






Information is one of the most important needs of families of critical patients. Healthcare professionals also identify the great value of communication with families to reduce their anxiety and stress. Despite this, families may feel inadequately informed, causing added suffering. The purpose of this study is to provide an understanding of both families’ and healthcare professionals’ perspectives on information giving within intensive care units (ICU).
MethodA narrative review was conducted using MEDLINE, CINAHL, PsycINFO databases and the Cochrane Library to identify studies published in either English or Spanish from 2002 to 2018.
Results47 studies were included, and five categories were identified: 1) “The need to know”, 2) Family satisfaction with the information received, 3) Impact of information on families’ experiences in the ICU, 4) Nurses and physicians’ perceptions of information transmission, and 5) Information process in the ICU.
ConclusionsProviding honest and truthful information to the families of critical patients is essential to reduce family anxiety and increase family control, although this often appears to be inadequately accomplished by staff. Interdisciplinary involvement in information giving may be beneficial for both families and ICU professionals. This review brings new understanding about the process of information to families of ICU patients and it can be used to improve the quality and humanization of care in the ICUs.
La información es una de las necesidades más importantes de los familiares de pacientes críticos. Los profesionales sanitarios identifican también el gran valor de la comunicación con los familiares, para reducir su ansiedad y estrés. A pesar de ello, los familiares pueden sentirse indebidamente informados, lo cual causa un sufrimiento añadido. El objetivo de este estudio es tratar de comprender las perspectivas de los familiares y los profesionales sanitarios sobre la información que se aporta en las unidades de cuidados intensivos (UCI).
MétodoSe realizó una revisión narrativa utilizando las bases de datos MEDLINE, CINAHL, PsycINFO y Cochrane Library para identificar los estudios publicados en inglés y español de 2002 a 2018.
ResultadosSe incluyeron 46 estudios, identificándose cinco categorías: 1) «Necesidad de saber»; 2) «Satisfacción del familiar con la información recibida»; 3) «Impacto de la información en las experiencias de los familiares en la UCI»; 4) «Percepciones de las enfermeras y medicos sobre la transmisión de información», y 5) «Proceso de información en la UCI».
ConclusionesLa aportación de información honesta y veraz a los familiares de los pacientes críticos es esencial para reducir su ansiedad e incrementar su control, aunque parece que esto no siempre es adecuadamente realizado por el personal. La implicación interdisciplinaria en la aportación de información puede ser beneficiosa para los familiares y los profesionales de las UCI. Esta revisión aporta una nueva comprensión acerca del proceso de información a los familiares de los pacientes de UCI, y puede utilizarse para mejorar la calidad y humanización de los cuidados en dichas unidades.
Intensive care units (ICUs) are highly technical settings.1 Due to the instability of the patient in critical condition, ICU personnel provide immediate and specialised care to respond to the physiological needs of the patient; however, they sometimes forget the fact that they are a part of a more complex family unit.2 In addition, patients in the ICU often cannot understand the information, or make important decisions, due to the seriousness of their illness. Even when the patients are full conscious of their conditions, some leave decision making in the hands of their family members.3,4 For that reason, so as to provide overall, holistic care in the ICU, healthcare professionals must involve the patients’ families, as a component of the therapy.5,6 In fact, many international organisations, such as the Joint Commission on the Accreditation of Healthcare Organizations, the American Nurses Association and the Society of Critical Care Medicine, support how important the care given by the families in the ICU setting is.7
Some authors argue that being admitted to the ICU negatively affects the whole family system and that it can cause social and psychological disorders in the family members, who can need specialised attention.5,8 Throughout the last few decades, the needs of the families of patients in the ICU’s have been debated and classified into 5 areas: safety, information, proximity, support and comfort,9 with information identified as one of the families’ most important needs.4,9–12 Family members of patients in critical condition very often experience feelings such as stress, anxiety, depression, fear, anguish and uncertainty because the families do not know what is happening and what the future will bring. The ICU can change quickly, even from hour to hour, so the family members need continual, progressive information.7 However, although receiving information is one of the main needs of the families of patients in the ICU, healthcare professionals often forget this needs. Some of the reasons may be that the relationship between nurses and families mainly focuses on technical procedures:1 the ICU staff and the families perceive the patients’ needs in different ways,1,5,13 and the nurses underestimate their role in giving information to the families.4,5,10
However, the evidence shows that the nurse/patient/family member relationship helps the professionals every day in decision making, and that the families consider it to be an essential element of patient care.3,13,14 Providing information also has a positive impact on the satisfaction of the dual patient/family unit.15 In spite of the great number of reviews that explore the needs of the families of patients in the ICU, to the best of our knowledge, none of them has focused on understanding information giving from the families’ and the healthcare professionals’ perspectives. Consequently, there is a need for further research into the process of giving information to the families in ICU settings, so as to identify the strategies that can satisfy the needs of the families of patients in critical condition. For that reason, the objective of this review was to provide an understanding of information giving to the families of patients in the ICU.
