




As of 30 April 2020, 203.715 SARS-CoV-2 infections had been reported in Spain, 54.486 in Madrid, 21.4% were health care workers. Our objective is to determine seroprevalence of COVID-19 among workers in a monographic pediatric hospital.
MethodsBetween April13th and 30th, 1.523 health workers were recruited to be tested for SARS-CoV-2 serology screening (All Test®) and they answered a questionnaire with demographic, epidemiological and clinical information and previous exposure to COVID-19.
FindingsOne thousand two hundred ninety two (84.8%) were tested. Positive serology (IgM and/or IgG) to SARS-CoV-2 was found in 17.2% (222/1.292), in 15.5% (201/1.292) if only IgG was considered. Median age was 44±13 years, 73% were female. The 33.8% (75/222) were asymptomatic. Eighty one had a previous positive rRT-PCR. The 14% (32/222) referred a family contact.
ConclusionSerology prevalence for SARS-CoV-2 in workers of a pediatric hospital was higher than in general population. Many of them had an unnoticed infection.
A 30 de abril de 2020, se habían notificado 203.715 infecciones SARS-CoV-2 en España, 54.486 en Madrid, y el 21,4% eran trabajadores de la salud. El objetivo del estudio es determinar la prevalencia serológica de infección SARS-CoV-2 en trabajadores de un hospital monográfico pediátrico.
MétodoDel 13 al 30 de abril, 1.523 trabajadores fueron convocados a realizar un test serológico (All Test®) frente a SARS-CoV-2 y respondieron un cuestionario con información demográfica, clínico-epidemiológica y de exposición a COVID-19.
ResultadosMil doscientos noventa y dos (84,8%) fueron estudiados. La prevalencia serológica (IgM y/o IgG+) a SARS-CoV-2 fue del 17,2% (222/1.292) y del 15,5% (201/1.292) considerando IgG positiva. La edad media fue 44 ± 13 años, el 73% eran mujeres. El 33,8% (75/222) fueron asintomáticos. Tenían rRT-PCR positiva previa 81. El 14% (32/222) contacto familiar.
ConclusiónLa prevalencia serológica SARS-CoV-2 en los trabajadores de un hospital pediátrico fue mayor que en la población general. Muchos pasaron una infección inadvertida.
The first case of COVID-19 in Madrid was recorded on 25 February 2020. As of 30 April, 203,715 cases had been reported (Red Nacional de Vigilancia Epidemiológica [Spanish National Epidemiological Surveillance Network] [RENAVE]); 58,486 of those cases were in Madrid. Of them, 21.4% corresponded to healthcare workers.1
The prevalence of SARS-CoV-2 infection in the generation population is around 5%-11%.2 Spain has more infected healthcare workers than any other country in the world, with significant variations in seroprevalence in studies conducted at general hospitals.3–8 The serological prevalence in individuals under 19 years of age is 1%-4%.9 Infections in Madrid in spring 2020 peaked on 26 March, with 3,364 cases.10
The procedure of choice for the diagnosis of acute SARS-CoV-2 infection is real-time reverse transcription–polymerase chain reaction (rRT-PCR) testing on a nasopharyngeal swab. Rapid, simple, highly sensitive and accurate tests must be available for purposes of large-scale identification of people who recovered from the infection or had subclinical infection.11–13 Serological tests detect IgM and IgG antibodies against SARS-CoV-2 in blood, serum or plasma, and aid in understanding the epidemiology thereof and the role of asymptomatic carriers.8,14,15 This is especially important in healthcare and community health workers.
The objective of this study was to determine the prevalence of SARS-CoV-2 infection in professionals at a specialised paediatric hospital since, as it had fewer infected patients, higher levels of community exposure could be assumed.
MethodsThis cross-sectional, descriptive study was conducted in workers at Hospital Infantil Universitario Niño Jesús [Niño Jesús University Children's Hospital] (Madrid), a specialised hospital with 180 beds.
In March and April 2020, 52 patients under 18 years of age with a positive PCR test for SARS-CoV-2 were admitted.
The hospital had 1,523 workers, 1,197 of whom were women (78%). All were offered serological testing between 13 and 30 April 2020 and invited to complete a survey. Workers on occupational leave and workers who did not undergo serological testing were excluded.
The variables analysed in seropositive workers were: age, sex, chronic diseases, tobacco use, symptoms (low-grade fever or fever, cough, sore throat, difficulty breathing, ageusia, anosmia, muscle pain, headache, asthenia, chills, etc.), date of onset of symptoms and contact with confirmed or possible cases of COVID-19. The results of prior rRT-PCR tests were collected.
