



This revision describes in detail the different diagnostic techniques of catheter-related infection, both in terms of catheter removal and preservation. Culture techniques based on catheter withdrawal are classified depending on the detection of extraluminal and/or intraluminal colonization, and new methodologies are described. In general, the most important recommendations are: (a) do not send for culture catheter tips without suspicion of infection, (b) Maki's technique is the standard for detecting extraluminal colonization, (c) take 2 pairs of peripheral blood cultures before starting antibiotic treatment, (d) use skin and connections/connectors cultures for the conservative diagnosis due to their high negative predictive value (Gram and culture), and (e) take differential quantitative blood cultures though all catheter lumens and through a peripheral vein.
Esta revisión describe con detalle las diferentes técnicas diagnósticas de infección relacionada con el catéter, tanto con la retirada como con la conservación del mismo. Las técnicas de cultivo basadas en la retirada del catéter se clasifican en base a la detección de colonización extraluminal, intraluminal, o ambas, asimismo, se describen nuevas metodologías. De forma general, las recomendaciones más importantes son: a) no enviar para cultivo puntas de catéter retiradas sin sospecha de infección, b) la técnica de Maki es el estándar válido de detección de colonización extraluminal, c) tomar 2 parejas de hemocultivos de sangre periférica antes de iniciar tratamiento antibiótico, d) utilizar cultivos de piel y conexiones/conectores para el diagnóstico conservador por su alto valor predictivo negativo (Gram y cultivo), y e) extraer hemocultivos cuantitativos diferenciales por todas las luces del catéter y por vena periférica.
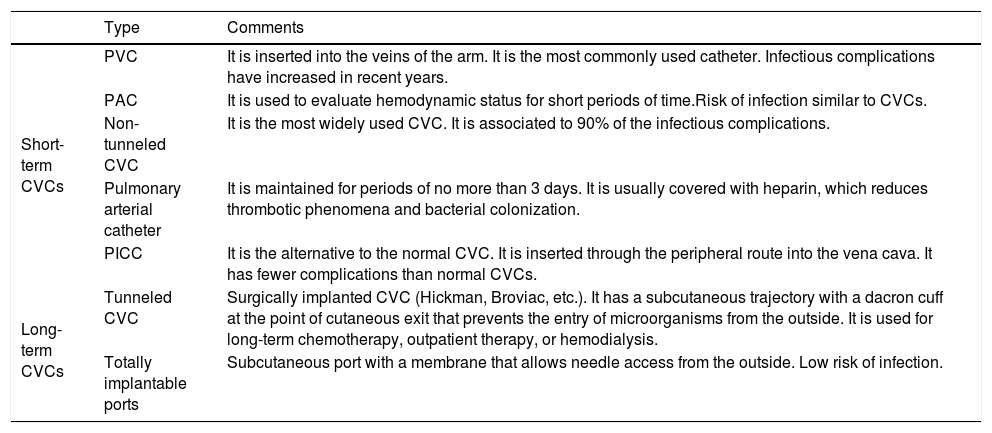
Intravascular catheters (IC) are widely used for diagnostic and therapeutic purposes. Based on EPINE data, almost 70% of patients admitted in Spanish hospitals have at least one catheter inserted.1 Local and systemic infections are one of the main complications associated with the use of IC, which are related to high morbidity and mortality rates. There are several types of IC (Table 1), but central venous catheters (CVCs) are the cause of 90% of catheter-related bloodstream infections (C-RBSI), although peripheral catheters are having increasing rates of infection. C-RBSI rate is approximately 1.18 episodes/1000 admissions, ranging from 0.5 to 2.7 in peripheral and central venous catheters, respectively.
