






To explore the use of β-lactoglobulin polymerized using microbial transglutaminase and heating to identify whether protein polymerization could reduce in vivo allergenicity and maintain in vitro and ex vivo immunoreactivity for use in tolerance-induction protocols.
METHODS:Based on previous protocols applied in mice and children, we performed in vivo challenges (using a skin prick test) with native and polymerized β-lactoglobulin in adult patients with an IgE-mediated allergy to β-lactoglobulin. In vitro humoral immunoreactivity was analyzed using immunoblotting. Cell-mediated immunoreactivity was analyzed using ex vivo challenges with native and polymerized β-lactoglobulin and monitored by leukocyte adherence inhibition tests.
RESULTS:The skin tests demonstrated that there was a significant reduction in immediate cutaneous reactivity after polymerization. Polymerization did not decrease the immunoblotting detection of s-IgE specific to β-lactoglobulin. Cell-mediated immunoreactivity, as assessed by ex vivo challenges and leukocyte adherence inhibition tests, did not exhibit significant differences between leukocytes challenged with native versus polymerized β-lactoglobulin.
CONCLUSIONS:The polymerization of β-lactoglobulin decreased in vivo allergenicity and did not decrease in vitro humoral or ex vivo cell-mediated immunoreactivity. Therefore, we conclude that inducing polymerization using transglutaminase represents a promising technique to produce suitable molecules for the purpose of designing oral/sublingual tolerance induction protocols for the treatment of allergies.
The primary strategy currently used to manage cow’s milk allergies is to diagnose the offending protein (whey proteins, cheese caseins or both) and prescribe its dietary elimination (1-3). Nevertheless, avoidance strategies may also contribute to a loss of tolerance (4). Oral tolerance induction protocols using whole cow’s milk have been described (5,6). However, the use of a natural extract of an allergen may elicit allergic reactions, thereby limiting the progress of desensitization. Modified allergens (allergoids) have been used in desensitization protocols to minimize the allergic reactions produced by the native allergen (7). Less allergenic immuno-equivalent proteins may be obtained, for example, using recombinant DNA technology (8), but this method is laborious and expensive. More accessible approaches, including extensive baking, have been used for milk tolerance induction based on the assumption that the destruction of conformational epitopes yields a safer protein for oral administration (9). However, this type of physical denaturation may also induce difficult-to-control chemical modifications in the allergen, making the characterization of the resultant allergen almost impossible while simultaneously destroying the linear epitopes necessary to prime tolerance induction (10). The rationale for performing safe and efficient oral tolerance induction protocols ideally includes the use of a protein that is immunogenic (harboring all relevant T cell epitopes) but less allergenic (eliciting weaker clinical reactions) (11). The allergenicity of a modified antigen may be evaluated using in vivo challenge tests (cutaneous or oral) and/or ex vivo challenge tests, such as the basophil degranulation assay. The extent of the allergen-elicited cell-mediated immunoreactivity responsible for priming the subsequent immune response and/or tolerance may be analyzed prior to treatment using T cell proliferation assays (12) or after treatment by detecting markers of immune tolerance from cultured PBMCs or searching for inducible Tregs expressing IL-10 and TGF-β (13). As a model for this study, we employed enzymatic polymerization, a process that is widely used to produce industrial foods. The use of biotechnology to modify the physical properties of dairy products is currently practiced and can alter the allergenicity of native proteins, thereby resulting in the creation of new and troublesome allergens or less allergenic (hypoallergenic) products (14). Among bovine whey proteins, β-lactoglobulin (β-Lg) is a prevalent allergen, as demonstrated by oral challenges, skin scratch tests and skin prick tests (SPTs) (15). Because polymerization enzymes, such as microbial transglutaminase (TG), are applied to decrease syneresis, polymerized β-Lg is found in industrialized dairy products, such as curd cheese and yogurt. TG catalyzes acyl-transfer reactions between the gamma-carboxyamide groups of glutamine residues and the epsilon-amino group of lysine, thereby causing the inter- or intramolecular crosslinking of proteins (16). Previous studies in mice have demonstrated that the polymerization of β-Lg by TG in the presence of cysteine may reduce β-Lg antigenicity before and after digestion (17,18). SPTs have also indicated that polymerized β-Lg may be less allergenic than native β-Lg in children with an IgE-mediated cow’s milk allergy (19). However, ex vivo cell-mediated immunoreactivity to polymerized β-Lg has not yet been studied in humans. Seeking an immunogenic but less allergenic molecule for use in desensitization protocols and in accordance with the directive of the FAO/WHO decision tree for analyzing the allergenicity of foods derived from biotechnological processes (20), we examined the allergenicity and immunoreactivity of native and polymerized β-Lg in adults with and without a confirmed diagnosis of an IgE-mediated allergy to β-Lg. The FAO/WHO directive recommends performing the diagnosis of a specific IgE-mediated allergy following SPTs using the native and bioprocessed proteins in people with proven allergies to the native protein. Because the detection of a specific IgE using SPT or ImmunoCAP assays is associated with certain pitfalls (21), we also performed confirmatory SDS-PAGE immunoblots to improve analytical sensitivity and detect false-negative or false-positive results (22). This analysis was conducted in accordance with the GRADE approach (grades of recommendation, assessment development and evaluation) for grading the quality of evidence of diagnostic tests (23). Therefore, as a secondary endpoint, we assessed the sensitivity of the ImmunoCAP and SPT assays for detecting specific IgE antibodies against β-Lg in patients who exhibited specific IgE sensitization, as confirmed by SDS-PAGE immunoblotting. Ex vivo cell-mediated immunoreactivity for β-Lg has previously been evaluated with the leukocyte migration inhibition test (24). We used an equivalent but technically simpler assay to assess β-Lg cell-mediated immunoreactivity: the leukocyte adherence inhibition test (LAIT) (25-28).
