


Transcription factor 7-like 2 has been shown to be associated with type 2 diabetes mellitus in multiple ethnic groups in recent years. In the Chinese Han population in particular, numerous studies have evaluated the association between the rs11196218A/G polymorphism of the transcription factor 7-like 2 gene and type 2 diabetes mellitus. However, the results have been inconsistent, so we performed a meta-analysis to assess the association. Odds ratio and 95% confidence interval values were calculated using a random-effects model or a fixed-effects model based on heterogeneity analysis. The quality of the included studies was evaluated using the Newcastle-Ottawa Scale. Subgroup analyses were conducted based on conformity with Hardy-Weinberg equilibrium in the control group as well as on other variables, such as age, sex and body mass index. Sensitivity analysis was also performed to detect heterogeneity and to assess the stability of the results. In total, 10 case-control studies comprising 7,491 cases and 12,968 controls were included in this meta-analysis. The combined analysis indicated that the rs11196218A/G polymorphism was not associated with type 2 diabetes mellitus (G vs. A, OR=1.04, 95% CI=0.97-1.13, p=0.28). The subgroup analyses also did not show any association between the rs11196218A/G polymorphism and the risk of type 2 diabetes mellitus. Furthermore, the results of the subgroup analyses indicated that the absence of an association was not influenced by age, sex or body mass index. The results of the sensitivity analysis verified the reliability and stability of this meta-analysis. In conclusion, this study indicated that there is no significant association between the rs11196218A/G polymorphism and the risk of type 2 diabetes mellitus in the Chinese Han population.
Type 2 diabetes mellitus (T2DM) is a complex metabolic disease resulting from a combination of environmental and genetic factors 1. With the development of society and the improvement of people's standard of living, the prevalence of T2DM is increasing rapidly all around the world. T2DM is very harmful to human health and life, and it also confers a heavy burden on society.
The transcription factor 7-like 2 (TCF7L2) gene, located on chromosome 10q25 2, is part of the Wnt signaling pathway 3 and has been shown to be strongly associated with an increased risk of T2DM in Icelandic 4, European 5–11, West African 12, southern Asian 13, eastern Asian 14, and Chinese 15–19 populations. The TCF7L2 gene is regarded as one of the most important genes for determining genetic susceptibility to T2DM that has been identified in humans so far.
With the growth of research efforts, studies on the association between this variation and T2DM have been extensively performed in China, but the results are disputable. Overall, the most significant risk locus identified in Chinese individuals is rs11196218. Therefore, only the rs11196218A/G polymorphism was considered in the present meta-analysis.
In contrast to a single study, meta-analyses are based on all available studies, which has improved the statistical power for exploring the above associations and has led to more reliable conclusions in recent years 20. Therefore, in the present study, a meta-analysis was performed to allow a valuable conclusion to be drawn regarding the relationship between the rs11196218A/G polymorphism and T2DM risk in the Chinese Han population.
MATERIALS AND METHODSOur study adhered to the PRISMA Statement regarding the reporting of systematic reviews and meta-analyses 21.
Search strategyIn this meta-analysis, we searched articles in PubMed, Elsevier, SpringerLink, Embase, the Cochrane Library, ISI Web of Science, Google Scholar and the China National Knowledge Infrastructure (CNKI). The search languages included English and Chinese. The following key words and subject terms were used: TCF7L2, transcription factor 7-like 2, rs11196218, diabetes mellitus, type 2, type 2 diabetes mellitus, T2DM, and T2D. The reference lists of eligible studies and relevant review papers were additionally identified via a manual search on this topic. The last research update was performed on July 15, 2014.
Inclusion and exclusion criteriaThe primary studies included in our meta-analysis had to meet the following criteria: (1) the association between the TCF7L2 polymorphism (rs11196218) and T2DM risk in the Chinese Han population was clearly evaluated, (2) the diagnosis of T2DM and the sources of the cases and controls were clearly described, (3) a case-control study design was employed, and (4) original data and sufficient information were provided to estimate the odds ratio (OR) and the corresponding 95% confidence interval (95% CI). The major reasons for exclusion were as follows: (1) duplicate data were presented; (2) the article consisted of an abstract, comment, or review or focused on pathological mechanisms; and (3) more than one article was published by the same author using the same data series, in which case the most recent published paper or the paper with the largest sample size was selected.