In this article, the family members of patients in the ICU are considered individuals with whom the healthcare professionals establish therapeutic relationships in order to share information about the health of the patient who is their relative.16 As used in this manuscript, the action of information giving refers to a key aspect of the communication between the healthcare professionals and the families. Information giving is not just the action of informing; it is also that of building a therapeutic relationship and an association with the patients and their families.17
Materials and methodsA narrative review was carried out so as to be able to include studies with different designs and to provide a wide, critical and objective analysis of current knowledge about the issue under study.18–20
Search strategyFour databases were searched for references: MEDLINE, CINAHL, PsycINFO and Cochrane Library, including all the primary studies and reviews published in English or in Spanish between January 2002 and December 2018. The criteria for inclusion and exclusion for this review were also identified (Table 1).
Selection criteria.
| Criteria for inclusion | Criteria for exclusion |
|---|---|
| • Studies and reviews related to the process of giving information to the families of patients in the ICU | • Publications related to families of paediatric patients in the ICU |
| • Studies and reviews related to the perceptions of families and professionals about giving information in the ICUs | • Information related to giving families information, in which nurses are not involved |
| • Terminal care in the ICU | |
| • Grey literature |
The search terms used were «information», «family», «nursing» and «critical care». These terms and their synonyms were combined using the Boolean operators AND and OR. In addition to using the «snowball» technique, specialised literature was searched manually. The specific journals searched were related to family nursing (Journal of Family Nursing) and to critical care nursing (American Journal of Critical Care, Critical Care Nursing, Critical Care Nursing Quarterly, Current Opinion in Critical Care, Dimensions of Critical Care Nursing, Intensive Critical Care Nursing, Journal of Critical Nursing and Nursing in Critical Care).
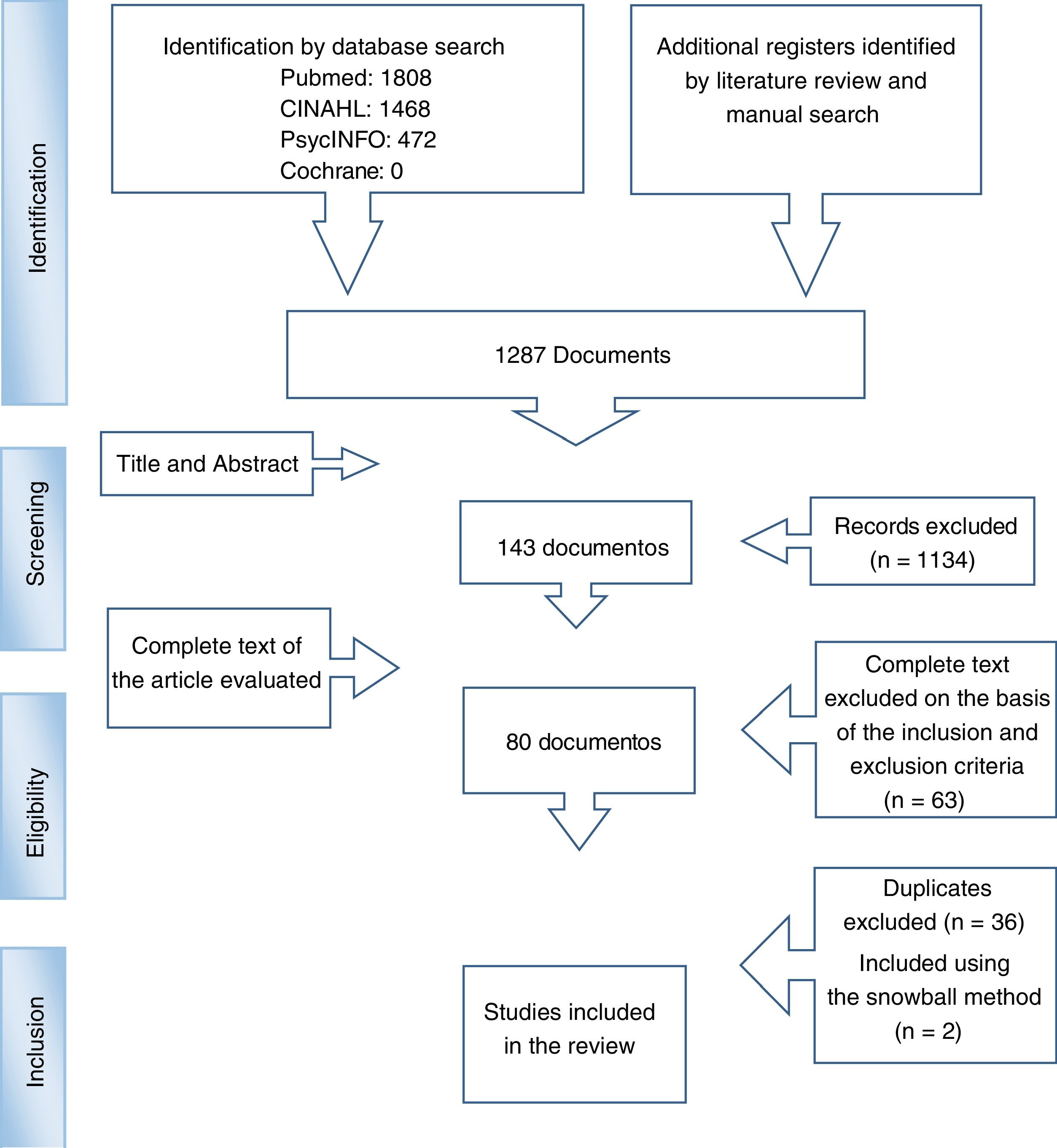
Process of selectionIn the first stage, all the records identified were reviewed and, after eliminating duplicates, their titles and abstracts were read. In the second stage, the complete text of the articles screened was evaluated for eligibility, excluding the articles that did not comply with the inclusion criteria. In the end, 46 articles were included in this review (Fig. 1).