A rapid immunochromatographic assay in venous blood (All Test® 2019-nCoV IgG/IgM rapid lateral flow immunoassay) was used due to its availability and ease of use. At that time, enzyme-linked immunosorbent assay (ELISA) was not yet commercially available.
Ethical considerationsThe study was approved by the hospital's independent ethics committee.
Statistical analysisAge, the sole quantitative variable, was reported in terms of median and interquartile range. For qualitative variables, percentages and corresponding 95% confidence intervals were calculated. Qualitative variables were compared using the chi-squared (χ2) test. A difference was determined to be statistically significant with a p value of 0.05.
ResultsOf the workers, 84.3% (1,292/1,523) had the test done. The prevalence of positive (IgM and/or IgG) serology for SARS-CoV-2 was 17.2% (95% CI: 15.16%-19.35%). The results listed below relate to this group of seropositive workers:
- •
The median age was 46 (range: 20-68) years; 74% were women. Among healthcare workers, (75%), 27% (60) were auxiliary staff, 19% (43) were physicians and 19% (42) were nurses. Among non-healthcare workers, the largest percentage of those who tested positive were administrative staff, with 10.9% (24), followed by cleaning staff, with 6.3% (14). The date of onset of symptoms was reported as 16 March by 40% of workers.
- •
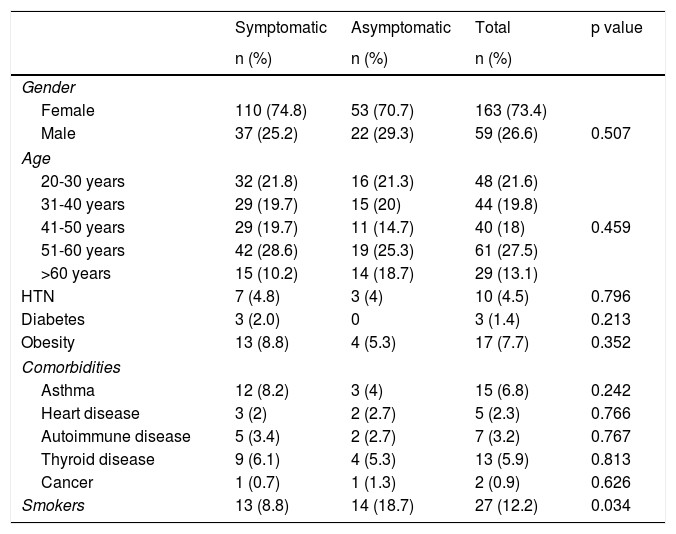
The most common symptoms were respiratory symptoms (50%), fever or low-grade fever (34%), ageusia and/or anosmia (38.7%), general symptoms (30%), and gastrointestinal symptoms (26%). Asymptomatic cases accounted for 33.8% of the total. There were no significant differences in rates of asymptomatic patients by age group or gender. Overall, 12% were smokers. Smoking was reported by 18.7% of the asymptomatic workers versus 8.8% of the symptomatic workers (p < 0.05) (Table 1).
Table 1.Epidemiological characteristics of workers with positive serology.
Symptomatic Asymptomatic Total p value n (%) n (%) n (%) Gender Female 110 (74.8) 53 (70.7) 163 (73.4) Male 37 (25.2) 22 (29.3) 59 (26.6) 0.507 Age 20-30 years 32 (21.8) 16 (21.3) 48 (21.6) 31-40 years 29 (19.7) 15 (20) 44 (19.8) 41-50 years 29 (19.7) 11 (14.7) 40 (18) 0.459 51-60 years 42 (28.6) 19 (25.3) 61 (27.5) >60 years 15 (10.2) 14 (18.7) 29 (13.1) HTN 7 (4.8) 3 (4) 10 (4.5) 0.796 Diabetes 3 (2.0) 0 3 (1.4) 0.213 Obesity 13 (8.8) 4 (5.3) 17 (7.7) 0.352 Comorbidities Asthma 12 (8.2) 3 (4) 15 (6.8) 0.242 Heart disease 3 (2) 2 (2.7) 5 (2.3) 0.766 Autoimmune disease 5 (3.4) 2 (2.7) 7 (3.2) 0.767 Thyroid disease 9 (6.1) 4 (5.3) 13 (5.9) 0.813 Cancer 1 (0.7) 1 (1.3) 2 (0.9) 0.626 Smokers 13 (8.8) 14 (18.7) 27 (12.2) 0.034 HTN: hypertension; n: number of hospital workers.
- •
The largest share of seropositive individuals worked in a general hospitalisation area (19.8%), followed by oncology (14.9%) and intensive care (8.6%). In 32 (14.3%) workers, there was prior contact with a family member.