Quality assessmentThe Newcastle-Ottawa Scale (NOS) 22 was used to assess the quality of the studies included in our meta-analysis. The NOS contains eight items and is categorized into three dimensions: selection, comparability and exposure, for case-control studies. In particular, the selection dimension contains four items, the comparability dimension contains one item, and the exposure dimension contains three items. A star system is used to allow semi-quantitative assessment of study quality, and a study can be awarded a maximum of one star for each numbered item within the selection and exposure categories. Meanwhile, a maximum of two stars can be given for comparability. The NOS ranges from zero up to nine stars, as follows: high-quality study: more than seven stars; medium-quality study: between four and six stars; poor-quality study: less than four stars.
Data extractionFor quality control, the data were extracted by two reviewers using a standardized extraction form. If the information on the genotype distribution was inadequate, we tried to contact the authors by telephone or e-mail. The following information was extracted from each article: the last name of the first author, the year of publication, the region, the numbers of cases and controls, the source of the controls, the numbers of genotypes for cases and controls, matching factors, and the Hardy-Weinberg equilibrium (HWE) in each control group. Disagreement was resolved by consulting a third reviewer.
Ethics statementThis article reports a meta-analysis of data obtained from previous studies. All of the data were anonymized before analysis. We also confirmed that none of the data involved competing interests.
Statistical analysisIn this meta-analysis, OR and 95% CI values were used to assess the association between a polymorphism of the TCF7L2 gene (rs11196218: G vs. A) and T2DM risk. In addition, statistical significance was assessed using a Z-test, and p<0.05 indicated statistical significance for the association. The model selection was based on the heterogeneity test; therefore, the χ2-based Q-test was performed in this study 23. When the Q-test yielded a p-value of more than 0.10, a fixed-effects model was used 24; otherwise, a random-effects model was applied 25. Heterogeneity was also assessed using the I2 test. The I2 statistic was specifically documented for the percentage of study variability observed due to heterogeneity rather than chance (I2=0-25%, no heterogeneity; I2=25-50%, moderate heterogeneity; I2=50-75%, high heterogeneity; I2=75-100%, extreme heterogeneity) 26.
Subgroup analyses were performed based on HWE. Specifically, the p-values for HWE in the control group were determined using the Pearson chi-square test, regardless of whether the authors provided these values. HWE is the principal law of population genetic studies: if p>0.05, the focus conforms to HWE, and the control samples are representative. In Europeans, when excessive calories are consumed, variation in TCF7L2 can cause impaired β-cell function, indicating that body mass index (BMI) can influence the effect size of TCF7L2 variants; hence, these two factors will ultimately affect each other 27–29. This interaction may also exist in Asians. For this reason, we considered whether age, sex and BMI were matched between cases and controls in our subgroup analyses. For example, the studies showing a significant difference in age (p<0.05) between the cases and the controls were assigned to the incomparability subgroup of age, whereas those exhibiting p>0.05 were assigned to the comparability subgroup. However, due to the limited data in the studies, subgroup analyses based on environment were not conducted.
Sensitivity analysis was also performed to search for heterogeneity and to assess the stability of the results. One case-control study was omitted each time to reflect the influence of each dataset on the pooled OR.
Additionally, funnel plots were used to evaluate publication bias. All p-values were two tailed. Review Manager 5.0 (2011, The Cochrane Collaboration) software was used to perform the meta-analysis.