The selection and initial review of the articles were carried out by the main author of this article. When doubts arose as to the eligibility of an article, the second author was asked to help to review that article. Finally, the two authors would agree on final article inclusion.
Extraction and data analysisThe documents gathered that complied with the inclusion criteria were analysed and recurrent issues were identified. The thematic analysis was used as the analytical framework for this review, for reaching better understanding of the information provided to the family members in the setting of the ICU.20,21 Our process spanned 3 stages: initial coding of the findings from the studies included; organising the codes into categories; and developing the main categories and their corresponding subcategories. To strengthen the rigour of this review, the data, codes and categories were developed and then discussed and accepted by the 2 authors.
ResultsThis review covers 46 studies selected and included (Table 2). The data were classified into 5 categories: 1) «Need to know»; 2) «Family member’s satisfaction with the information received»; 3) «Impact of the information on the families’ experiences in the ICU»; 4) «Nurses’ and physicians’ perceptions of the transmission of information», y 5) «Information giving in the ICU».
Studies included in the review.
| Author(s) (year) | Study objective(s) | Design | Data gathering method | Sample/sampling | Main results | Country |
|---|---|---|---|---|---|---|
| Al-Hassan and Hweidi (2004) | Identify the needs of Jordan families with a relative admitted to the ICU | Quantitative Descriptive cross-sectional study | CCFNI questionnaire | 158 family members (18−72 h following patient admission). | Information is one of the most important needs | Jordan |
| Convenience sampling | ||||||
| Al-Mutair et al. (2013) | Identify the perceived needs of the families of patients in the ICU | Qualitative Descriptive exploratory study | Interviews | 12 family members of patients admitted to medical-surgical or traumatological ICUs | Information is one of the most important needs. Knowing the situation reduces anxiety. Ample, honest information | Saudi Arabia |
| Auerbach et al. (2005) | Evaluate the satisfaction of the family members with respect to need fulfilment | Quantitative Descriptive study | CCFNI questionnaire | 40 family members of patients admitted to traumatological ICUs | Satisfaction is related to the information provided | USA |
| Azoulay et al. (2002) | Evaluate the effectiveness of the information given to families of patients in the ICU | Random trial | Intervention | 87 family members received an information leaflet for family members and standard information, and 88 did not receive it | The information leaflet for family members provided general information, the name of the physician in the ICU in charge of the patient, a drawing of a typical ICU room with the names of all the devices, and a glossary of 12 terms commonly used in the ICU. It was linked to good understanding and improved satisfaction | France |
| Bailey et al. (2010) | Describe the perceptions of the family members as to information, anxiety and satisfaction | Quantitative Descriptive cross-sectional study | CCFNI, STAI and Androfact™ questionnaires | 30 family members of patients admitted for at least 24 h. | Ample, honest information. | Canada |
| Convenience sampling | Connection between information and satisfaction with the attention. Lack of connection between information and anxiety level | |||||
| Bond et al. (2003) | Ascertain the needs of the family of patients with severe head injury | Qualitative Descriptive exploratory study | Interviews | 7 family members of patients with severe head injury admitted for more than 24 h. | The most common phrase was the need to know. The family members reported a lack of information from the physician. Incoherence in the information provided by the various staff members | USA |
| Convenience sampling | ||||||
| Browning et al. (2006) | Identify and explore the needs that the family members considered covered. | Quantitative | NMI questionnaire | 30 family members of patients on respiratory support (24−36 h after patient admission). | The family members are not satisfied with the information | USA |
| Descriptive exploratory study | Convenience sampling. | |||||
| Chien et al. (2006) | Evaluate the effect of an educational programme for critical patients based on the value assigned to their needs | Quasi-experimental | Intervention and C-CCFNI and C-STAI questionnaires | 66 family members (34 in the experimental group and 32 in the control group). | Information is one of the most important needs. Information reduces the family members’ anxiety and increases their satisfaction | China |
| Convenience sampling | ||||||
| Daly et al. (2010) | Implement a wide system of communication and test regular, structured meetings about the results of long-stay patients in the ICU | Clinical trial | Intervention | Control group (135 patients): standard communication | There are no statistically significant differences between the two groups as far as the hospital stay and costs | USA |
| Intervention group (346 patients) | ||||||
| Davidson et al. (2010) | Evaluate an support intervention for the family members of patients on respiratory support | Quantitative | Intervention and CCFNI questionnaire | 30 family members of patients on respiratory support. | Information is one of the most important needs for the family members involved. The intervention was very useful for the families | USA |
| Intervention | Convenience sampling | |||||
| Engström and Söderberg (2004) | Describe the experiences of the family members of patients in the ICU | Qualitative | Interviews | 7 family members (1 male and 6 females) of patients on respiratory support. Convenience sampling | The most difficult thing: the wait for information. | Sweden |
| Descriptive interpretive study | Direct, honest information, even when it is negative. | |||||
| They feel more reassured if they can phone the ICU. If they do not understand the information, they ask the nurse | ||||||