MATERIALS AND METHODSEthics StatementsThis study was submitted to and approved by the Institutional Research Ethics Board and was registered in the Brazilian National Ethics Research System (SISNEP 409/2008). In accordance with the Helsinki Declaration, signed consent forms were obtained from all subjects.
Study design and subjectsThis descriptive case-control study was designed to examine the following parameters: A) the in vivo allergenicity of native β-Lg and transglutaminase/cysteine-polymerized β-Lg (TgPolβ-Lg) in symptomatic adult patients exhibiting specific IgE antibodies against β-Lg (βs-IgE); B) the in vitro humoral immunoreactivity of native β-Lg and heated polymerized β-Lg (HtPolβ-Lg) in symptomatic adult patients exhibiting βs-IgE, as diagnosed by SDS-PAGE immunoblotting, SPT and ImmunoCAP assays; and C) the ex vivo cell-mediated immunoreactivity of β-Lg and TgPolβ-Lg, independent of patient βs-IgE status. The participants were divided into three groups according to their clinical presentation and analytical results. The first group (group A) included 45 patients (17 males; mean age: 46.2 years, SD: 12.2 years) with convincing clinical histories of reproducible adverse reactions to bovine milk. All subjects exhibited βs-IgE detectable by SDS-PAGE immunoblotting. The second group (group B) was used as a control for the immunoblotting analysis performed in the first group and included 20 individuals selected based on an evident tolerance to cow’s milk, an absence of βs-IgE by ImmunoCAP assay and SPT non-reactivity to β-Lg or TgPolβ-Lg (6 males; mean age: 21.9 years, SD: 17.6 years). The third group (group C) included 49 subjects with atopic respiratory and/or dermatological diseases (19 males; mean age: 28.7 years, SD: 20.6 years) regardless of βs-IgE status. This group was used to compare the ex vivo cell-mediated immunoreactivity between β-Lg and TgPolβ-Lg by comparing the mean ex vivo antigenic challenge results determined using the leukocyte adherence inhibition test (LAIT).
Allergens, antibodies and reagentsChromatographically purified β-Lg (>95% pure) was provided by Davisco Foods, Inc. (Le Sueur, USA). A goat polyclonal secondary antibody to human IgE–epsilon chain (ab9159) and peroxidase (HRP)-conjugated rabbit polyclonal secondary antibody to goat IgG (ab6741) were acquired from Abcam, Inc. (Cambridge, MA, USA). A commercial preparation of transglutaminase from Streptoverticillium mobaraense (Activa®) containing 99% maltodextrin and 1% transglutaminase (TG) with a declared activity of 100 U/g was donated by Ajinomoto Co. (Tokyo, Japan). Cysteine, sodium dodecyl sulfate (SDS) and 3,3’-diaminobenzidine tetrahydrochloride (DAB) were obtained from Sigma-Aldrich Chemie GmbH (Steinheim, Germany). Tween-20 and β-mercaptoethanol were obtained from Merck KgaA (Darmstadt, Germany).
β-lactoglobulin polymerizationFor immunoblotting, β-Lg was polymerized by heating (see Reducing SDS-PAGE section) to stimulate the formation of tetramers (HtPolβ-Lg) because the high-molecular weight polymers generated by transglutaminase activity did not penetrate the SDS-PAGE gel.
For skin tests, cysteine/transglutaminase β-Lg polymerization was performed as described previously (18).