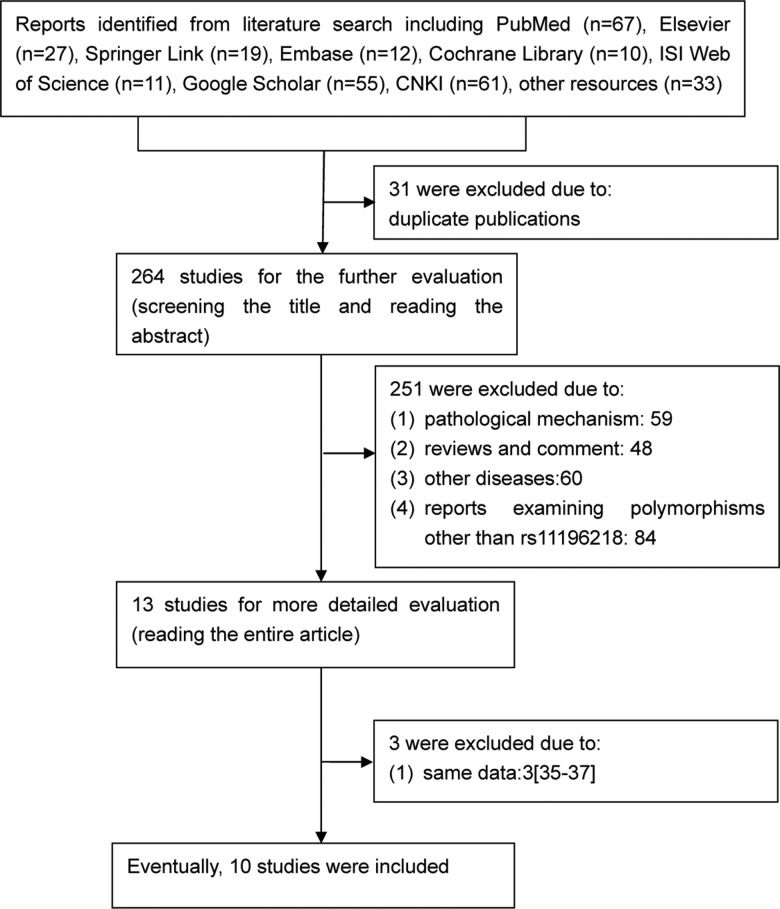
RESULTSStudies and data included in this meta-analysisIn total, 295 articles were relevant to our search terms, of which 285 papers were excluded. Thus, 10 case-control studies 15–19,30–34 comprising 7,491 cases of T2DM and 12,968 controls were ultimately included in this meta-analysis (Figure 1). All of these studies were published from 2007-2014.

The characteristics of these studies are summarized in Table 1. The genotype frequency of the single nucleotide polymorphism (SNP) was consistent with HWE in the control group (p>0.05) in all studies except for two 32,33. The quality assessment of all included studies, evaluated according to the NOS, is provided in Table 2. Most studies were of high quality in terms of selection and exposure. However, the quality of comparability was relativity low, as only 3 studies 15,33,34 were comparable with the controls regarding age, sex and BMI.
The basic characteristics of the included studies addressing rs11196218.
| First author | Publication year | Region | Source of controls | Sample sizes | Cases | Controls | HWE | Comparability | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case | Control | G | A | G | A | ||||||
| Ng | 2007 | Hong Kong | Community-based and hospital staff | 433 | 419 | 676 | 190 | 599 | 239 | Yes | Age*, sex*, BMI** |
| Zhang | 2008 | Hunan | Hospital-based | 536 | 475 | 716 | 272 | 623 | 221 | Yes | Age*, sex**, BMI* |
| Luo | 2009 | Beijing | Hospital-based | 500 | 500 | 684 | 252 | 696 | 240 | No | Age**, sex**, BMI** |
| Ma | 2010 | Shanghai | Hospital-based | 259 | 200 | 309 | 209 | 240 | 168 | Yes | Age**, sex*, BMI** |
| Lin | 2010 | Chengdu | Hospital-based | 1529 | 1439 | 2171 | 887 | 2015 | 863 | Yes | Age**, sex*, BMI** |
| Wen | 2010 | Shanghai | N/D | 1165 | 1136 | 1699 | 629 | 1677 | 595 | No | Age*, sex*, BMI* |
| Zhu | 2011 | Anhui | Hospital-based | 300 | 300 | 156 | 444 | 122 | 478 | Yes | Age*, sex*, BMI* |
| Zheng | 2012 | Chongqing | Hospital-based | 227 | 152 | 340 | 114 | 218 | 86 | Yes | Age*, sex**, BMI** |
| Qiao | 2012 | Harbin | Hospital-based | 700 | 560 | 1025 | 367 | 819 | 295 | Yes | Age*, sex*, BMI* |
| Zhai | 2014 | Henan | Community-based and Hospital-based | 1842 | 7777 | 2639 | 967 | 111287 | 4041 | Yes | Age**, sex**, BMI** |
Abbreviations: HWE, Hardy-Weinberg equilibrium; Yes, the genotype distribution conformed to HWE in the control group; No, the genotype distribution not conform to HWE in the control group;
Hospital-based: subjects who were enrolled from health checks conducted at the hospital; community-based and hospital staff: subjects who were enrolled from the community and hospital staff; N/D: no description; *: p>0.05; **: p<0.05.