Types of intravascular catheters most commonly used.
| Type | Comments | |
|---|---|---|
| Short-term CVCs | PVC | It is inserted into the veins of the arm. It is the most commonly used catheter. Infectious complications have increased in recent years. |
| PAC | It is used to evaluate hemodynamic status for short periods of time.Risk of infection similar to CVCs. | |
| Non-tunneled CVC | It is the most widely used CVC. It is associated to 90% of the infectious complications. | |
| Pulmonary arterial catheter | It is maintained for periods of no more than 3 days. It is usually covered with heparin, which reduces thrombotic phenomena and bacterial colonization. | |
| PICC | It is the alternative to the normal CVC. It is inserted through the peripheral route into the vena cava. It has fewer complications than normal CVCs. | |
| Long-term CVCs | Tunneled CVC | Surgically implanted CVC (Hickman, Broviac, etc.). It has a subcutaneous trajectory with a dacron cuff at the point of cutaneous exit that prevents the entry of microorganisms from the outside. It is used for long-term chemotherapy, outpatient therapy, or hemodialysis. |
| Totally implantable ports | Subcutaneous port with a membrane that allows needle access from the outside. Low risk of infection. |
CVC, central venous catheter; PVC, peripheral venous catheter; PAC, peripheral arterial catheter; PICC, peripherally inserted central venous catheter.
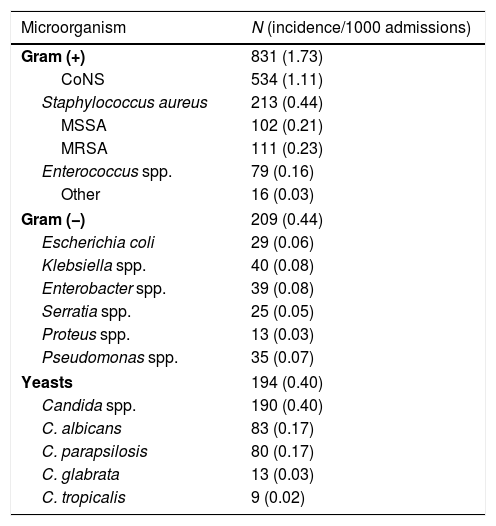
The most frequent causative agents of C-RBSI are Gram-positive microorganisms, followed by Gram-negative and yeasts. Table 2 shows the etiology of C-RBSI episodes between 2003 and 2010 at the Hospital General Universitario Gregorio Marañón (Madrid, Spain). Coagulase negative staphylococci (CoNS) caused 43.3% of C-RBSI, followed by Staphylococcus aureus (17.3%), Gram-negative bacilli (17%), and yeasts (16%).
Main microorganisms producing catheter-related bloodstream infections. Data from the Hospital General Universitario Gregorio Marañón de Madrid (2003–2010).
| Microorganism | N (incidence/1000 admissions) |
|---|---|
| Gram (+) | 831 (1.73) |
| CoNS | 534 (1.11) |
| Staphylococcus aureus | 213 (0.44) |
| MSSA | 102 (0.21) |
| MRSA | 111 (0.23) |
| Enterococcus spp. | 79 (0.16) |
| Other | 16 (0.03) |
| Gram (−) | 209 (0.44) |
| Escherichia coli | 29 (0.06) |
| Klebsiella spp. | 40 (0.08) |
| Enterobacter spp. | 39 (0.08) |
| Serratia spp. | 25 (0.05) |
| Proteus spp. | 13 (0.03) |
| Pseudomonas spp. | 35 (0.07) |
| Yeasts | 194 (0.40) |
| Candida spp. | 190 (0.40) |
| C. albicans | 83 (0.17) |
| C. parapsilosis | 80 (0.17) |
| C. glabrata | 13 (0.03) |
| C. tropicalis | 9 (0.02) |
CoNS, coagulase negative staphylococci; MSSA, methicillin-susceptible Staphylococcus aureus; MRSA, methicillin-resistant Staphylococcus aureus.
Catheter colonization occurs by progression of microorganisms to the tip of the catheter along either the inner surface (≥7 days of indwelling time) or the outer surface (<7 days of indwelling time) of the catheter. Depending on the pathogenesis there are different diagnostic procedures based on extra or intraluminal colonization, which are described below.2
Diagnostic procedures based on catheter withdrawalAccurate diagnosis when there is suspicion of catheter-related infection (CRI) requires catheter withdrawal. However, routine catheter tip cultures are not recommended. The catheter may be removed when any of the following circumstances occur: unnecessary catheters, easy to replace catheters, catheters in patients with bacteremia that persists despite correct antimicrobial treatment, catheters with infection in the subcutaneous tunnel, catheters causing pulmonary emboli or major circulation, catheters causing endocarditis, and catheters infected by difficult-to-eradicate microorganisms.