Preparation of solutions for skin testsTo standardize skin tests with respect to the conditions of previous studies (2), β-Lg and TgPolβ-Lg skin solutions were diluted to a concentration of 10,000 PNU/mL. Nitrogen levels were quantified by Kjeldahl’s method (AOAC 991.22), which indicated that each gram of lyophilized β-Lg contained 14.4 g of nitrogen and each gram of lyophilized TgPolβ-Lg contained 11.1 g of nitrogen. For the skin tests, β-Lg, TgPolβ-Lg and the control substances were solubilized at a pH of 7.0 and diluted to their final concentrations using a 20% w/v glycerol/saline solution (20% GS). The β-Lg solution was diluted to a concentration of 0.7 mg/mL using 20% GS, and the TgPolβ-Lg solution was diluted to a final concentration of 0.9 mg/mL using 20% GS. The TG and cysteine skin reactivities were tested simultaneously. The TG solution for the skin tests was diluted to a concentration of 0.2 mg/mL using 20% GS, and the cysteine solution for the skin tests was diluted to 0.3 mg/mL using 20% GS. Histamine (1 mg/mL in 20% GS) was used as a positive control, and the negative-control solution was 20% GS.
Skin test methodologySkin tests were performed on the volar aspect of the patient’s forearms after withholding antihistamines for at least 10 days. Skin prick tests (SPTs) were performed using a disposable sterile acrylic needle consisting of a 1-mm lancet attached to a blunt base (Punctor®, Alko do Brasil Ltda, Rio de Janeiro, Brazil). The needle was introduced at a 90° angle to the skin through an allergen solution droplet, removed after 1 second and discarded. The final reading was performed 15 minutes later, and the wheal’s greatest diameter and its perpendicular length at that point were measured to estimate the mean wheal diameter (MWD) (29). Because there was no reaction to the negative control, a MWD ≥3 mm was considered significant for sensitization.
The samples were analyzed by SDS-PAGE under reducing conditions using a Mini Protean Tetra Cell apparatus (Bio-Rad, CA, USA) and 5%T/20%C gel gradients (30). Purified β-Lg samples (5 mg/mL) were prepared in a buffer containing 2% SDS and 5% β-mercaptoethanol and then heated for 10 min at 96 °C. An aliquot of 5 μL, which was equivalent to 25 μg of protein, was applied to each lane. A 10-170 kDa molecular mass pre-stained protein ladder (PageRuler®, Fermentas, Hanover, MD, USA) was used to identify approximate molecular weights.
Following electrophoresis, the proteins were electroblotted onto 0.45-μm pore-size nitrocellulose membranes (Bio-Rad) using a Mini Trans-Blot Cell apparatus (Bio-Rad). Membranes were incubated overnight at 4°C with gentle agitation in 3 mL phosphate-buffered saline (PBS), pH 7.0, containing 3 μL of the individual patient’s serum, followed by three washes in PBST (PBS containing 0.05% Tween-20). The membranes were incubated under gentle agitation for 2 hours in polyclonal goat IgG anti-human IgE (15 μg in 3 mL PBS), washed three times with PBST and incubated with horseradish peroxidase (HRP)-conjugated rabbit anti-goat IgG (30 μg in 3 mL PBS) for 2 hours. After three washes with PBST, HRP activity was stimulated by incubating the membranes in 10 mL PBS containing 0.05% DAB followed by the addition of 50 μL developing solution (CoCl2.6H2O plus NiSO4) and 20 μL of hydrogen peroxide (H2O2) (31). When impregnation and color development were complete, the membranes were washed in distilled water and subsequently dried. Images of the membranes were digitalized, and the relative densitometry of the bands was analyzed using ImageJ software (Windows version 1.44 of NIH ImageJ, http://rsb.info.nih.gov/ij/index.html) by measuring the average optical density (OD). Adjusted optical density (AOD) was calculated following background correction by subtracting the average OD from a user-defined area within the image from the average OD of a similar area defined around the measured bands (32).
Polymerization of β-Lg via heating created 72-kDa β-Lg tetramers (HtPolβ-Lg) exhibiting an electrophoretic mobility similar to BSA (66.7 kDa) (33). Although the β-Lg samples were purified, we performed parallel in vitro serum competition assays with BSA (1 mg/mL) to rule out the possibility of BSA interference in the assay.
The concentrations of serum IgE antibodies specific for β-Lg were measured by ImmunoCAP assays (Pharmacia, Uppsala, Sweden), and the results were expressed in kU/L. A concentration greater than 0.35 kU/L was considered significant for sensitization (34).