Quality assessment of all of the included studies.
| First author | Publication year | Selection | Comparability | Exposure |
|---|---|---|---|---|
| Ng | 2007 | ⋆⋆⋆ | ⋆ | ⋆ |
| Zhang | 2008 | ⋆⋆ | ⋆ | ⋆⋆ |
| Luo | 2009 | ⋆⋆ | ⋆ | ⋆⋆ |
| Ma | 2010 | ⋆⋆ | ⋆ | ⋆⋆ |
| Wen | 2010 | ⋆⋆ | ⋆⋆ | ⋆⋆⋆ |
| Lin | 2010 | ⋆⋆ | ⋆ | ⋆⋆ |
| Zhu | 2011 | ⋆⋆⋆⋆ | ⋆⋆ | ⋆⋆ |
| Zheng | 2012 | ⋆⋆⋆⋆ | ⋆ | ⋆⋆ |
| Qiao | 2012 | ⋆⋆⋆ | ⋆⋆ | ⋆ |
| Zhai | 2014 | ⋆⋆ | ⋆ | ⋆⋆ |
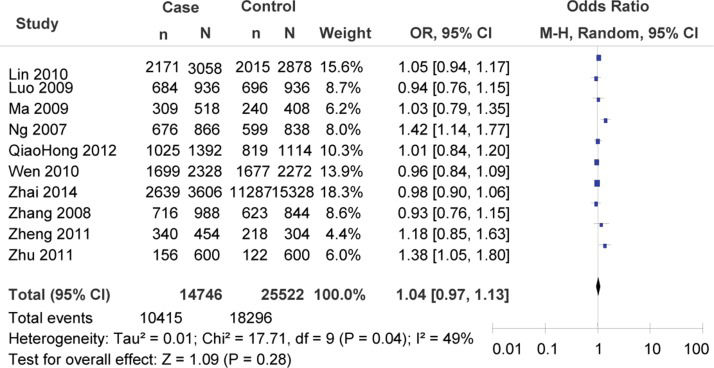
Using the heterogeneity test, we detected heterogeneity among the studies in comparisons of the risk of carrying allele G. Thus, a random-effects model was applied for the meta-analysis. The results indicated that the rs11196218A/G polymorphism was not associated with the risk of T2DM (G vs. A: OR=1.04, 95% CI=0.97-1.13, p=0.28; heterogeneity test χ2=17.71, p=0.04, I2=49%; Figure 2).
. n indicates the total number of G alleles, and N indicates the total number of G alleles plus A alleles.")
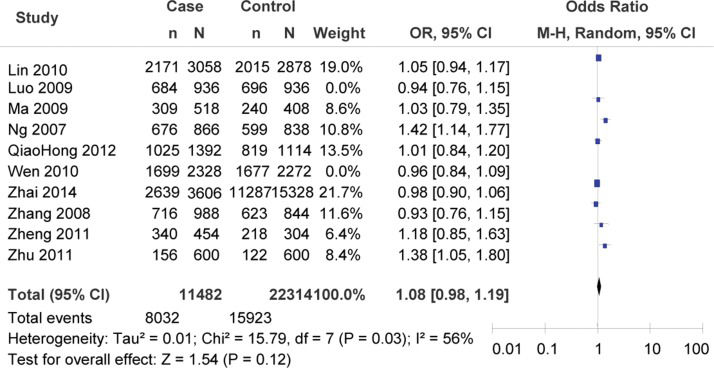
The subgroup meta-analysis of the studies that exhibited consistency with HWE in the control group also showed that there was no association between the rs11196218A/G polymorphism and T2DM risk (G vs. A: OR=1.08, 95% CI=0.98-1.19, p=0.12; heterogeneity test χ2=15.79, p=0.03, I2=56%; Figure 3).
. n indicates the total number of G alleles, and N indicates the total number of G alleles plus A alleles.")
The subgroup meta-analysis of the studies based on age indicated that there was no significant association between the rs11196218A/G polymorphism and T2DM risk (subgroup of age comparability: OR=1.11, 95% CI=0.96-1.28, p=0.18; heterogeneity test χ2=14.81, p=0.01, I2=66%; subgroup of age incomparability: OR=1.00, 95% CI=0.94-1.06, p=0.93; heterogeneity test χ2=1.45, p=0.69, I2=0%).