The sample to be processed will be the final segment of the catheter, specifically the last 5cm. Shorter segments may mean that the end of some lumens in the multi-lumen catheters are lost. In pulmonary arterial catheters, the most representative sample is the introducer. In the special case of totally implantable ports, the reservoir must be cultured in addition to the tip.
The catheter tip, placed in a sterile, properly identified dry container, should be sent immediately to the laboratory, where it should either be processed on arrival or kept refrigerated. Catheters coated with antiseptics or antibiotics can affect culture result, significantly underestimating the bacterial load and this should be taken into account when interpreting the results.3
Cultures for detection of extraluminal colonizationThe semiquantitative Maki's technique described in 1977 is still the standard for a rapid and easy culture of the external catheter tip surface.4 It consists of rolling the catheter tip forth and across a blood agar plate. Colonization is defined when ≥15cfu/plate are recovered after 24–48h of incubation at 37°C under aerobic conditions. However, when endoluminal colonization occurs (approximately 15% of C-RBSI are from endoluminal source), it can be misdiagnosed using Maki's technique. Therefore, the combination of this technique with others that detect intraluminal colonization can solve this problem. Another limitation is that only one type of culture media and one culture condition are used. Therefore, in case of suspicion of infection by other microorganisms with special nutritional requirements, other media and incubation conditions must be used.5
Nevertheless, even in long-term catheters, several authors demonstrated that Maki's technique was not inferior to other quantitative techniques which detect intraluminal colonization.
Cultures for detection of intraluminal colonizationIn 1985 Liñares et al. described a modification of Cleri's technique to quantify colonizing microorganisms inside the catheter lumen.6 It consists of flushing 3 times the catheter lumen with 2ml of tryptic soy broth followed by culture. Colonization was set at 1000cfu/ml. However, it is susceptible of contamination during manipulation and it is practically out of use.
Cultures for detection of extra and intraluminal colonizationIn 1990 Brun-Buisson simplified Cleri's technique by vortexing the catheter tip into 1ml of sterile water followed by culture.7 They report a 97.5% sensitivity and 88% specificity using the same Cleri's cut-off. A similar procedure was described by Sherertz et al. which consists of sonicating the catheter tip into 10ml of enrichment broth followed by culture.8 Sensitivity and specificity was 93% and 94%, respectively using a cut-off of 100cfu/ml. However, when this procedure was compared with other techniques, none of them individually had a sensitivity higher than 58% to detect catheter colonization.
Recently, Guembe et al. suggested an optimized and simplified version by pre-cutting the catheter tip before sonication (2–5mm fragments).9 With this modification they obtained better validity values than Maki's technique in adults’ CVCs.
Another recent finding in pediatric population was demonstrated by Martín-Rabadán et al., as in neonatal silicone peripherally inserted central venous catheters (PICCs) Maki's technique misdiagnosed almost half of colonized catheters.10,11 They proposed an alternative method based on the longitudinal cutting of the tip previous to Maki's technique. A similar loss of diagnosis occurred in reservoir ports, so culture of the inside and outside of ports in addition to catheter tip must be performed.12,13
Rapid diagnostic techniquesThere are 4 main techniques: Gram stain of the catheter tip, it is out of use as it requires special microscopes and translucent catheters14; Gram stain of impressions from the external surface of the catheter, mainly used for rule out C-RBSI15; acridine orange stain, it is out of use by its toxicity; and molecular techniques, such as PCR and sequencing of 16S rRNA and MALDI-TOF, that have been applied in some situations, but it is necessary to further investigate its use. Despite they are faster than conventional culture, they do not allow neither microorganism's identification nor susceptibility testing assays. Besides, they cannot be applied in the laboratory routine.