Leukocyte adherence inhibition testLeukocytes from heparin-treated blood samples drawn by venipuncture from the forearm were separated from fresh blood by sedimentation at 37°C for one hour. Aliquots of 100 μL of plasma were incubated with 10 μL of each antigen extract (the same solutions used in the skin tests: β-Lg at 0.7 mg/mL in 20% GS and TgPolβ-Lg at 0.9 mg/mL in 20% GS) for 30 minutes under gentle agitation (200 rpm) at 37°C. Plasma without antigens was used as a control. After incubation, the plasma was placed into a standard Neubauer hemocytometer counting chamber with a plain, non-metallic glass surface and left to stand for 2 hours at 37°C in a humidified atmosphere to allow leukocytes to adhere to the glass. The leukocytes were then counted, the coverslip was gently removed, and the chamber was washed by immersion in a beaker with PBS at 37°C. A drop of PBS was subsequently added to the hemocytometer chamber, and a clean coverslip was placed over it. The remaining cells were counted in the same squares examined previously. The percentage of cell adherence (cell number after washing/cell number before washing) was calculated, and leukocyte adherence inhibition (LAI) was estimated based on the ratio between the percentage of adherent cells from the challenged groups versus the control groups: LAI = [1-(% adherent cells of challenged sample/% adherent cells of control sample)]x100.
Statistical analysesStatistical analyses and graphs were produced using GraphPad Prism software (version 5.0; GraphPad Software, Inc., San Diego, CA, USA). The data are reported as arithmetic means with 95% confidence intervals (CI) and standard deviations (SD). Differences in the means of matched samples were assessed by paired t-tests. Contingency tables analyzed by chi-square and Fisher’s exact tests were used to compare the categorical diagnostic performance between assays. Spearman correlations were used to analyze the LAIT results between β-Lg and TgPolβ-Lg. For all analyses, a p-value of less than 0.05 was considered significant.
RESULTSGroup A: ImmunoCAP s-IgEThe mean level of IgE antibodies specific for β-Lg was 1.5 kU L-1 (CI: 0.5 to 2.4; SD: 3.2 kU/L). Specific IgE antibodies were detected using ImmunoCAP assays in 19 patients (sensitivity = 42.2 %). The test results are presented in Table 1.
Test results from group A patients.
| Patient | Ageyears | sIgEβLgkU/L | SPTPCMWD | SPTβLgMWD | SPTTgβLgMWD | AOD72 kDa | AOD36 kDa | AOD18 kDa |
|---|---|---|---|---|---|---|---|---|
| 1 | 57 | 0.6 | 10 | 5 | 0 | 37.6 | 16.4 | 0.4 |
| 2 | 45 | 0.6 | 7 | 4 | 4 | 10.0 | 0.0 | 0.0 |
| 3 | 51 | 0.0 | 8 | 5 | 0 | 20.4 | 0.0 | 0.0 |
| 4 | 48 | 0.5 | 8 | 4 | 4 | 10.7 | 9.6 | 2.1 |
| 5 | 32 | 0.0 | 7 | 0 | 0 | 16.5 | 13.5 | 1.8 |
| 6 | 34 | 0.0 | 6 | 3 | 3 | 21.0 | 8.0 | 6.1 |
| 7 | 47 | 12.6 | 9 | 0 | 0 | 46.6 | 7.0 | 0.0 |
| 8 | 26 | 0.0 | 11 | 0 | 3 | 18.8 | 9.9 | 0.0 |
| 9 | 18 | 2.1 | 6 | 0 | 0 | 48.8 | 10.2 | 0.0 |
| 10 | 53 | 0.0 | 5 | 0 | 4 | 24.1 | 12.1 | 0.0 |