| Engström and Söderberg (2007) | Describe the nurses’ experiences with family members in the ICU | Qualitative | Discussion group | 24 ICU nurses | They value honest, consistent information. | Sweden |
| The family members can blame them when there is not enough information | ||||||
| Gaeeni et al. (2015) | Explain the perspectives of family members of patients in the ICU and of the nurses with respect to informative support | Qualitative | Semi-structured interviews | 19 family members/nurses | Provide information: receive news about the admission, complete and truthful information, and general information. | Iran |
| Content-focused analysis | Handling the information: keep them informed and gradual revelation. | |||||
| Use of the information: support for the patient and for the family members | ||||||
| Hinkle et al. (2011) | Compare the perceptions on the needs of the family members and staff (physicians and nurses). Search for any need not yet described in the CCFNI | Quantitative | CCFNI questionnaire and item commentaries | 101 family members of patients admitted for at least 24 h. | Information is one of the most important of the families’ needs. Staff underestimate the families’ need for information | USA |
| Descriptive prospective study | 109 nurses. | |||||
| 28 physicians. | ||||||
| Convenience sampling | ||||||
| Hughes et al. (2004) | Quantify the contribution of information to the family members in ICUs chapels, analysing the information available and the governmental policies about ICUs | Quantitative | Analysis of ICU policies with respect to the families | 119 hospitals | Informative leaflets better than the recommended level. 16% of the ICUs do not reach the Health Department recommendations. | GB |
| Descriptive study | Relative variability of the quality and amount of information to which the patients have access | |||||
| Hughes et al. (2005) | Examine the experiences of the family members and the way in which the staff perceive them | Qualitative | Semi-structured interviews | 8 family members of patients suddenly admitted to the ICU and 5 nurses | Type of information requested. | GB |
| Well-founded theory | Type of information provided. | |||||
| Importance of the information | ||||||
| Khalaila (2012) | Investigate the importance and the needs covered perceived by family members of patients in the ICU and evaluate the families’ satisfaction with the needs covered | Quantitative | CCFNI and FS-ICU questionnaires | 70 family members of critical patients that had received respiratory support in a medical ICU for more than 48 h. | Satisfaction with the attention was positively associated with the needs for meeting, except for the need for information | Israel |
| Cross-sectional study | Convenience sampling | |||||
| Karlsson et al. (2011) | Quantify the satisfaction of family members of critical patients | Quantitative Descriptive retrospective study | CCFSS questionnaire and two open questions | 35 family members of 35 patients that had been discharged from the ICU 48 h before | The family members think that they have received little medical information. They emphasise feelings of uncertainty. | Sweden |
| Open questions: they emphasise the importance of knowing what is happening at all times | ||||||
| Keenan and Joseph (2010) | Identify the needs of the family members of patients with severe head injury | Qualitative | Semi-structured interviews | 25 family members of 15 patients (44 interviews in 2 sessions). Purposive sampling | Most family members expressed the need for information. Coherent, understandable, honest and updated information. | Canada |
| Part of a mixed method study | Specific information about their family member, not about statistics | |||||
| Lee and Lau (2003) | Examine the immediate needs of the family members in the ICUs | Quantitative | C-CCFNI questionnaire | 40 family members (24−72 h after patient admission). | The need for information is one of the most important, and one of the last to be fulfilled | China |
| Descriptive cross-sectional study | Convenience sampling | |||||
| Llamas-Sánchez et al. (2009) | Establish the needs of the family members of patients in the ICU. | Quantitative | Survey initiated in the references. Validity not mentioned | 268 family members of patients admitted at least 48 h before. | Information is one of the most important needs. The information provided by the nurses is understood better. Statistically significant differences between breadth of the information and satisfaction | Spain |
| Establish the satisfaction with the information provided | Cross-sectional observational study | Random systematic sampling | ||||
| Maxwell et al. (2007) | Compare perceptions of the family members and nurses about the needs | Quantitative | CCFNI and NMI questionnaires and two open questions | 50 individuals (30 nurses and 20 family members), at least 24 h after ICU admission. Convenience sampling | Information is one of the families’ most important needs. | USA |
| Descriptive exploratory study | Differences with respect to the importance of the information. | |||||
| Differences as to the perception of the satisfaction provided by the information | ||||||
| McKiernan et al. (2010) | Describe the experiences of the family members in the ICUs | Qualitative | Interviews | 6 family members. | Everyone expressed the need to know. The family members associated the information with the way of coping with the experience. The nurses provided most of the information requested. Ample, accurate and honest information. The professionals believe that the family members understand the information, but that is not so | Ireland |
| Phenomenological study | Purposive sampling | |||||
| Nelms et al. (2010) | Explain the core experiences of family members of patients with critical illness, and their implications in family nursing | Qualitative | Semi-structured interviews | 11 relatives (41 family members) of patients on respiratory support during the hospital stay | Nurse-family interaction: one of the main ways in which the families search for information. The family members feel uncertainty due to: results, patient status, doubts about the decisions and medical treatments, unexpected episodes, and ambiguous information. | USA |
