



Serogroup 6 of Streptococcus pneumoniae initially consisted of the 6A and 6B serotypes, but in recent years, the 6C and 6D serotypes were reported. The aim of this study was to determine the frequency and molecular characterization of invasive S. pneumoniae isolates serotypes 6C and 6D in Colombia, from 1994 to 2013.
MethodologyAll the isolates recovered during the surveillance from 1994 to 2013, and identified as 6A or 6B, were re-tested to detect the serotypes 6C and 6D. The serotyping was performed using the Quellung reaction and PCR. The susceptibility testing was performed on penicillin, erythromycin, ceftriaxone, trimethoprim/sulfamethoxazole, chloramphenicol, tetracycline and vancomycin. Molecular typing was performed using pulsed-field gel electrophoresis and multilocus sequence typing.
ResultsFrom a total of 271 and 350 isolates serotyped previously as serotypes 6A and 6B, 61 (22.5%) and 15 (4.3%) were recognized as 6C and 6D, respectively. Isolates presented with low resistance to antimicrobials. Serotype 6C isolates were mainly associated with ST9007 (42.6%) and ST9008 (19.7%), and serotype 6D isolates with ST1135 (80%).
ConclusionThis study showed the circulation of serotype 6C and 6D in Colombia between 1994 and 2013, information that is important to determine the dynamics of these recently described serotypes.
el serogrupo 6 de Streptococcus pneumoniae estaba conformado inicialmente por los serotipos 6A y 6B, pero en los últimos años los serotipos adicionales 6C y 6D fueron reportados. El objetivo de este estudio fue determinar la frecuencia y la caracterización molecular de aislamientos invasivos de S.pneumoniae serotipos 6C y 6D en Colombia, desde 1994 a 2013.
MetodologíaTodos los aislamientos recuperados durante la vigilancia 1994-2013 e identificados como 6A o 6B se analizaron para detectar los serotipos 6C y 6D. La serotipificación se realizó usando la reacción de Quellung y PCR. La prueba de sensibilidad se realizó a la penicilina, eritromicina, ceftriaxona, trimetoprim/sulfametoxazol, cloranfenicol, tetraciclina y vancomicina. La tipificación molecular se realizó mediante electroforesis en gel de campos pulsados y análisis de las secuencias multilocus.
ResultadosDe un total de 271 y 350 aislamientos previamente identificados como serotipos 6A y 6B, 61 (22,5%) y 15 (4,3%) fueron reconocidos como 6C y 6D, respectivamente. Los aislamientos presentaron una baja resistencia a los antimicrobianos. Los aislamientos serotipo 6C se asociaron principalmente a los ST9007 (42,6%) y ST9008 (19,7%). El 80% de los aislamientos 6D se asociaron con ST 1135.
ConclusiónEste estudio demostró la circulación del serotipo 6C y 6D en Colombia desde 1994. La información es importante para determinar la dinámica de estos serotipos descritos recientemente.
The polysaccharide capsule of Streptococcus pneumoniae is the main virulence factor, and based on its chemical composition more than 96 serotypes have been described.1 Serogroup 6 has been recognized worldwide as an important cause of invasive pneumococcal disease (IPD); initially it was composed of the serotypes 6A and 6B, but in recent years, additional types as the 6C, 6D, 6E, 6F, 6G and 6H have been reported.2–6
Serotype 6C was described in 2007,2 its capsular loci structure presents a high similitude with the serotype 6A, except the wciNα gene that is substituted in 6C serotype by the wciNβ gene. Therefore, the chemical structures of both serotypes differs; a galactose in the capsular polysaccharide of 6A is replaced for glucose in serotype 6C.7 Since the description of serotype 6C, it has been reported in several surveillance studies as one of the most prevalent serotypes8,9 and its molecular epidemiology has been associated to 6A serotypes.1,10 Serotype 6D, was originally considered an artificial strain created at the laboratory by the insertion of wciNβ gene into a 6B strain.11 However, it was posteriorly found in asymptomatic carriers and in IPD isolates.3,12 Serotype 6D has been mainly reported in Asian countries.12–14
In Colombia, the National Surveillance Network System Program of Bacterial Agents Causing Pneumonias and Meningitis (SIREVA II–PAHO program) has reported nine serotypes between 1994 and 2014: 14 (23.3%), 1 (13.5%), 6B (7.9%), 23F (7.1%), 3 (6.7%), 19F (6.0%), 6A (5.5%), 5 (5.1%) and 19A (4.0%); these serotypes have been located as the cause of 79.5% IPD cases; among these, the proportion of the serotypes 6A/6B was 13.5%.15,16 The aim of this study was to describe the frequency, antimicrobial susceptibility and the molecular characterization of serotypes 6C and 6D among the IPD isolates that have been identified as 6A and 6B.