| 11 | 39 | 0.0 | 8 | 0 | 0 | 10.4 | 13.4 | 8.1 |
| 12 | 46 | 1.2 | 5 | 0 | 0 | 13.2 | 5.9 | 0.0 |
| 13 | 55 | 5.2 | 5 | 0 | 0 | 23.2 | 0.0 | 0.0 |
| 14 | 42 | 0.0 | 9 | 0 | 3 | 24.1 | 7.8 | 3.4 |
| 15 | 65 | 0.0 | 5 | 0 | 0 | 21.1 | 6.8 | 0.0 |
| 16 | 53 | 0.0 | 6 | 5 | 0 | 23.1 | 12.5 | 0.0 |
| 17 | 48 | 15.4 | 5 | 3 | 0 | 35.9 | 0.0 | 0.0 |
| 18 | 49 | 4.0 | 6 | 0 | 0 | 7.6 | 0.0 | 0.0 |
| 19 | 58 | 0.0 | 6 | 0 | 0 | 24.8 | 0.0 | 0.0 |
| 20 | 59 | 0.4 | 6 | 4 | 5 | 15.6 | 0.0 | 0.0 |
| 21 | 43 | 0.5 | 6 | 4 | 4 | 19.2 | 0.0 | 0.0 |
| 22 | 28 | 0.0 | 9 | 6 | 0 | 19.4 | 0.0 | 0.0 |
| 23 | 39 | 4.0 | 6 | 3 | 3 | 14.6 | 0.0 | 0.0 |
| 24 | 55 | 0.0 | 7 | 0 | 0 | 25.9 | 0.0 | 0.0 |
| 25 | 51 | 0.0 | 7 | 3 | 0 | 16.4 | 0.0 | 0.0 |
| 26 | 42 | 9.2 | 9 | 9 | 6 | 21.0 | 0.0 | 0.0 |
| 27 | 52 | 1.8 | 8 | 5 | 5 | 24.3 | 12.2 | 12.5 |
| 28 | 36 | 0.0 | 8 | 3 | 3 | 10.5 | 9.2 | 0.0 |
| 29 | 22 | 0.0 | 7 | 4 | 0 | 7.1 | 0.0 | 0.0 |
| 30 | 41 | 1.2 | 7 | 6 | 3 | 12.0 | 0.0 | 0.0 |
| 31 | 56 | 0.0 | 7 | 6 | 4 | 12.2 | 12.2 | 12.5 |
| 32 | 58 | 0.0 | 4 | 0 | 4 | 17.0 | 0.0 | 0.0 |
| 33 | 56 | 0.0 | 8 | 4 | 0 | 19.9 | 0.0 | 0.0 |
| 34 | 29 | 0.0 | 6 | 4 | 4 | 10.9 | 0.0 | 0.0 |
| 35 | 44 | 0.4 | 7 | 0 | 0 | 9.8 | 0.0 | 0.0 |
| 36 | 48 | 0.0 | 6 | 5 | 3 | 20.4 | 0.0 | 0.0 |
| 37 | 70 | 0.0 | 7 | 4 | 0 | 8.2 | 0.0 | 0.0 |
| 38 | 64 | 4.6 | 5 | 0 | 0 | 10.0 | 0.0 | 0.0 |
| 39 | 40 | 1.2 | 0 | 0 | 0 | 11.7 | 5.8 | 4.4 |
| 40 | 61 | 0.0 | 7 | 4 | 0 | 14.6 | 0.0 | 0.0 |
| 41 | 50 | 3.8 | 10 | 6 | 4 | 5.5 | 5.4 | 0.0 |
| 42 | 63 | 0.0 | 8 | 6 | 0 | 5.0 | 0.0 | 7.3 |
| 43 | 23 | 0.0 | 6 | 5 | 5 | 14.1 | 0.0 | 0.0 |
| 44 | 46 | 0.0 | 8 | 0 | 0 | 6.0 | 3.5 | 13.9 |
| 45 | 38 | 0.0 | 7 | 0 | 0 | 7.2 | 0.0 | 0.0 |
s-IgE βLg: specific IgE antibodies against beta-lactoglobulin measured by ImmunoCAP (kU/L); SPT: skin prick test; PC: positive control (histamine); MWD: mean wheal diameter (mm); βLg: native beta-lactoglobulin; TgβLg: beta-lactoglobulin polymerized by transglutaminase and cysteine; AOD: adjusted optical density.
The test results are presented in Table 1. The mean MWD for histamine (positive control) obtained by SPT was 6.8 mm (CI: 6.2 to 7.3; SD: 1.8 mm). β-Lg was reactive in SPTs in 26 patients (sensitivity = 57.7%). The mean MWD for β-Lg obtained by SPT was 2.6 mm (CI: 1.9 to 3.4; SD: 2.5 mm). TgPolβ-Lg was reactive in SPTs in 19 patients (sensitivity = 42.2%). The mean MWD for TgPolβ-Lg obtained by SPT was 1.6 mm (CI: 1.0 to 2.2; SD: 2.0 mm). The mean difference between the paired MWD means for β-Lg and TgPolβ-Lg was 1.0 (p = 0.0075). There was no skin reactivity observed against TG, cysteine or the negative control solution in any patient (results not shown).
Comparison of categorical performance between assaysAnalysis of the contingency table between the ImmunoCAP (19 positives) and SPT assays using β-Lg (26 positives) for the 45 patients with positive immunoblots via chi-squared (α<0.05 and p = 0.39) and Fisher exact tests (α<0.05 and p = 0.46) failed to reveal significant differences.
