drain was removed after the seventh day, when the fluid drainage was <1 mL/day. At the predetermined times, the animals were euthanized; the thorax was removed en bloc, and the lungs were expanded and maintained submersed (10% formalin) for 48 hours. Next, the pleural cavity was exposed for macroscopic evaluation (10–12). For histological analysis of the retina, the rabbit eyes were enucleated and fixed (10% formalin) for slide preparation and Hematoxylin & Eosin (H&E) staining.
Lactic dehydrogenase (kinetic UV method), total protein (Biuret method), and the Interleukin-8 (IL-8), VEGF and TGF-β1 (ELISA method) cytokines were quantified in the blood and pleural fluid. Thyroid hormone levels (triiodothyronine and free thyroxine) in the blood was detected using chemiluminescence (ImmuLITE 2000, Siemens, Erlangen, Germany), and the levels of renal function markers (urea and creatinine) were determined with the kinetic UV method.
Baseline serum levels were obtained from the rabbits prior to iodopovidone treatment and were used as the control.
Macroscopic and microscopic evaluations were performed according to previously described methodology (10–12). A consensus grading of the macroscopic adhesions was reached by two investigators (LRT and JP) who were blinded with respect to the treatment group using the semi-quantitative scheme: (0) normal pleural space, (1) 1-3 small adherences, (2) over 3 adherences in which the lung can easily be separated from the thorax, (3) generalized adhesions (containing areas where the lung could only be separated from the thoracic wall with difficulty) and (4) complete obliteration of the pleural space by adhesions. The pleura visceral fragments were processed, stained (hematoxylin–eosin), and evaluated for the presence of thickening using grades from 0-4: 0 = none, 1 = equivocal, 2 = mild, 3 = moderate and 4 = marked changes. The microscopic analysis was performed by two examiners (LA and MMPA) who were blinded to the treatment. Retina fragments were also H&E stained and analyzed with light microscopy by two independent investigators (LRT and FMD).
Statistical AnalysisThe results are presented as median and interquartile range (25%-75%). Comparisons among the three groups were performed using non-parametric tests (the Mann-Whitney rank sum test or Kruskal-Wallis analysis of variance on ranks). A value of p<0.05 was considered significant. The SigmaStat 3.1 (Systat, CA, USA) program was used for the analyses.
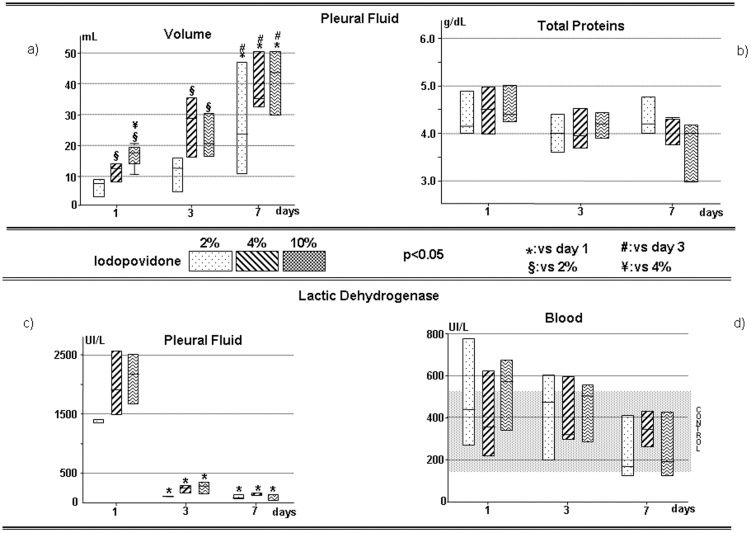
RESULTSFigure 1 shows the characteristics of the inflammatory response after the iodopovidone instillation. Progressive pleural exudation was observed, with maximum fluid drainage at seven days (2%, 23 mL [11-46 mL], p = 0.035; 4%, 34 mL [32-44 mL], p = 0.003 and 10%, 43 mL [29-49 mL], p = 0.004). On the first (p<0.001) and third (p = 0.045) days following the pleural injection, the fluid produced with 4% and 10% iodine was superior to that produced with 2% iodine. After the seventh day, the pleural fluid markedly diminished in the majority of the animals, regardless of the concentration; this result precluded the statistical analyses in the groups. There were no differences in the protein levels among the groups. Regardless of the injected concentration, a marked elevation of lactic dehydrogenase was evident only in the pleural fluid. Twenty-four hours following the instillation, the levels were significantly greater than those obtained after three days (2%, p<0.001; 4%, p = 0.003 and 10%, p = 0.002) or seven days (2%, p<0.001; 4%, p = 0.003 and 10%, p = 0.002).