Microorganisms’ identificationThe certainty diagnosis of CRI requires that the same microorganism must be present in the different samples obtained. The use of MALDI-TOF has been a revolution due to the immediacy and accuracy of bacteria and fungi identification. However, the similarity between the different strains isolated from the CRI specimens should be established as reliably as possible (by means of molecular techniques), especially in the case of coagulase-negative staphylococci.16
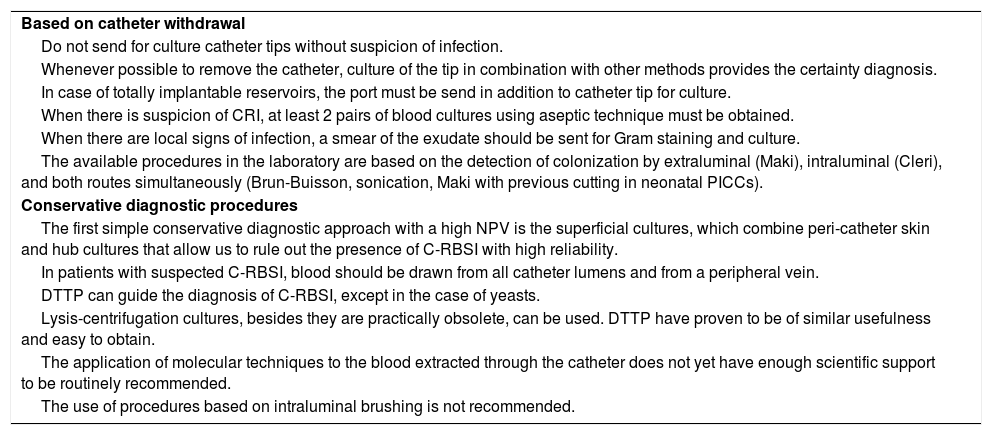
In Table 3 there is a summary with the general recommendations for diagnostic procedures based on catheter withdrawal.
Summary recommendations for diagnostic procedures of catheter-related infections.
| Based on catheter withdrawal |
| Do not send for culture catheter tips without suspicion of infection. |
| Whenever possible to remove the catheter, culture of the tip in combination with other methods provides the certainty diagnosis. |
| In case of totally implantable reservoirs, the port must be send in addition to catheter tip for culture. |
| When there is suspicion of CRI, at least 2 pairs of blood cultures using aseptic technique must be obtained. |
| When there are local signs of infection, a smear of the exudate should be sent for Gram staining and culture. |
| The available procedures in the laboratory are based on the detection of colonization by extraluminal (Maki), intraluminal (Cleri), and both routes simultaneously (Brun-Buisson, sonication, Maki with previous cutting in neonatal PICCs). |
| Conservative diagnostic procedures |
| The first simple conservative diagnostic approach with a high NPV is the superficial cultures, which combine peri-catheter skin and hub cultures that allow us to rule out the presence of C-RBSI with high reliability. |
| In patients with suspected C-RBSI, blood should be drawn from all catheter lumens and from a peripheral vein. |
| DTTP can guide the diagnosis of C-RBSI, except in the case of yeasts. |
| Lysis-centrifugation cultures, besides they are practically obsolete, can be used. DTTP have proven to be of similar usefulness and easy to obtain. |
| The application of molecular techniques to the blood extracted through the catheter does not yet have enough scientific support to be routinely recommended. |
| The use of procedures based on intraluminal brushing is not recommended. |
As some catheters are unnecessary withdrawn and removing the catheter is not always possible, it is accepted to eradicate CRI by remaining the catheter in place. In such cases, the diagnostic procedures should be based on strategies that do not require the tip or fragments of the catheter to be available for study. These methods allow to anticipate tip colonization and to identify patients at risk of C-RBSI, being able to rule out the catheter as the source of the bacteremia and thus avoiding the unnecessary removal of the catheter.
Semiquantitative superficial culturesThey are based on the application of knowledge of the main pathways of microorganisms to the tip of the catheter: the surrounding skin at the insertion site (extraluminal) and the inside of the catheter hubs (intraluminal). The detection of ≥15cfu/plate in any of them defines colonization. They are a simple and inexpensive approach to the conservative diagnosis of CRI.