Combined categorical analytical sensitivityCombined SPTs with β-Lg and TgPolβ-Lg exhibited cutaneous reactivity in 30 patients (sensitivity = 66.6%). The combination of ImmunoCAP and SPT assays for β-Lg revealed reactivity in 34 patients (sensitivity = 75.5%). A combination of the three tests detected cutaneous reactivity in 38 patients (sensitivity = 84.4%).
Immunoblot assaysFigure 1 shows the purified beta-lactoglobulin electroblotted 0.45-μm pore-size nitrocellulose membranes after incubation with patient’s serum, primary antibody (goat IgG anti-human IgE), secondary antibody (HRP-conjugated rabbit anti-goat IgG) and DAB revelation from subjects of group A. Our immunoblot analysis revealed 18-kDa bands (β-Lg monomers) in 11 patients (24.4%) with a mean AOD of 1.6 (CI: 0.5 to 2.7). The immunoblots also revealed 36-kDa bands (β-Lg dimers) in 19 patients (42.2%) with a mean AOD of 4.0 (CI: 2.4 to 5.6). Additionally, there were bands at 72-kDa (β-Lg tetramers) in 45 patients (100%) with a mean AOD of 17.7 (CI: 14.73 to 20.6). The mean of the difference between the AODs of the 18-kDa bands and 36-kDa bands was 2.4 (p = 0.00027, CI: 0.8 to 3.9). The mean of the differences between the AODs of the 18-kDa bands and 72-kDa bands was 16.0 (p<0.0001, CI: 12.7 to 19.4). The mean of the difference between the AODs of the 36-kDa bands and 72-kDa bands was 13.6 (p<0.0001, CI: 10.7 to 16.5). The blot membranes incubated with the serum subjected to BSA competition did not exhibit any difference compared with those incubated with the corresponding serum not subjected to BSA competition (see Figure 2). Of the 20 patients from group B, representing milk-tolerant controls with non-reactive SPTs for β-Lg and TgPolβ-Lg and absent β s-IgE based on ImmunoCAP, only one patient (5%) exhibited a 72-kDa band with an AOD = 10.5 (see Figure 3).
, secondary antibody (HRP-conjugated rabbit anti-goat IgG) and DAB revelation, demonstrating bands of s-IgE against β-lactoglobulin at 72 kDa (β-Lg tetramers), 36 kDa (β-Lg dimers) and 18 kDa (β-Lg monomers) from patients in group A. Lane P = pre-stained 10-170 kDa molecular mass protein ladder (PageRuler®, Fermentas).")
Purified beta-lactoglobulin electroblotted on 0.45-μm pore-size nitrocellulose membranes after incubation with patient’s serum, primary antibody (goat IgG anti-human IgE), secondary antibody (HRP-conjugated rabbit anti-goat IgG) and DAB revelation, demonstrating bands of s-IgE against β-lactoglobulin at 72 kDa (β-Lg tetramers), 36 kDa (β-Lg dimers) and 18 kDa (β-Lg monomers) from patients in group A. Lane P = pre-stained 10-170 kDa molecular mass protein ladder (PageRuler®, Fermentas).
, secondary antibody (HRP-conjugated rabbit anti-goat IgG) and DAB revelation. Immunoblot membranes exhibited bands of s-IgE against β-lactoglobulin (β-Lg). Lane 1: Molecular weight ladder (10 to 170 kDa); Lane 2: distinct band at 72 kDa in a patient from group A; and Lane 3: distinct band at 72 kDa from the same patient after ex vivo serum competition with BSA.")
Purified beta-lactoglobulin electroblotted on 0.45-μm pore-size nitrocellulose membranes after incubation with patient’s serum, primary antibody (goat IgG anti-human IgE), secondary antibody (HRP-conjugated rabbit anti-goat IgG) and DAB revelation. Immunoblot membranes exhibited bands of s-IgE against β-lactoglobulin (β-Lg). Lane 1: Molecular weight ladder (10 to 170 kDa); Lane 2: distinct band at 72 kDa in a patient from group A; and Lane 3: distinct band at 72 kDa from the same patient after ex vivo serum competition with BSA.