- •
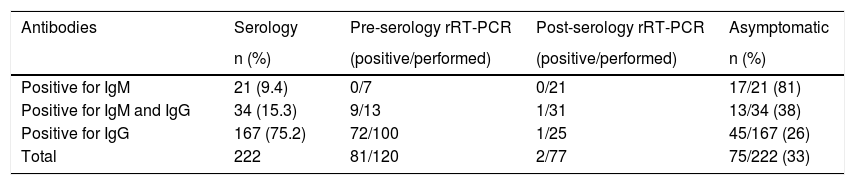
Table 2 shows the results of serology and rRT-PCR testing and the numbers of asymptomatic professionals.
Table 2.Results of serology and rRT-PCR testing and numbers of asymptomatic professionals.
Antibodies Serology Pre-serology rRT-PCR Post-serology rRT-PCR Asymptomatic n (%) (positive/performed) (positive/performed) n (%) Positive for IgM 21 (9.4) 0/7 0/21 17/21 (81) Positive for IgM and IgG 34 (15.3) 9/13 1/31 13/34 (38) Positive for IgG 167 (75.2) 72/100 1/25 45/167 (26) Total 222 81/120 2/77 75/222 (33) n: number of hospital workers; rRT-PCR: real-time reverse transcription–polymerase chain reaction.
- •
For those with positive results for IgM, subsequent rRT-PCR tests were ordered for confirmation of infection; all of them came back negative.
Given that numbers of patients admitted to a specialised paediatric hospital were much lower than numbers of adult patients admitted to hospital, this study is important as its results can be compared to those of other studies at other centres prioritising COVID-19 care.6
The prevalence of SARS-CoV-2 infection in the workers (17%) was higher than in the general Spanish population (5%) and in the population of Madrid (11%).2 Not counting cases positive for IgM and considering only those positive for IgG, the prevalence would come down to 15.5%.
According to our results, the reliability of diagnosis with a positive result for IgM is limited, since rRT-PCR for confirmation purposes came back negative in all cases, and most workers with a positive result for IgM (80.9%) were asymptomatic. This suggests that the test is very sensitive but not very specific, and points to the possibility that those positive results were false positives.
It is important to note that more than one in four workers were asymptomatic.
This higher prevalence could be explained by the fact that the workers continued working and remained exposed to SARS-CoV-2 outside of their homes. It is unknown whether the environment in which transmission most commonly occurred was the community, the home or the hospital, or, within this, whether transmission could have occurred through contact with patients, relatives and/or co-workers. The fact that, during the first two months, just 52 COVID-19 patients were admitted to our hospital makes it more likely that the sources of nosocomial transmission were workers themselves. This was all the more likely considering that 33% of them recovered from the infection following an asymptomatic course and many recovered following a course with few symptoms. However, it is also important to consider that the largest numbers of positive cases occurred in the areas with the highest numbers of COVID-19 patients (hospitalisation, oncology and intensive care).
It is essential to establish a preventive strategy, through active pursuit of rRT-PCR testing of infected professionals, either systematically (e.g. at specific time intervals) or when a cluster of cases is detected in an area of work and/or in workers who have a higher risk of exposure or care for vulnerable patients. Serology testing is essential in estimating levels of exposure and identifying higher-risk areas.6,12,16 The peak of symptom onset occurred in parallel to the peak of community infections; therefore, this strategy would be most useful at the height of epidemic transmission.10
The limitations of this study included its analysis of a sample of workers with positive serology results and the self-administered nature of the survey, meaning that some questions may not have been correctly interpreted. The study also lacked reliable information on the nature of the contact between workers and patients suspected of transmission and on the personal protective measures used in each case. The serology technique selected can influence the results.17 Immunochromatography can serve as a screening method to determine seroprevalence in the population.18,19 It is more sensitive in serum or plasma than in capillary blood. ELISA shows better diagnostic sensitivity, and therefore now prevails.20,21
FundingThis study received no specific funding from public, private or non-profit organisations.
Conflicts of interestThe authors declare that they have no conflicts of interest.
We would like to thank all the workers who completed the survey; the laboratory staff who did a great deal of work in a short period of time; hospital management for acquiring the test; Dr Mercedes Alonso, the head of the microbiology unit; and Dr M. Teresa García, an occupational medicine physician, for helping with the study reported in this article.
Please cite this article as: Escribano Ceruelo E, Espinel Ruíz MA, Ortega López-Peláez M, Fernández Garoz B, Asensio Antón J, Jiménez García R. Seroprevalencia de infección frente a SARS-CoV-2 en trabajadores de la salud en un hospital monográfico pediátrico en Madrid (España). Enferm Infecc Microbiol Clin. 2022;40:326–329.