The subgroup meta-analysis of the studies based on sex demonstrated that there was no significant association between the rs11196218A/G polymorphism and T2DM risk (subgroup of sex comparability: OR=1.10, 95% CI=0.98-1.24, p=0.12; heterogeneity test χ2=13.04, p=0.02, I2=62%; subgroup of sex incomparability: OR=0.98, 95% CI=0.91-1.05, p=0.49; heterogeneity test χ2=1.58, p=0.66, I2=0%).
Finally, the subgroup meta-analysis of the studies based on BMI illustrated that there was no significant association between the polymorphism and T2DM risk (subgroup of BMI comparability: OR=1.03, 95% CI=0.90-1.17, p=0.72; heterogeneity test χ2=6.21, p=0.10, I2=52%; subgroup of BMI incomparability: OR=1.06, 95% CI=0.96-1.18, p=0.26; heterogeneity test χ2=11.32, p=0.05, I2=56%).
Sensitivity analysisA single study included in the meta-analysis was omitted each time to reflect the influence of each dataset on the pooled OR values. We found that no single study could change the pooled results (Table 3), which indicated that the results were relatively reliable.
The results of the sensitivity analysis with each rs11196218A/G-focused study omitted.
| Study omitted | OR | 95% CI | p-value |
|---|---|---|---|
| Lin et al. | 1.01 | 0.96-1.07 | 0.62 |
| Luo et al. | 1.03 | 0.98-1.08 | 0.32 |
| Ma et al. | 1.02 | 0.97-1.07 | 0.44 |
| Ng et al. | 1.00 | 0.95-1.05 | 0.90 |
| Qiao et al. | 1.02 | 0.97-1.07 | 0.41 |
| Wen et al. | 1.03 | 0.98-1.09 | 0.26 |
| Zhai et al. | 1.04 | 0.98-1.11 | 0.16 |
| Zhang, Y. | 1.03 | 0.98-1.08 | 0.32 |
| Zheng et al. | 1.02 | 0.97-1.07 | 0.50 |
| Zhu, H. | 1.01 | 0.96-1.06 | 0.69 |
Abbreviations: OR, odds ratio; CI, confidence interval.
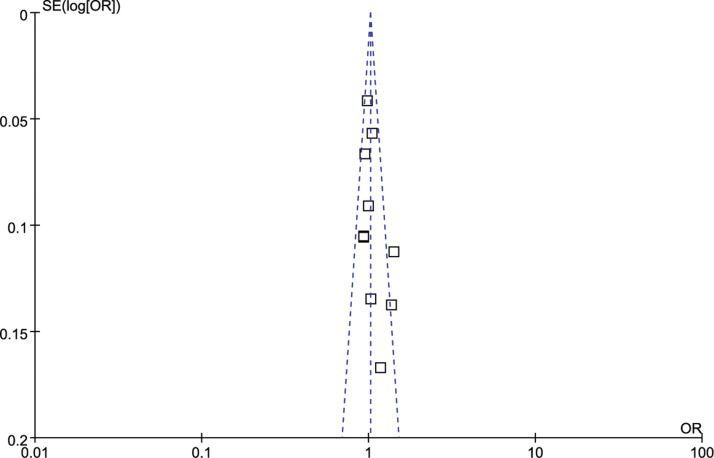
The shape of the funnel plots was symmetrical, suggesting that there was no evidence of publication bias for the rs11196218A/G polymorphism (Figure 4).
DISCUSSION. Each point represents an independent study on the indicated association. The dark point represents two overlapping articles.")
Since the initial discovery that TCF7L2 is strongly associated with an increased risk of T2DM in Icelandic populations in 2006 4, many replication studies have confirmed the role of TCF7L2 in conferring susceptibility to T2DM in different populations and ethnic groups 5,7,11,14,38,39, especially for the rs7903146C/T polymorphism. However, in the Chinese population, rs7903146 is very rare, and several studies have indicated that rs11196218 is the most significant risk variant 17. Nevertheless, the results regarding the rs11196218A/G polymorphism and T2DM risk have been inconsistent for the Chinese Han population. Certain studies 15–19 confirmed that the G allele of the rs11196218A/G polymorphism was significantly associated with T2DM risk, whereas studies by Ma 30, Zheng et al. 31, Luo et al. 32, Wen et al. 33 and Qiao et al. 34 did not find a significant association between the rs11196218A/G polymorphism and T2DM risk in the Chinese Han population. Therefore, to resolve the conflict among these studies, we performed a meta-analysis to assess the association between the rs11196218A/G polymorphism and T2DM risk.