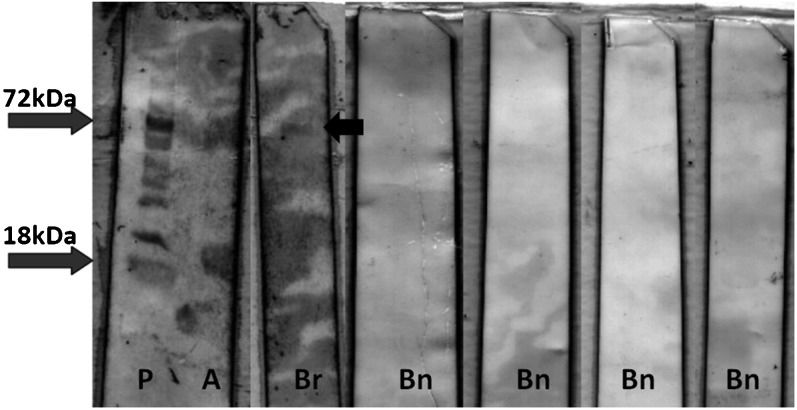
, secondary antibody (HRP-conjugated rabbit anti-goat IgG) and DAB revelation. Immunoblot membranes exhibiting bands of s-IgE against β-lactoglobulin from four non-reactive patients in group B (Bn), from the single reactive patient from group B (Br), and from one reactive patient from group A (A) used as a control for the blotting technique. P = pre-stained 10-170 kDa molecular mass protein ladder (PageRuler®, Fermentas).")
Purified beta-lactoglobulin electroblotted on 0.45-μm pore-size nitrocellulose membranes after incubation with patient’s serum, primary antibody (goat IgG anti-human IgE), secondary antibody (HRP-conjugated rabbit anti-goat IgG) and DAB revelation. Immunoblot membranes exhibiting bands of s-IgE against β-lactoglobulin from four non-reactive patients in group B (Bn), from the single reactive patient from group B (Br), and from one reactive patient from group A (A) used as a control for the blotting technique. P = pre-stained 10-170 kDa molecular mass protein ladder (PageRuler®, Fermentas).
In group C, the mean leukocyte adherence inhibition (LAI) produced by ex vivo challenge with β-Lg was 39.6% (SD: 36.8%; CI: 29.0% to 50.2%), whereas the LAI produced by ex vivo challenge with TgPolβ-Lg was 47.7 (SD: 38.4; CI: 36.6 to 58.7). The difference of the means based on a paired t-test was not significant (p = 0.07). The correlation between challenges was significant (Spearman r = 0.65 CI = 0.44 to 0.79 p<0.0001). Results are presented in Table 1. Figure 4 depicts the microscope aspect before and after the PBS wash of two patients with LAI = 54% and 100%, respectively, and a control (without antigen challenge) with 100% leukocyte adherence.
 = 100%. Patient B exhibited leukocyte adherence inhibition (LAI) = 54%. C = Control (without antigen) with leukocyte adherence (LA) = 100%.")
Leukocyte adherence inhibition tests from two patients in group C before and after washing. Patient A exhibited leukocyte adherence inhibition (LAI) = 100%. Patient B exhibited leukocyte adherence inhibition (LAI) = 54%. C = Control (without antigen) with leukocyte adherence (LA) = 100%.
Among the immunoreactive proteins found in whey in bovine milk, β-Lg is prominent because of its relatively high concentration (3 to 4 g/L on average) and low digestibility (35). The high incidence of sensitization to this protein (38) is understandable in light of the fact that β-Lg is not a component of human breast milk (36) and is usually absorbed in an unchanged form (37). β-Lg proteins naturally occur as dimers at a pH>3 (39). Heating β-Lg to 70°C induces further polymerization (40). Purified heated β-Lg preparations generally contain monomers, dimers and tetramers when examined using reducing SDS-PAGE (33). Protein polymerization using TG in industrialized dairy products is a commonly employed technique to decrease whey syneresis and improve the gel strength/viscosity of set-type yogurt and curd cheese (41). Treatment with TG has been shown to decrease wheat allergenicity (42). Given the evidence that polymerization reduces the antigenicity of β-Lg (18) and ovalbumin in mice (43), the application of polymerization techniques could potentially reduce the allergenicity of industrialized foods for humans and might be useful in producing “allergoids” for desensitization immunotherapy (7). A probable explanation for this reduced allergenicity is that polymerization masks IgE antibody binding sites due to crosslinking of the protein. Polymerization may also create new epitopes, which may result in the development of hypersensitivities that are not related to the native protein.