| Analysis of secondary data | Essential: Ample, honest and accurate information | |||||
| Omari (2009) | Identify the needs of the family members of patients in the ICU. | Quantitative | CCFNI and NMI questionnaires | 139 family members of 85 patients (24−48 h after admission). Convenience sampling | Information is found among the most important needs that are not adequately handled | Jordan |
| Explore whether these needs have been covered | Descriptive exploratory study | |||||
| Paul and Rattray (2008) | Identify the short- and long-term impact of critical illness on family members of patients. Identify the needs of the family members, their experiences and interventions, to cover them | Literature review | MEDLINE, British Nursing Index and Archive, EMBASE, CINAHL, PsycINFO and Cochrane | Review of publications from 1950 to 2007 limited to English. Studies on family members of critical patients were included | Information: one of the most important needs. | GB |
| Narrative review | Admission: Communication affects how the needs are covered. Non-covered needs: lack of information about medical equipment, procedures and patient status | |||||
| Plakas et al. (2009) | Examine the experiences of family members of critical patients | Qualitative | Interviews, participatory and non-participatory observation (from 2002 to 2005) | 25 family members | The frequency, quality and breadth of information are important. | Greece |
| Well-founded theory | Information effects the emotions negatively or positively. Spending more time with the patient increases the opportunities of obtaining information | |||||
| Prachar et al. (2010) | Identify the needs of family members in the neuro-ICU | Quantitative | CCFNI questionnaire | 111 family members of patients admitted at least 24 h (78 emergency admissions and 30 elective). | The same needs are important for both groups, in relation to the information. The family members valued the information from the nurses more highly that that from the physicians | USA |
| Descriptive prospective study | Convenience sampling | |||||
| Santana Cabrera et al. (2007) | Compare the satisfaction of family members of patients in the ICU from the staff’s point of view | Quantitative | Survey of relative satisfaction. Same interview modified for professionals | 52 family members of patients admitted at least 24 h before. | Family members are satisfied with the information. | Spain |
| Descriptive prospective study | 69 professionals (58 nurses and 11 physicians). Random ICU staff sampling | The staff underestimated how appropriately this need is handled | ||||
| Santana-Cabrera et al. (2009) | Analyse the nurses’ perceptions of the quality of the process of communication with family members of patients in the ICU | Quantitative | NACF survey | 70 nurses | Generalised lack of nurse activity with respect to communication with the family members | Spain |
| Descriptive cross-sectional study | ||||||
| Shaw et al. (2014) | Evaluate an educational programme to improve clinical trust in the communication techniques and the families’ satisfaction by the ICU team | Quantitative | Supplier satisfaction survey and FS-ICU questionnaire | 46 caregivers in multidisciplinary teams and 121 family members of patients in the ICU | The ICU team improved their confidence in the communication with the family members of critical patients; the satisfaction of the family members with the communication also improved | USA |
| Pre-post intervention | ||||||
| Shelton et al. (2010) | Examine the impact on the ICU team, the satisfaction of the family members, the hospital stay and the healthcare costs of incorporating a full-time coordinator | Quasi-experimental | Intervention and FSS questionnaire | Stage I: 190 patients. | The intervention was linked to greater family member satisfaction with respect to the communication with each member of the team | USA |
| Stage II: 187 patients | ||||||
| Söderström et al. (2006) | Describe and interpret the interactions between the family members and the staff in the ICU | Qualitative | Observations and interviews | 10 family members | 2 groups: mutual understanding and lack of mutual understanding | Sweden |
| Stayt (2009) | Examine the nurses’ emotional role in care for the family members of critical patients | Qualitative | Non-structured interviews | 12 nurses. | They describe the information as an essential aspect of care for the family members. Honest and accurate information versus hope. Bad news is the physician’s responsibility | GB |
| Phenomenological study | Purposive sampling | |||||
| Sundararajan et al. (2012) | Determine the level of satisfaction with the care received. | Quantitative | Satisfaction survey | 84 family members of patients hospitalised in ICU for at least 48 h. The patients had already been discharged. Convenience sampling | High score: communication with the nursing staff (courtesy, respect and compassion). | Australia |
| Identify the aspects related to satisfaction | Prospective observational study | Low score: communication less frequent with the physicians | ||||
| Takman and Severinsson (2004) | Describe and compare the different opinions of physicians and nurses about the needs in the ICUs | Quantitative | CCFNI questionnaire | 605 (nurses: 526; physicians: 79) | Differences in perception between physicians and nurses about the information | Norway |
| Descriptive correlational study | Convenience sampling | |||||
| Takman and Severinsson (2005) | Discover and compare the physicians’ and nurses’ perceptions about the needs in the ICUs | Quantitative | CCFNI questionnaire | 311 professionals (275 nurses and 36 physicians). | Women scored the information higher. Better scores received by physicians with similar experiences with family members in the past | Norway |
| Descriptive exploratory study | Non-probabilistic sampling | |||||