Previously, Luo et al. 32 conducted a meta-analysis to evaluate the effect of TCF7L2 on genetic susceptibility to T2DM in the East Asian population. However, only one article analyzed included samples from the Chinese Han population. In the current study, to increase the statistical power of the analysis, a larger amount of data was collected from the literature to perform an up-to-date meta-analysis for the Chinese Han population.
Our meta-analysis, which included 7,491 T2DM cases and 12,968 controls from 10 case-control studies, explored the association between rs11196218A/G and T2DM risk. Overall, we did not find that the rs11196218A/G polymorphism was significantly associated with an increased risk of T2DM in the Chinese Han population, which is consistent with the findings of Ma 30, Zheng et al. 31, Luo et al. 32, Wen et al.33 and Qiao et al. 34. However, a previous meta-analysis performed by Luo et al. 32 found that rs11196218 showed a marginal association with T2DM risk (OR=1.09, 95% CI=1.00-1.19, p=0.059). The most plausible explanation for this discrepancy is the different genetic backgrounds associated with different ethnic groups, areas and population substructures.
In the present study, obvious heterogeneity was observed in the comparisons among studies. Thus, a random-effects model was applied for the meta-analysis, after which we conducted a sensitivity analysis to identify the source of the heterogeneity. After omitting the study by Ng et al. 17 from the analysis, there was no heterogeneity among the remaining studies. One plausible explanation for the influential role of this study was that the populations examined by Ng et al. 17 resided in the metropolis of Hong Kong; as the residents of Hong Kong emigrated from different areas of China, they have probably undergone population admixture. Moreover, T2DM is a complex hereditary disease, so the historical immigration, complex ancestries, population movement, and recent intermarriages with other ethnic groups that have occurred in Hong Kong may have resulted in different risk factors in different people 40. Therefore, the genetic origins of risk may be relatively different between this region and other areas. Pritchard et al. 41 also suggested that low diversity may be sufficient to lead to different results. However, although heterogeneity was observed among studies, the results of the sensitivity analysis verified the reliability and stability of the present meta-analysis.
T2DM is a complex hereditary disease caused by genetic and environmental factors (1). Other confounding factors, such as age, sex, BMI, the environment and sophisticated gene-gene and gene-environment interactions, may also affect the results of studies on T2DM. Thus, the subgroup analyses in the present study were also conducted based on variables such as age, sex and BMI. However, the results indicated that the association of the rs11196218A/G polymorphism with T2DM was not influenced by age, sex or BMI in the studied population. Due to the limited data available in the studies analyzed, subgroup analyses based on the environment and gene-gene and gene-environment interactions were not conducted.
There were certain advantages of our meta-analysis. First, to the best of our knowledge, this is the most comprehensive meta-analysis of the association between the rs11196218A/G polymorphism of the TCF7L2 gene and T2DM risk in the Chinese Han population conducted to date, and our analysis had improved statistical power for exploring this association. Second, the protocol for this meta-analysis, using explicit methods and criteria for study selection, data extraction, and data analysis, was well designed before it was initiated. Third, a stringent searching strategy based on computer-assisted and manual searches was applied to include as many eligible studies as possible. Finally, the quality of the studies included in our meta-analysis was satisfactory; in fact, each article exhibited at least five stars. However, there were still certain limitations of this meta-analysis. First, the sample sizes of several of the studies included in our meta-analysis were relatively small. Second, due to the limited information on environment and lifestyle available the included studies, it was not possible to perform a subgroup meta-analysis or an interaction analysis based on environment or lifestyle. Finally, similar to a case-control study, a meta-analysis is a retrospective study, and recall bias might also exist.
In conclusion, we did not find any association between the TCF7L2 gene rs11196218A/G polymorphism and T2DM risk in the Chinese Han population. To achieve a better and more comprehensive understanding of the association between TCF7L2 gene polymorphisms and T2DM risk, we suggest that studies including large samples and different ethnicities and lifestyles and examining sophisticated gene-gene and gene-environment interactions should also be considered in future analyses.
AUTHOR CONTRIBUTIONSMa ET and Wei L developed the idea for the study and drafted the manuscript. Ma ET, Wei L, Wang HL and Tian RR were responsible for conducting the search, the data collection and the study quality assessment. Ma ET, Wei L Wang HL and Guo J analyzed and interpreted the data. All of the authors read and approved the final version of the manuscript.