The skin test results presented in this study indicated a significant reduction in the allergenicity of TgPolβ-Lg compared with native β-Lg. Polymerization changes the spatial distribution of allergenic epitopes, which may explain the decreased cutaneous reactivity of these epitopes. However, although the average skin reactivity to TgPolβ-Lg was lower than the average reactivity to β-Lg, four patients exhibited no skin reaction to β-Lg but did exhibit significant skin reactivity to TgPolβ-Lg. This finding indicates that transglutaminase polymerization may be deleterious for certain patients. Polymerization also increases the analytical detection of βs-IgE antibodies by SDS-PAGE immunoblotting. Before subjecting β-Lg samples to SDS-PAGE, the samples were heated for 10 min at 96°C. Heating stimulates the polymerization of β-Lg and results in the detection of 72-kDa bands (tetramers) (33). Because β-Lg monomers are small proteins, they can be lost during the blotting process due to diffusion through the nitrocellulose membrane pores. Polymerization increases the molecular size of the protein, which results in greater membrane retention and better detection by specific antibodies. This effect was demonstrated by the significant increase in the number of 72-kDa bands compared with the number of 36-kDa and 18-kDa bands following polymerization. Polymerization also produced a significant increase in the AOD of the 72-kDa bands. As a secondary objective, we used immunoblotting as a proxy for sensitization to study the accuracy of the SPTs and ImmunoCAP tests. Both tests were unable to detect a significant number of sensitized patients. The ImmunoCAP test demonstrated a false-negative rate of 57.8%, and the SPT demonstrated a false-negative rate of 42.3%. When the assays were combined, the false-negative rate decreased to 24.5%. These data demonstrate that these two analytical tests are complementary tools for diagnosing allergic sensitization, and a negative result from one assay does not necessarily indicate an absence of sensitization.
Failure of leukocytes to adhere to glass after ex vivo challenge with specific antigens depends mostly on cellular mechanisms resulting from the interactions of T cells, B cells and macrophages (44-46). When activated in the presence of a specific antigen, E-rosette-forming cells release soluble supernatants that interfere with the glass adherence phenomenon observed in control, unchallenged plasma (27). The involvement of T cells was also suggested by the fact that anti-θ (anti-theta) antibodies abolish the inhibition of adherence (47). Anti-θ antibodies are specifically directed against the C3H antigen associated with T cells (48). Leukotrienes, specifically LTC4 (49), are important factors in the process and are modulated by interferon secretion (50). As cysteinyl leukotriene generation by dendritic cells is a recognized step in the Dectin-2 recognition of allergens (51), the LAIT may be used to analyze this pathway indirectly.
The evaluation of cell-mediated immunoreactivity may allow the prediction of the overall ability of an allergoid to induce tolerance, but this subject remains an object of study. The actual generators of tolerance are the tolerogenic dendritic cells that prime naive T cells to become IL-10- and TGF-β1-releasing Treg cells (52,53). Dendritic cells collect macromolecules from mucosal layers via transepithelial dendritic phagocytosis (54). Oral dendritic cells (oral Langerhans cells, oLC) constitutively express high levels of high affinity IgE receptors (FcεRI) occupied by IgE antibodies that appear to be essential for the collection of antigens (55). The increase in molecular weight induced by enzymatic polymerization may theoretically promote phagocytosis and interfere with the absorption of β-Lg monomers by lipocalin receptors (56). Thus, the ability of IgE to bind an allergoid is essential and must be evaluated before the application of a tolerance-induction protocol in clinical trials. Transglutaminase may also be used to create covalent linkages between different proteins. Recombinant fusion of allergenic proteins and bacterial immunogenic proteins stimulates dendritic cell activity (57). This fusion ability of transglutaminase may theoretically be used to increase the tolerogenic activity of allergoid polymers through covalent addition of coadjuvants. This topic warrants further study.
Additionally, the perception that cow’s milk proteins such as beta-lactoglobulin may be immunogenic should stimulate the creation of human milk banks to feed premature newborns with immature digestive and immune systems (58).
In conclusion, our data support the concept that enzymatic polymerization is a tool that can decrease the in vivo allergenicity of β-Lg. As polymerization did not decrease the in vitro humoral or ex vivo cell-mediated immunoreactivity of β-Lg, we conclude that inducing polymerization by transglutaminase represents a promising technique to produce suitable molecules for the purpose of designing oral/sublingual tolerance induction protocols for the treatment of allergies.
We thank Ms. Michele Augusto Fernandes and Ms. Conceição Aparecida Vilella for their excellent technical assistance.
No potential conflict of interest was reported.
Olivier CE, Lorena SL, and Zollner RL conceived the study and manuscript, outlined the content and were integrally involved in the writing/rewriting of the final manuscript. Villa-Boas MB and Netto FM performed/supervised the transglutaminase-induced beta-lactoglobulin polymerization. Santos RA, Pinto DG, Lima RP, and Olivier CE performed/supervised the cutaneous tests. Lima RP, Pinto DG, and Olivier CE performed/supervised the immunoblotting. Lima RP, Pinto DG, Silva GK, and Olivier CE performed/supervised the leukocyte adherence inhibition tests.