Materials and methodsFrom January 1994 through December 2013, a total of 621 isolates of S. pneumoniae serogroup 6 were received at the national surveillance program in Colombia (SIREVA II). All isolate samples were cultured from patients with a diagnosis of invasive disease. The serotyping was performed using the Quellung reaction (Staten Serum Institute Denmark). The susceptibility testing was performed by micro-dilution and using Kirby–Bauer methods according to recommendations by the Clinical and Laboratory Standards Institute (CLSI).17 All isolates were tested with penicillin, erythromycin, ceftriaxone, trimethoprim/sulfamethoxazole, chloramphenicol, tetracycline and vancomycin.
Isolates identified as 6A (n=271) were retested by multiplex PCR for the identification of serotype 6C, using primers to detect wciN6C gene in serotype 6C18 and the cpsA (conserved capsular biosynthetic locus).19 The PCR was performed with 100ng of each primer, 2.5mM MgCl2, 0.5mM of each deoxynucleoside triphosphate, 1Unit Taq Polymerase and 5μl of DNA, which was obtained using the boiling method. The cycling PCR conditions were as follows: initial denaturation at 94°C for 5min, followed by 30 cycles of 94°C for 30s, 61°C for 45s and 72°C for 60s, with a final extension at 72°C for 5min. PCR products were resolved on 1.2% agarose gels containing 0.5μg/mL of ethidium bromide. The positive isolates by PCR were confirmed using the Quellung method with the reaction of the factor antiserum 6d (antigenic combination factors 6b−, 6c−, 6d+). In the identification of serotype 6D, 350 isolates recovered in the surveillance and serotyped as 6B were tested by Quellung reaction with the factors antiserum 6c and 6d (antigenic combination factors 6b−, 6c+, 6d+). In the processes, strains serotype 6C and 6D were used as a control, which were donated by the Institute Adolfo Lutz of Brazil and the Centers for Disease Control & Prevention, Atlanta, respectively.
Pulsed-field gel electrophoresis (PFGE) was performed in the total of isolates identified as 6C and 6D. Isolates that exhibited a similarity >75% were considered as a cluster by the unweighted-pair group method with arithmetic means (UPGMA), using the Dice similarity coefficient, an optimization value of 1.5% and tolerance position of 1.0%. The genetic relationship was analyzed among isolates 6C/6D, Spain9VST156, Spain23FST81, Spain6BST90, Colombia23FST338, South Africa6BST185 and the 6A and 6B PFGE patterns published previously.20 From each PFGE cluster one isolate was selected to identify the sequence type (ST) by multilocus sequence typing (MLST).21 The STs were determined using the software available on the MLST (http://pubmlst.org/spneumoniae/).