| Torrents Ros et al. (2003) | Discover the level of satisfaction and the information that the family members have after a personalised welcome | Quantitative | The questionnaire was created during the study. Validity is not discussed | 70 family members. | The level of satisfaction was high after applying the protocol | Spain |
| Descriptive prospective observational study | Convenience sampling | |||||
| Vandall-Walker et al. (2007) | Outline the process of nursing support for the families of critical adults from the family members’ perspectives (Western Canadian Teaching Context) | Qualitative | In-depth interviews and notes | 20 family members (27 interviews). | The nurses were authorised to talk with the family members, but some of them never did. | Canada |
| Convenience sampling | The family members looked for information to the nurses first, because they were more accessible | |||||
| Vandall-Walker and Clark (2011) | Determine what the families’ «work» was in coping with the critical illness of a relative, from their perspective | Qualitative | In-depth interviews | 20 family members (27 interviews) in Study I, and 13 family members (15 interviews) in Study II | The information helped the family members to reduce uncertainty, make decisions and gain trust | Canada |
| Velasco Bueno et al. (2018) | Compile an inventory of petitions for information prioritised by the family members | Qualitative | Structured interviews and descriptive cross-sectional study | Families, physicians and nurses of critical patients | The most important questions for the family members were their concern about the clinical situation, the measures to adopt, the prognosis and the information. The physicians and nurses were able to respond to the majority of the questions | Spain |
| Quantitative | ||||||
| Verhaeghe et al. (2005) | Organise the scientific knowledge available about the experiences and needs of the family members of patients in coma in the ICU | Bibliographic review | MEDLINE, PsycINFO and CINAHL | 46 records in English from 1970 to 2004 | Information as a universal need, very important for the family, and not always covered. | Belgium |
| Broad, accurate information that leaves margin for the family members to hope. Personnel capable of covering the needs for information. Information is a need that affects the fulfilment of other needs. The nurses underestimate their role in information giving | ||||||
| Verhaeghe et al. (2007) | Evaluate la relationship between the families’ hope and the information provided by the staff members | Quantitative | 24 in-depth interviews (from 2001 to 2005) | 22 family members of 16 patients in coma. Theoretical sampling | The family members want truthful information given in an understandable way, leaving margin for hope. They require different types of information, depending on the stage of the illness through which the patient is going | Belgium |
| Well-founded theory | ||||||
| Wetzig and Mitchell (2017) | Ascertain the needs of family members of patients in the ICU for adult trauma | Comprehensive review | CINAHL, EmBase, Medline, PsycINFO and PubMed | 16 publications | Information, making sense, support, hope, involvement and protection were the main themes. | Australia |
| The family members identified the need for information as something essential. Consistency, honesty and understanding are essential features of the information | ||||||
| Wong et al. (2015) | Examine the experiences of the family members of critical patients as to their interactions with the personnel and with the setting when their relative is admitted to ICU | Qualitative | In-depth interviews (2009−2011). Well-founded theory | 12 family members | The interactions experienced by the family members of critical patients were mostly about communication: obtaining information, the language of communication, communication of support and communication without support | Australia |
| Well-founded theory | ||||||
| Zaforteza et al. (2005) | Study the relationships that nurses establish with the family members of critical patients, especially with respect to the process of giving the families information | Qualitative | Observations and in-depth interviews | 14 nurse/family relationships observed. | The nurses state that information reduces the families’ fears, but they consider that they should be careful when giving it to the family members, because conflicts can arise with the physicians | Spain |
| Exploratory study | 6 interviews. Purposive sampling |
Getting information appeared, in most of the studies, as one of the most important needs for the families of patients in critical condition.4,10,22–25 Likewise, the «need to know» was one of the phrases most often repeated in the studies included with respect to the experiences of the family members of patients in the ICU.22,26–30 The families’ need for information was recurrent, regardless of the pathology, prognosis or result of the patients.26–31 Age, sex, educational level, cultural level and whether the admission to ICU was unexpected or planned were factors that had no effect on the family members’ experiences with respect to the need for information.10,23,25,32–34
Satisfaction of the families con the information receivedOn evaluating the satisfaction of the needs of the families, they stated that their need to be informed was not always satisfied.8,25,28,33,35,36 In practice, the ICU staff can take this for granted.1,5,25,28 Even though the families considered receiving information from the physicians on a daily basis to be important,8,32,33,35,37,38 this aspect was one of the least satisfied.8,10,26,28,37
On the other hand, the most positive communicative interchanges were those carried out by the nurses.3,10,30,33,37,38 The family members confirmed that when they did not understand the medical information well, they attempted to clear up their doubts by asking the nurses.27,31,38 The families stated that the nurses were more accessible and friendly.4,30,38 Some authors3,33 attributed the families’ positive appreciation of their interaction with the nurses to the amount of time that the nurses spent with the patients and family members, which contributed to a closer relationship.