Many studies have been performed to assess the validity values of this procedure in several populations. It was in 1990 when Cercenado et al. used the term “superficial cultures” and the main finding was that they had a 99% of negative predictive value (NPV). However, the positive predictive value (PPV) was 34%.17 Fortún et al. improved it to 88.5% by additionally culturing the first 2cm of the subcutaneous segment.18
Moreover, as cultures from the inside of the hubs may dislodge the biofilm into the bloodstream, Pérez-Granda et al. recently report an alternative procedure based on instillation of enrichment broth through the withdrawn closed connector, showing slightly better results than conventional hub cultures combined with skin cultures (sensitivity >80% and NPV >90%).19
Despite there are few studies assessing the validity of Gram staining of the insertion site and hubs smears, it gives immediate information to rule out C-RBSI (negative predictive value of 97%).20
Culture and staining of blood drawn through the catheterCultures drawn through all lumens of an infected catheter compared to cultures drawn through a peripheral vein allow to certainly determine C-RBSI. They are based on the fact that the number of cfu/mL of bacteria is higher in the blood drawn through the catheter than in the blood drawn through the peripheral vein. For quantitative differential cultures, 10ml of blood are placed in special lysis-centrifuge tubes to lyse red cells with detergents, so the leukocyte-rich layer is cultured into agar plates. Blood must be drawn though all catheter lumens so as not to lose almost 30% of the diagnosis of C-RBSI. Cultures should be performed before initiating antimicrobial therapy and with the same volume of blood per bottle. To confirm an episode of C-RBSI, colony counts of microorganisms grown from blood obtained through the catheter hub must be at least 3-fold greater than the colony counts from blood obtained from a peripheral vein. The greatest advantage of the quantitative technique, performed by means of the lysis-centrifugation procedure, is that it allows the diagnosis of CRI, in the case of positive blood cultures, and avoids unnecessary catheter removals in those cases with negative blood cultures. The main limitations of this method are associated to its complexity and the requirement for immediate processing by the Microbiology laboratory.2
Additionally, differential quantitative blood cultures, based on a pour-plate technique in which blood is mixed with 80ml of BHI agar and poured intro Petri dishes, are also reliable using a cut-off value of a fourfold difference between blood samples drawn from the catheter and a peripheral vein. It was demonstrated by Capdevila et al. that this technique had a sensitivity of 94%, a specificity of 100%, and positive predictive value of 100% for C-RBSI.21
Techniques based on the growth rate of blood culturesThey are based on that the greater the inoculum of microbes inoculated into blood culture bottles, the shorter the incubation required to detect microbial growth. This technique is also considered an accurate diagnostic method for detecting C-RBSI without removing the catheter.
Blot et al. established in 120min the significant growth difference between the paired samples, with a sensitivity of 94% and a specificity of 91% in the diagnosis of C-RBSI (with bacteria) and has been proposed for routine use in practice in hospitals with automated bacteremia detection systems.22 Other studies with short and long-term CVCs obtained similar percentages.
The main drawbacks of this technique (differential time to positivity, DTTP) are: difficulty in differentiating false positives and true infections in blood cultures, blood cultures obtained from the different lumens of the catheter must be correctly identified, blood must be drawn though all catheter lumens, blood volume is a key factor in the profitability of a blood culture, it is also important to collect the first milliliters of blood drawn through the catheter, they require immediate incubation, and they cannot be applied to fungal and polymicrobial infections.2
The combined use of several conservative techniques increases sensitivity and specificity in the diagnosis of C-RBSI.23 Subsequently, the use of the DTTP for the diagnosis of C-RBSI would be useful as a confirmatory method. If the paired blood cultures are positive for the same microorganism, but the DTTP is less than 2h or, if the blood culture of the catheter is negative, the catheter does not need to be removed.
Molecular techniques of blood drawn through the catheterThe diagnosis of C-RBSI by molecular techniques without catheter removal has been studied mainly in blood samples and studies have been limited to very specific groups of patients (hematological or neutropenic). There are few studies on the use of molecular techniques in samples other than blood, which are described below.
Techniques applied to positive blood culturesAmplification techniques: GenomEra (Abacus) to detect S. aureus and Streptococcus pneumoniae; GeneXpert (Cepheid) and BD GeneOhm (Becton-Dickinson) to detect S. aureus. In recent years, multiple PCR platforms have been developed, such as the FilmArray (bioMérieux) system using multiple nested PCRs or the Verigene (Luminex) and Prove-it Sepsis (Mobidiag) systems using multiple PCRs with microarray panel hybridization.
Other methods include isothermal amplification techniques (LAMP, loop-mediated isothermal amplification), such as Eazyplex MRSA (Amplex Biosystems GmbH), which detects S. aureus and coagulase-negative staphylococci.
In situ hybridization techniques with fluorescent probes (FISH), in particular the PNA-FISH technique (Pathogen-Specific Methods Peptide nucleic acid, AdvanDx), uses probes that bind to the 16S rRNA genes of bacteria and 18S rRNA in yeasts. They allow the identification of S. aureus, coagulase-negative staphylococci, E. faecalis, Enterococcus spp., E. coli, K. pneumoniae, P. aeruginosa, C. albicans, C. glabrata, C. krusei, C. parasilopsis and C. tropicalis.