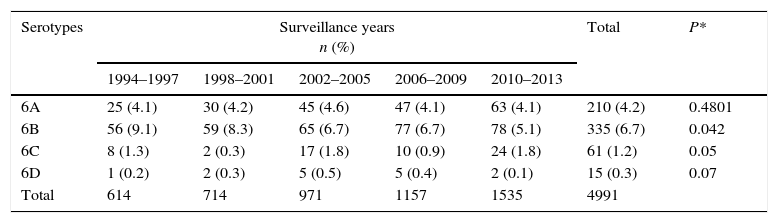
ResultsFrom 1994 to 2013, a total of 4991 isolates of S. pneumoniae as the cause of IPD were collected in Colombia; among all the isolates collection, the serotype 6C had a frequency of 1.2% among all the surveillance isolates (Table 1). The identification of 6C serotype by PCR presented a concordance of 100% with the Quellung reaction.
Frequency of invasive serotypes 6A, 6B, 6C, and 6D isolates from 1994 to 2013 among total serogroup 6 pneumococcal isolates from 1994 to 2013.
| Serotypes | Surveillance years n (%) | Total | P* | ||||
|---|---|---|---|---|---|---|---|
| 1994–1997 | 1998–2001 | 2002–2005 | 2006–2009 | 2010–2013 | |||
| 6A | 25 (4.1) | 30 (4.2) | 45 (4.6) | 47 (4.1) | 63 (4.1) | 210 (4.2) | 0.4801 |
| 6B | 56 (9.1) | 59 (8.3) | 65 (6.7) | 77 (6.7) | 78 (5.1) | 335 (6.7) | 0.042 |
| 6C | 8 (1.3) | 2 (0.3) | 17 (1.8) | 10 (0.9) | 24 (1.8) | 61 (1.2) | 0.05 |
| 6D | 1 (0.2) | 2 (0.3) | 5 (0.5) | 5 (0.4) | 2 (0.1) | 15 (0.3) | 0.07 |
| Total | 614 | 714 | 971 | 1157 | 1535 | 4991 | |
P*: Estimated between 2006–2009 and 2010–2013.
Isolates were recovered from blood (50.8%) (31/61), cerebrospinal fluid (46.0%) (28/61), and other sterile fluids (3.2%) (2/61). Meningitis was the most common diagnosis (46.0%) (28/61), followed by pneumonia (24.5%) (15/61), sepsis (18%) (11/61), and other invasive diseases (11.5%) (7/61).
The serotype 6C isolates were mainly recovered from children <5 years old (37.7%) (23/61) and adults >50 years old (26.2%) (16/61). In the other age groups it presented low proportion (5–14 (9.8%) (6/61) and 15–50 (21.3%) (13/61) years old), and 4.9% (3/61) of patients did not report age data. Only one isolate (3.6%) from a patient with meningitis presented a MIC to penicillin ≥0.125μg/mL. Eight isolates (13.1%) were non-susceptible to trimethoprim/sulfamethoxazole (MIC≥8.0μg/mL), seven (11.5%) were non-susceptible to tetracycline (MIC≥8.0μg/mL), and all isolates presented susceptibility to ceftriaxone, erythromycin, chloramphenicol, and vancomycin.
Among the 350 isolates identified previously as serotype 6B, 15 (4.3%) were typed as 6D. These isolates were recovered from patients with meningitis (8/15) (53.3%), pneumonia (5/15) (33.3%) and sepsis (2/15) (13.3%). The 6D serotype caused IPD in children <5 years old (20%), 5–14 (26.7%), 14–50 (26.7%) and >50 (20%). One patient (6.7%) did not provide age information. The MIC to penicillin ≥0.125μg/mL was observed in one isolate (6.6%). Two isolates (13.3%) were resistant to trimethoprim/sulfamethoxazole (MIC≥8.0μg/mL).