Impact of information on the experiences of the families of patients in the ICUInformation helped to reduce the uncertainty felt by the family members.25,27,29,31,39–41 It also reduced the families’ confusion, which in turn helped the families to handle the situation that they were going through better.27,30,41 Facing up to the experience calmed their own worries,28 facilitating decision making.10,37 One of the most difficult aspects for the families of patients in the ICU was having to wait for the information to be updated, as well as their uncertainty about the patient’s condition and prognosis.25,27
The uncertainty caused by the lack of information produced feelings of desperation and loss of control, and made the family members feel vulnerable.31 To relieve these sensations, the families looked for further information, approaching the physicians, nurses and other professionals in the ICU hallways, making interminable phone calls, or simply trying to guess the possible meaning of the staff’s expressions and reactions.10,14,25,40
In contrast, the families experienced less anxiety10,14,25,37 and greater satisfaction12,23,37 when they were given understandable and honest information. Providing clear and sincere information increased the families’ trust in the health professionals; this, in turn, favoured positive interactions between the family members and the ICU staff.29 In addition, the family members that were capable of understanding explicit and implicit messages showed personal satisfaction.42 However, when the families did not receive or did not understand the information, they felt confused and perceived a sensation of being abandoned by the ICU staff.14,42 Likewise, confusion arose when the information given by different staff members was contradictory.23
Nurses and physicians’ perceptions of the transmission of informationIn many cases, the physicians and nurses underestimated the families’ need to be informed, compared with their expectations.4,10,35,43 When the physicians’ about the information were compared, it was found that the nurses evaluated the families’ «need to know» as greater than the physicians did.44 A higher score for the information process was also found among female staff members, or when a staff member had experienced a similar situation in his/her own family.45 In general terms, the nurses considered that the information was important to the family members.1,28,46
In some circumstances, the nurses did not reveal the information voluntarily because they did not know what to say, or they did not even feel involved in the information process.28 Some of the nurses felt that the task of giving information corresponded to the physicians.1,28 In addition, the nurses tended to avoid situations in which they might be forced to provide contradictory information, thus creating a conflict, especially when it came to communicating bad news.10,46–48 Likewise, the nurses could simply give «no risk» information to keep from giving false hope to the family members.1,46
Another aspect with which the nurses agreed was the fact that some family members could be «controlling» when they requested information about the patient in the ICU; they could «put the nurses to test» and compare the answers that they obtained from other staff members.28,48 The nurses could also feel overwhelmed when families blamed them for the lack of information.48
However, the nurses considered themselves to be responsible for identifying the families’ need for information.45 The evaluation of the needs of the family members seemed to be related to the nurse’s empathy and professional experience. The nurses that showed the most empathy were more sensitive in providing the families with information, feeling dissatisfied when they did not have enough time to offer further information, due to distractions such as visiting hours or work overload.9 As for the level of experience, there were several different opinions. While Paul and Rattray23 found that the most skilled nurses attributed less value to the need of the family members’ need for information, Takman and Severinsson44 indicated that the skilled nurses were more attentive to satisfying the families’ needs for information. Chien et al.37 argued that the reason for a non-proactive attitude about information giving was that the nurses tended to generalise the need for information and often did not make an individualised evaluation to identify the type of information that the families required with respect to the patient’s situation and the family’s experience.
Process of information giving in the ICUWhat type of information? Who gives it?The families of critical patients stated that they wanted to receive information, firstly from the physician and, in second place, from the nurse. The families also indicated that the information giving process should be initiated by the ICU personnel10 and that they thought that most of the information could be provided by physicians and nurses.4 Specifically, the family members tended to the physician for accurate information about the patient’s condition, treatment, prognosis and diagnostic tests.4,27–29 They expected the nurses to provide information about the patient’s daily care, and about the reasons for choosing specific treatments; they also asked about the ICU setting and its equipment; about the different disciplines involved in the patient’s care; and about what the family members could do for the patient when he/she was discharged.10 The families also asked for specific individualised information, not only information based on statistics and probabilities about the patients’ healthcare results.29
As for the professionals involved in the information giving process, increased satisfaction was found between the families and professionals when those in charge of evaluating and backing the family members’ need for information were the advanced clinical practice nurses,7,49–51 who also acted as a liaison between the family and the medical team.51
However, both families and nurses considered it important to have the same source of information whenever possible.28 If that did not happen, inconsistencies and contradictions might be caused, generating confusion and distrust.10,26,28,39
A last point is that Shaw et al.49 emphasised the importance of multidisciplinary training in communication to improve the satisfaction of the families and the ICU personnel.
How and when to inform?The information given to the family members of the patients in ICU has to be honest and the most accurate possible, to be given in an understandable manner that simultaneously leaves margin for hope.10,12,14,23,25–32,35–37,40,41,43,52–54 Not everyone agreed with this last point, and many families preferred honesty, even when it could pose a threat to their hope.10,25–27,39 Some families associated realistic hope with complete, accurate and true information. False expectations were based on incomplete or incorrect information that could bring about a lack of trust and loss of control of the situation.54 However, the families expressed the importance of receiving information given in a thoughtful manner.39
The family members also felt assured when they could call the staff at any time to request information.27,39 They also appreciated receiving phone calls at home to keep them updated about any changes in the patient’s condition,10,33 or if the patient was going to be discharged from the ICU, in order to be able to choose to be there to accompany her/him.28
Written information in the form of leaflets about the policies, rules, equipment and terms used in the ICU was widely recommended, given that it helped the family members to accept the great amount of information that they were given at the time of admission and improved their understanding of it. The leaflet also improved family satisfaction and extended an invitation to talk with the ICU caregivers.24,28,37,55–57
Torrents et al.56 indicated that the families felt more satisfied when the nurse in charge of the patient received them according to protocol and provided them with an informative guide. The families said that not only the information that they were given was important, but that the way that the information was transmitted and the friendliness with which they were given it were also important.31
Structured information not only satisfied the needs of the family members, it also reduced the workload of the nurses, because it reduced the number of questions and phone calls that the nurses received from the family.50 As for the proper moment, communication with the personnel in the ICU was essential during the first hours after admission to the unit. The family members needed to receive explanations about the setting and the medical team,14,23 and about why certain procedures were being done and about the patient’s condition.23 It might be necessary to repeat this information several times, because the families’ initial state of shock would prevent them from assimilating it.30,54 Keenan and Joseph29 emphasised the fact that the intense «need to know» during the first few days after the patient was admitted to the ICU evolved over time towards coherent information related to the prognosis and long-term quality of life.
The families of the patients in the ICU from sudden circumstances required different types of information over the various stages of the process that they were undergoing.54 In addition, as the patients’ stay extended, the families could want to talk about the possibility that their relative would die, or about negative feelings.22,37,58
On a daily basis, updated information made it easier for the families to accept what was happening; and it also helped them to understand the seriousness of the patient’s condition, even once the critical period had been surmounted.10,35,36
DiscussionThe findings from this review emphasise the universal nature and importance of information giving for the families of patients in critical condition. However, healthcare professionals seem to have a different perception, given that providing individualised information does not appear to be a priority for them. In fact, several authors highlighted the importance of personalised, regular and progressive evaluation of the families’ need for information,2,36 which could help to develop an optimum information giving process. This would also help the families to cope, to the greatest extent possible, with the turmoil that they suffer during their family member’s admission to the ICU.
This review also emphasises the nurses’ feelings about their involvement in the information giving process, given that they consider giving information to be an important task. However, they give priority to the physician’s role. In contrast, family members state that the information provided by the physicians is important for them, but the information given by the nurses is also important, and that nurses are more accessible and friendly.10,33,39 The evidence reflects the significant role that nurses play when it comes to communicating with the families of patients in ICUs. Nurses constitute an immediate source of information, because they are in constant contact with the patients and family members and the nurses help them to interpret information from the physicians.8,35,39,42
For these reasons, systematic and multidisciplinary treatment of information, which covers all the patient-related issues, is essential to promote the wellbeing of the families. However, this would not be possible with the appropriate communication and collaboration of the ICU team,54,58,59 for preventing inconsistencies, contradictions and incorrect interpretations. This fact reflects the need for work teams for the ICUs.1,4,47,48 In addition, meetings or conversations with the ICU team (a physician in change, backed up by a nurse) also appear to be effective ways of strengthening communication with family members.39
Lastly, the findings of this review support the fact that providing honest, accurate and understandable information is essential for a satisfactory information giving process.14,23,25,27,29–32,35–37,40,41,43,52 Providing such information reduces anxiety among the families of patients in critical condition. Leske60 argues that family members suffering from anxiety are often incapable of offering support to their family members who are ill, possibly transmitting their anxiety to the patient in the end. This anxiousness can also take the form of a lack of trust in the personnel, dissatisfaction with patient healthcare, and even lawsuits. It is therefore essential to train the personnel in specialised services, such as emergency services or the ICUs, to handle the families’ emotional needs and their need for information.4,61
LimitationsAs we have mentioned before, it is worthwhile emphasising the impossibility of finding enough studies that handle in depth the issue of information giving to the families of patients in the ICU, despite the fact that it is a universal need. Many studies are based on the general experiences or needs of the families. In addition, only 12 of the 46 studies included in this review specifically mentioned information giving.1,10,12,14,22,39,42,49,50,54,56,62 Likewise, many articles were essentially descriptive or explicative, and although several recommendations were found in the literature, there was no evidence about the most appropriate methods for giving information to the families.25
As for gathering information, the questionnaire used most often in many cases was the Critical Care Family Needs Inventory (CCFNI),63 which has been validated for and adapted to multiple contexts. It is not a specific questionnaire to evaluate information, and this fact should be remembered when interpreting the results. In addition, information giving was conceptualised in certain studies as a social dimension of family support,32 defining reassurance as foreseeing the families’ need to know the results and to feel that there is hope.6 In general, information giving is considered an integral component of emotional support.64 Some studies have used the aspects of support and information from the CCFNI questionnaire together to investigate the information.9 Due to the fact that the main objective of our review was to understand the process of the information given to families with a relative in critical condition, when results from the studies included were extracted, we included certain aspects related to other needs of the family members, such as support and assurance.
ConclusionThis review provides a wide general view of the information giving process provided in the ICUs from the perspectives of the families and of the healthcare professionals working in such units.
For the families of the patients in the ICU, information is a high priority need that is not always properly covered by the professional staff. Honest, ample information increases the satisfaction of the family members and reduces their anxiety, which has a positive effect on the patient. Providing adequate information to the families does not seem a high priority for the nurses and physicians. At any rate, the information giving process produces relationships of trust between the family and the professionals, and impacts the way in which other needs, such as emotional support and assurance, are handled.
Consequently, individualised, regular and progressive evaluation, together with appropriate communication and collaboration with ICU personnel, can help the families to benefit from quality information giving. Implementing a systematic process for the information given in the ICU may prevent the families from suffering, reduce their anxiety and improve the satisfaction of patients and families with the healthcare given. A family-oriented focus requires the professionals to change their attitudes, skills and training, as well as calling for a commitment to place the patient and the family members as the centre of attention.
It is hoped that this review has provided clarity about and offered guidelines for informative support for the families of patients in the ICU. Professionals and managers are also invited to use this review to improve the quality and humanisation of healthcare in the ICUs.
FundingThe authors have not received any type of funding related to the research and/or authorship of this article.
Conflict of interestsThe authors have no conflicts of interest related to the authorship and/or publication of this article to declare.
We would like to thank Martín Aoiz sincerely for help in translating this article.
Please cite this article as: Regaira-Martínez E, Garcia-Vivar C. El proceso de información a los familiares en las unidades de cuidados intensivos: una revisión narrativa. Enferm Intensiva. 2020. https://doi.org/10.1016/j.enfi.2019.11.004