Probe techniques, such as the AccuProbe system (Hologic), which uses specific DNA probes to detect S. aureus, S. pneumoniae, Enterococcus spp. and Streptococcus of groups A and B; or the mixed Sepsis Flow Chip system (SFC, Master Diagnostica) based on a multiplex PCR followed by automatic membrane hybridization with specific DNA probes using DNA-Flow technology (hybriSpot HS24).
Techniques applied directly to the patient's blood- 1.
PCR-based techniques: (a) Real-time PCR, SepsiTest (Molzym GmbH), detects 345 pathogens using 16S rRNA bacterial and 18S rRNA fungal targets or Magicplex Sepsis Real-Time (Seegene), detects 85 bacterial species and 6 fungi; (b) Multiplex PCR, such as VYOO (Analytik Jena AG), detects 34 bacterial and 7 fungal species; LightCycler SeptiFast (Roche Molecular Diagnostics), real-time multiplex PCR in combination with FRET probes, detects 25 bacterial species, 5 yeasts and Aspergillus fumigatus; or IRIDICA BAC-BSI Assay (Abbott Molecular), a multiplex PCR associated with a mass spectrometry system.
- 2.
Nanotechnology techniques: based on magnetic resonance, T2MR (T2 Biosystems), for the detection of Candida species.
- 3.
Techniques based on sequencing: still under evaluation, iDTECT Dx Blood (Pathoquest) sequences the entire genome of 800 bacterial species and 400 viruses; and LiDia BSI test (DNAe), a technique that captures microbial DNA with immunomagnetic balls by performing an ion-sensitive field effect transistor (ISFET) based sequencing on a microchip.
These techniques have several problems such as low blood load of microorganisms (1–10cfu/mL), variety of microorganisms under study, presence of inhibitors, interferences with the human genome, contaminating DNA or DNA from dead microorganisms.
There is still not enough information to replace traditional cultures or to recommend the implementation of molecular techniques for C-RBSI diagnosis in clinical practice. It is expected that new methods will be designed to solve the current problems of these techniques, especially with the great advances that are taking place in mass sequencing and nanotechnology techniques.
In Table 3 there is a summary with the general recommendations for conservative diagnostic procedures.
ConclusionsIn accordance with the new guidelines on the diagnosis and treatment of catheter-related infections developed by SEIMC and SEMICYUC in 2017,24 the following conclusions regarding the diagnosis of CRI are detailed:
- •
Only catheter tips from patients with signs and symptoms of infection should be sent to the Microbiology laboratory for culture. Systematic surveillance cultures are not recommended.
- •
Samples from patients with severe and critically ill C-RBSI require urgent attention by the microbiologist.
- •
In patients in whom the catheter is removed due to suspected sepsis, at least two pairs of peripheral blood cultures should be taken by aseptic technique before antibiotic treatment is started.
- •
Maki's semi-quantitative procedure remains a valid standard in routine use. Other techniques that detect the presence of intraluminal and/or extraluminal colonization are considered suitable alternatives for special situations.
- •
Qualitative catheter cultures should not be performed.
- •
The identification of CRI-related microorganisms at the genus and species level, the determination of the biotype and the study of the antimicrobial susceptibility pattern are recommended. Molecular typing techniques are reserved for research studies.
- •
In patients, in whom the catheter is intended to be preserved, a semi-quantitative study of skin and hubs/connectors is recommended due to their high negative predictive value (NPV).
- •
If there are local signs of infection, a Gram stain and swab culture may be helpful.
- •
In critical patients with suspected sepsis, Gram staining of skin and hubs allows, due to their NPV, to provide faster information for decision making. The results must be confirmed with the culture.
- •
Quantitative differential blood cultures of blood, taken by all catheter lumens and by a peripheral vein, are a recommended procedure in the conservative diagnosis of C-RBSI.
This work has been supported by the Spanish Society for Clinical Microbiology and Infectious Diseases (SEIMC).
Conflicts of interestThe authors have no conflicts of interest to declare.
We thank members of the editorial board of EIMC for the opportunity to publish this scientific document.