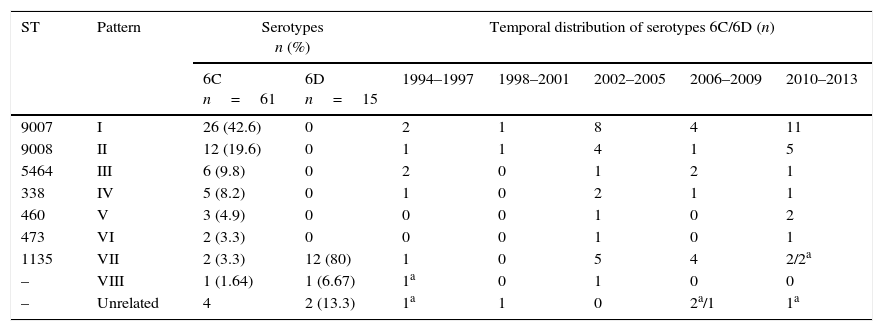
The isolates were grouped in eight clusters by PFGE (Table 2, figure supplementary). The cluster I grouped a total of 26 (42.6%) isolates that presented a relationship with the ST9007 (aroE: 1, gdh: 10, gki: 9, recP: 43, spi: 10, xpt: 1, ddl: 6). The cluster II was formed by 12 (19.7%) isolates associated with the ST9008 (aroE: 10, gdh: 5, gki: 4, recP: 43, spi: 146, xpt: 20, ddl: 28). Both sequences, ST9007 and ST9008, were found and reported for the first time in this study. These sequences presented a high frequency in the last years of surveillance (Table 2). Cluster III grouped 9.8% (6/61) of the isolates, which were related to the ST5464. In Cluster IV, 8.2% (5/61) of the isolates were related to Colombia23FST338 clone. The clusters V and VI associated three and two isolates with ST473 and ST460, respectively. Cluster VII grouped twelve isolates 6D and two 6C that were associated to with ST1135, and identified mainly in 2002–2005 and 2006–2009. In cluster VIII, one isolate 6D was genetically identical to one isolate 6C. Finally, four (6.6%) isolates 6C and two (13.3%) 6D were not genetically related.
Genetic and temporal distribution of S. pneumoniae serotype 6C and 6D isolates.
| ST | Pattern | Serotypes n (%) | Temporal distribution of serotypes 6C/6D (n) | |||||
|---|---|---|---|---|---|---|---|---|
| 6C n=61 | 6D n=15 | 1994–1997 | 1998–2001 | 2002–2005 | 2006–2009 | 2010–2013 | ||
| 9007 | I | 26 (42.6) | 0 | 2 | 1 | 8 | 4 | 11 |
| 9008 | II | 12 (19.6) | 0 | 1 | 1 | 4 | 1 | 5 |
| 5464 | III | 6 (9.8) | 0 | 2 | 0 | 1 | 2 | 1 |
| 338 | IV | 5 (8.2) | 0 | 1 | 0 | 2 | 1 | 1 |
| 460 | V | 3 (4.9) | 0 | 0 | 0 | 1 | 0 | 2 |
| 473 | VI | 2 (3.3) | 0 | 0 | 0 | 1 | 0 | 1 |
| 1135 | VII | 2 (3.3) | 12 (80) | 1 | 0 | 5 | 4 | 2/2a |
| – | VIII | 1 (1.64) | 1 (6.67) | 1a | 0 | 1 | 0 | 0 |
| – | Unrelated | 4 | 2 (13.3) | 1a | 1 | 0 | 2a/1 | 1a |
In this study, serotype 6C isolates were identified in the first year of surveillance (1994), similar to retrospective studies in different countries that showed the presence and circulation, in Denmark, isolates 6C have been reported since 196222 and in the USA have been found since 1989.23 Among the Colombian isolates serotype 6C presented a low frequency. On the contrary, countries such as the USA8 and Spain24 have reported a high frequency of this serotype in IPD. In Latin America, the SIREVA II program that included the participation of 20 countries, has reported the frequency of 6C isolates from 2009 to 2012 as a cause of IPD in countries such as: Brazil (n=54), Mexico (n=17), Colombia (n=17), Chile (n=14), Argentina (n=11), Costa Rica (n=4), Peru (n=3), Uruguay (n=3), Ecuador (n=2), Dominican Republic (n=2), Bolivia (n=1).25
Even though 6C isolates are generally more susceptible to antimicrobials than 6A,26 resistance and multi-drug resistance in 6C has been reported.10 In contrast, a low frequency of 6C resistant isolates was observed in our results. However, continuous the surveillance is important because the increase of resistance could be due to gene replacement events within the capsular loci from isolates non-susceptible to 6A or others serotypes.27
Two new STs, ST9007 and ST9008, were identified in this study, which clustered over half of the isolates, presented a greater circulation in the last years studied, and suggested the occurrence of clonal groups responsible for IPD caused by serotype 6C in Colombia. The ST 9007 presents with only one variant in the spi allele with the ST 2185, which was reported in isolates 6A in Poland, 6C/D in Germany and isolates 6C in Portugal and South Africa. ST9008 is associated with ST10717 by a single variant in the spi allele, which was reported from an isolate serotype 6C in the USA (http://pubmlst.org/spneumoniae/).