 of the pleural fluid volume and biochemical analyses during the acute phase of the iodopovidone intrapleural injection (1, 3 and 7 days). (a) The volume of pleural fluid collected. (b) The total protein levels in the pleural fluid. (c) Lactic dehydrogenase in the pleural fluid. (d) Lactic dehydrogenase levels in the blood.")
Results (median and interquartile range 25%-75%) of the pleural fluid volume and biochemical analyses during the acute phase of the iodopovidone intrapleural injection (1, 3 and 7 days). (a) The volume of pleural fluid collected. (b) The total protein levels in the pleural fluid. (c) Lactic dehydrogenase in the pleural fluid. (d) Lactic dehydrogenase levels in the blood.
Cytokine behavior is shown in Table 1. When the cytokine levels in the pleural fluid and blood were compared on the first day after injection, the IL-8 pleural was greater (2%, p = 0.003; 4%, p = 0.015 and 10%, p<0.001). After this initial increment, the pleural levels decreased beginning with the third day and stabilized until the seventh day. At this time, the IL-8 values were lower than those obtained in the blood (4%, p<0.001 and 10%, p = 0.049). In all of the evaluated periods, the serum levels were significantly greater than the baseline level of 26 pg/mL (16-55).
The median and interquartile (25%-75%) f cytokine levels in the pleural fluid and blood during the acute phase of iodopovidone intrapleural injection (1, 3 and 7 days), p<0.05 (∗vs. day 1; # vs. day3; § vs. 2%).
| Pleural Fluid | Blood | |||||||
|---|---|---|---|---|---|---|---|---|
| 2% | 4% | 10% | p | 2% | 4% | 10% | p | |
| IL-8 (pg/mL) | ||||||||
| Basal | 26 (16-55) | |||||||
| Day 1 | 2866 (2779-3459) | 3961 (2044-4273) | 4253 (3292-4443) | 0.587 | 1362 (1083-1703) | 1344 (1022-1531) | 1664 (1557-2115) | 0.121 |
| Day 3 | 1083 (874-1107)∗ | 921 (883-990)∗ | 1189 (617-1551)∗ | 0.733 | 875 (556-1684) | 1395 (978-1695) | 1981 (1796-2062) | 0.101 |
| Day 7 | 776 (535-953)∗ | 747 (630-818)∗ | 761 (662-1475)∗ | 0.455 | 1121 (402-1973) | 1270 (988-1343) | 2321 (1173-2642) | 0.289 |
| p | 0.007 | 0.003 | <0.001 | 0.849 | 0.913 | 0.802 | ||
| VEGF (pg/mL) | ||||||||
| Basal | 31 (31-34) | |||||||
| Day 1 | 332 (233-583) | 626 (527-763) | 525 (470-889) | 0.117 | 34 (30-37) | 53 (39-56) | 33 (22-54) | 0.629 |
| Day 3 | 602 (516-656) | 462 (428-950) | 1192 (793-1304) | 0.069 | 45 (31-45) | 49 (36-84) | 85 (53-94) | 0.328 |
| Day 7 | 1483 (610-1545)∗ | 1882 (1783-2959)∗ | 2627 (1717-3420)∗ | 0.064 | 31 (31-41)∗ | 44 (37-45) | 67 (49-110) | 0.264 |
| p | 0.017 | 0.003 | 0.004 | 0.833 | 0.846 | 0.323 | ||
| TGF-β1 (pg/mL) | ||||||||
| Basal | 286 (244-313) | |||||||
| Day 1 | 774 (701-872) | 862 (601-965) | 972 (764-1354) | 0.217 | 444 (31-523) | 382 (346-512) | 875 (826-927) | 0.009 |
| Day 3 | 1164 (506-1443) | 1315 (1234-1406)∗ | 1726 (1624-2028)∗§ | 0.031 | 736 (526-818) | 580 (493-1021) | 853 (674-902) | 0.837 |
| Day 7 | 989 (448-1585) | 2128 (2104-2196)∗#§ | 2439 (2064-2530)∗#§ | 0.020 | 786 (633-959) | 710 (636-841) | 851 (533-1005) | 0.912 |
| p | 0.794 | <0.001 | <0.001 | 0.067 | 0.027 | 0.066 | ||
In relation to VEGF (Table 1), the pleural values exceeded the serum value of 31 (31-34) during the entire study period. This cytokine was differentially expressed compared to IL-8, with the maximum expression reached on day seven (2%, p = 0.017; 4%, p = 0.003 and 10%, p = 0.004).
The pleural levels of TGF-β1 were significantly greater than those obtained in the serum at 4% or 10% concentrations on the third (4%, p = 0.022 and 10%, p<0.001) and seventh days (4%, p = 0.041 and 10%, p<0.001). The temporal analysis of the pleural fluid revealed stable values for the 2% concentration. At higher concentrations, we observed a progressive increase of the fluid levels (p<0.001). The serum values were also significantly greater than the baseline level of 286 (244-313) in all of the evaluated periods (Table 1.
Analysis of thyroid hormones and renal function markers (Figure 2) showed no significant differences among the groups during the study period. Furthermore, the results did not differ from the baseline values.
 of renal function markers and thyroid hormones in the blood during the study period (1-28 days). (a) The blood levels of urea, (b) creatinine, (c) Triiodothyronine and (d) free thyroxine.")
Analysis of macroscopic pleural adhesions demonstrated a progressive increase over time and was more pronounced in the animals injected with 4% or 10% iodine. Analogous behavior was observed for visceral pleural thickening, which was more pronounced at increased concentrations of the sclerosing agent (Figure 3). Finally, the morphological analysis of the retina showed no changes related to time or iodine concentration. We did not observe any edemas or alterations in retinal pigment epithelium (atrophy or hypertrophy) or in photoreceptors. Cells from the intermediate and internal retina were also within the normal limits. No macro or microscopic changes were observed in the left hemithorax (not injected, used as control).
 of the evaluation of macroscopic pleural adhesions and microscopic thickening after intrapleural iodopovidone during the study period (1 to –28 days). (a) Macroscopic adhesions evaluated using a 0-4 score. (b) Microscopic pleural thickness using a 0-4 score.")
The median and interquartile range (25%-75%) of the evaluation of macroscopic pleural adhesions and microscopic thickening after intrapleural iodopovidone during the study period (1 to –28 days). (a) Macroscopic adhesions evaluated using a 0-4 score. (b) Microscopic pleural thickness using a 0-4 score.
This study shows that the intrapleural injection of iodopovidone causes an early pleural inflammatory response with low systemic repercussion and no detectable side effects in our animal model. The higher iodine concentrations (4% and 10%) resulted in an early increase in pleural fluid production and more pronounced pleural adhesions and thickening. Finally, iodopovidone, in the studied concentrations, did not induce thyroid or renal function changes or anatomical changes in the retinal structure.
The mechanisms involved in pleural symphysis are not completely known. Introducing a sclerosing agent into the pleural space is known to damage the mesothelial cell monolayer and trigger an inflammatory response that is characterized by a neutrophilic exudate (13–15). The subsequent events culminate with fibrotic adhesion development between the pleural surfaces and the consequent obliteration of the cavity. Among the factors involved in the inflammatory response, we highlight mesothelial cell injury, the collagen-secreting capacity of these cells and the fibroblasts, the equilibrium between metalloproteinases and plasminogen activators and the relationship between cytokines and fibrinolysis (16).
Iodopovidone should be considered in addition to other sclerosing agents used in clinical practice, as it is universally found, easily manipulated and low cost (approximately $8 USD per 500 mL). Iodopovidone was introduced in the 1990s (17) and has an approximately 90% effectiveness (7–9). Similar to other agents, the produced pleural symphysis is most likely related to the injury of the mesothelial cells, which are initially exteriorized by a progressive production of pleural fluid with inflammatory characteristics.
During the first 24 hours after the iodine injection, an expressive elevation of intrapleural lactic dehydrogenase, which has a tendency to decrease over time, was identified; the systemic repercussions were minimal. Guo et al. (18) reported similar results after intrapleurally injecting iodine at 2% or 4% concentrations, and Marchi et al. (19), who induced experimental pleurodesis with talc or silver nitrate, also obtained an early decrease in serum lactic dehydrogenase, which reflected a local inflammatory response.
IL-8, an important mediator of the inflammatory process, shows similar behavior to lactic dehydrogenase. Regardless of the iodine concentration, pleural fluid IL-8 levels increased early during the first 24 hours and progressively decreased over time. In the serum, the IL-8 levels were stable but greater than the basal values. VEGF carries out multiple functions. In addition to participating in the initial inflammatory process in which VEGF stimulates the activation of mediators and facilitates the migration of inflammatory cells, it has an important role in vascular permeability, and, therefore, in pleural effusion production (12). In this study, we observed a progressive and accentuated elevation in pleural fluid, with minimal serum increase. Note the correspondence between VEGF and the intrapleural accumulation of fluid, which reinforces the role of VEGF in pleural effusion formation.
Finally, TGF-β is also recognized for its multiple roles, mainly in collagen deposition and fibrosis formation (16). Although TGF-β expression largely paralleled VEGF expression in the pleural cavity, the TGF-β serum levels throughout the study period were greater compared to the values obtained before treatment. This behavior allowed us to consider its participation in pleurodesis formation.
The result of this complex inflammatory process is pleural symphysis. We have demonstrated that the intrapleural injection of iodopovidone promotes, from the first 24 hours, a framework of adhesions with temporal progression and complete disappearance of the pleural cavity after 28 days.
In terms of the eventual side effects caused by iodopovidone, we did not observe any severe damage. Corroborating our findings, in a meta-analysis of observational studies, Agarwal et al. (5) demonstrated the efficacy and safety of iodopovidone pleurodesis reporting an absence of deaths. The most significant complication reported was varying degrees of chest pain. Systemic hypotension was reported in one study. Although this review supports the safety and efficacy of iodopovidone as an agent for chemical pleurodesis, no comments regarding dosage or concentration have been mentioned. However, in 2000, Singalavanija et al. (20) described five patients who presented higher serum creatinine levels and retinal damage with visual impairment after mistakenly ingesting potassium iodine orally at high concentrations. The authors concluded that potassium iodine is a chemical substance that in high doses can induce toxic effects on the retina, thereby damaging the retinal epithelium and photoreceptors cells. Recently, Wagenfeld et al. (6) described visual loss resulting from the breakdown of the diffusion barrier of the retinal pigment epithelium in three patients who received a 10% iodopovidone solution during thoracoscopic surgery. Note that the dose and the volume of iodopovidone used in this procedure were much greater than that normally recommended. Although our study has been conducted on a small number of animals, we did not find changes or damage in the retinal pigment epithelium of any rabbit, even at the highest concentration (10%) of iodopovidone.
Another side effect that should be considered is a possible thyroid blockage. Kovacikova et al. (21) reported that iodopovidone, either in topical use or as contrast in image procedures, may cause transient thyroid dysfunction, mainly in children. High concentrations of exogenous iodine are capable of diminishing thyroid hormone synthesis or induce thyrotoxicosis in susceptible individuals (22). However, Yeginsu et al. (23) reported that the intrapleural administration of 100 mL of 2% iodopovidone did not affect thyroid hormone levels in humans. Although our study was conducted in an animal model, we did not find abnormal results in thyroid hormone levels, even in high concentrations.
In conclusion, our findings suggest that iodopovidone is an effective and safe sclerosing agent. Further studies in humans should be conducted to determine the ideal dose and concentration.
AUTHOR CONTRIBUTIONSTeixeira LR conceived and designed the study, participated in all of the experimental stages, composition of the manuscript. Vargas SF prepared the figures, statistical analysis and final composition of the manuscript. Puka J, Pitta FG participated in all of the experimental stages. D'Amico FM was responsible for the retinal tissue analysis. Acencio MM was responsible for the laboratorial support and orientation of the statistical study. Antonangelo L was responsible for the laboratorial support, interpretation of the results. Terra RM, Macchi E designed the study and were responsible for the data analysis.
We thank biologists Carlos SR Silva and Vanessa Alvarenga and physicians Vivian Ribeiro, Flavio Zelada, Natalia Novaes and Renato AEK Matsumoto for their assistance with animal care and sample preparation and storage. Financial support: Research Support Foundation of the State of São Paulo (FAPESP) and the National Research Council (CNPq), Brazil.
No potential conflict of interest was reported.