A low proportion of isolates were also associated with ST5464 that has been reported in isolates 6C and 6B from carriers in Peru (http://spneumoniae.mlst.net/). Additionally, some 6C isolates were related to Colombia23FST338 clone, which has been associated frequently with isolates serotype 23F, but also with serotypes 19A, 19F, 23A/B.20 The relation of ST338 with isolates serotype 6C was also reported in the USA.8
The isolates also were associated to ST460 and ST473, and both sequences have been related to 6A isolates. In Colombia, the ST473 was previously identified in IPD Colombian serotype 6A isolates.20,27 ST460 has been more associated with serotype 6A,23 and less with 6C isolates.28 The ST473 associated with 6C isolates has been reported in USA,8,18,23 Spain24 and Australia.29 Additionally, ST473 was found in isolates serotype 6D in Australia.28
Serotype 6D has been reported as a cause of IPD mainly in Asian countries12,14 and in a low proportion in Australia,29 Europe30 and Israel.31 In Latin America, he first report of this serotype was done from carriers in Peru.32 Additionally, Cuba reported one isolate 6D from IPD within the SIREVA II–PAHO program.25 We determined that this serotype has been circulating since the beginning of the surveillance in a low frequency, and almost all the isolates were associated with ST1135, which has been reported in association with serotype 6B isolates (www.mlst.net).
In Colombia, the PCV7 was included in the Plan of Immunization in 2009 for children of 2 years of age from some regions in the country. Subsequently, PCV7 was switched to PCV10 in 2010, and extended to the whole country.33,34 During this study, only the serotype 6B had a decrease significant. However, this analysis could be affected by the time after PCVs introduction, and by the collection of isolates, which was done from many regions of the country with a different coverage of the vaccination.
In conclusion, this study shows that serotypes 6C and 6D have been circulated in Colombia since the surveillance was started. Even though the number of isolates found was low, a continuous surveillance is necessary to determine the impact of pneumococcal vaccines’ introduction on these serotypes. The detection of pneumococcal 6C serotypes by a PCR had a complete concordance with the Quellung reaction; it offers a substantial cost savings in comparison to the conventional antiserum. Additionally, the serotype 6C genetic structure was associated with switching capsular events among the serotypes of serogroup 6 and Colombian23F ST338 clone, a fact that potentially could lead to the increase of IPD rates caused for this serotype by expansion of capsular variants of international clones.
Conflict of interestThe authors declare no conflict of interest.
We acknowledge Elizabeth Castañeda (PhD and Emeritus Researcher, Instituto Nacional de Salud, Bogotá, Colombia) for her critical review to the manuscript. We also thank Dr. María Cristina Brandileone at the Institute Adolfo Lutz of Brazil by the Portugal6AST327 clone and serotype 6C strains, which were used in the PFGE and PCR controls. We also are grateful Dr. Carvahalo at the Centers for Disease Control & Prevention, Atlanta, by the isolate 6D, was used as a control in the quellung reaction. Also, we want to express our gratitude to Diana Diaz and Viviana Ramos by their technical support in the molecular methodology.
The following are the supplementary data to this article:
