




We have read a study by López Fernández et al.1 reporting the case of a woman with a history of hypertension, diabetes type 2 and a hospital admission, 2 years earlier, due to pneumonia and hyponatraemia. The woman visited the emergency department due to abdominal pain, vomiting and diarrhoea and showed signs of dehydration. During her stay, she had a seizure that led to a coma. She had serious hyponatraemia (101mmol/l), plasma hypo-osmolarity and normal potassium and renal function. She did not have metabolic acidosis (MA). After her hyponatraemia had been corrected, she underwent a colonoscopy, which showed a polyp with a villous appearance in the hepatic flexure of the colon. This, following laparoscopic right hemicolectomy, turned out to be villous adenoma with a moderately differentiated adenocarcinoma.
All of the above is consistent, in the authors’ opinion, with McKittrick–Wheelock syndrome. This term was coined in 1954 to describe an entity characterised by a villous adenoma of the rectum with chronic secretory diarrhoea that may cause dehydration, hypokalaemia, hyponatraemia and acute renal failure.2
A review of the literature in English on the matter, through an article by Malik et al.,3 yielded 35 cases with no sex predominance. Virtually all patients had acute renal failure (91%), hyponatraemia (96.3%) and hypokalaemia (95.6%).
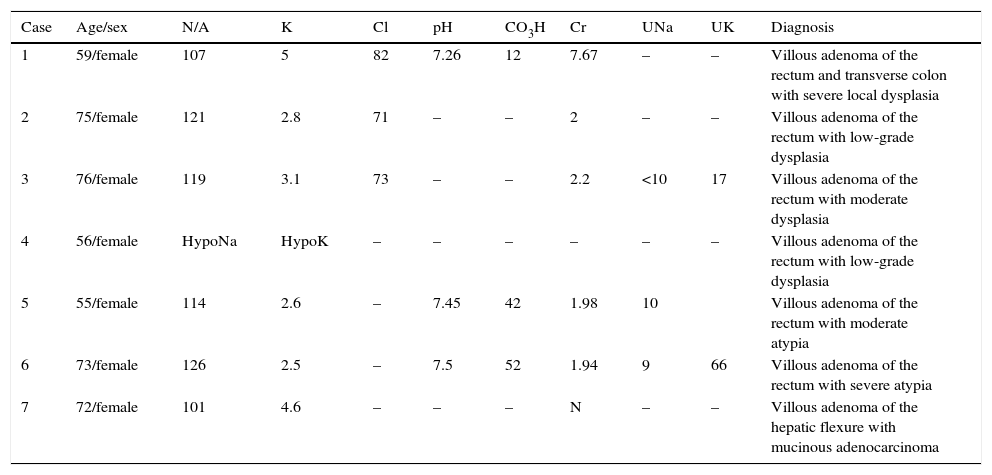
We also studied the 7 cases that we found in Spanish, including the one that motivated this letter (Table 1).4–8 All were women with hyponatraemia; 5 (71.4%) had hypokalaemia and, of the 3 cases with the relevant data, one had MA and the other 2 had metabolic alkalosis. Just one patient had normal renal function, and natriuresis was low in the 3 cases in which this information was available. This revealed a decrease in effective circulating volume. The case in question is striking due to the patient's normal renal function and potassium; the omission of data, whose absence complicates a proper diagnosis; and the very location of the villous adenoma (the vast majority of the lesions that lead to this syndrome are distal, which prevents compensatory absorption in the distal colon). Thus, while we do not intend to question the diagnosis made, we wish to note that it would have been important to know information such as the treatment that the patient was receiving at the time of admission; the cause of her hyponatraemia during her previous stay; her sodium levels in the interval between her 2 admissions; her natriuresis levels during her current admission; her TSH and cortisol levels; and, finally, her natraemia levels subsequent to her recovery.
Patient characteristics.
| Case | Age/sex | N/A | K | Cl | pH | CO3H | Cr | UNa | UK | Diagnosis |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 59/female | 107 | 5 | 82 | 7.26 | 12 | 7.67 | – | – | Villous adenoma of the rectum and transverse colon with severe local dysplasia |
| 2 | 75/female | 121 | 2.8 | 71 | – | – | 2 | – | – | Villous adenoma of the rectum with low-grade dysplasia |
| 3 | 76/female | 119 | 3.1 | 73 | – | – | 2.2 | <10 | 17 | Villous adenoma of the rectum with moderate dysplasia |
| 4 | 56/female | HypoNa | HypoK | – | – | – | – | – | – | Villous adenoma of the rectum with low-grade dysplasia |
| 5 | 55/female | 114 | 2.6 | – | 7.45 | 42 | 1.98 | 10 | Villous adenoma of the rectum with moderate atypia | |
| 6 | 73/female | 126 | 2.5 | – | 7.5 | 52 | 1.94 | 9 | 66 | Villous adenoma of the rectum with severe atypia |
| 7 | 72/female | 101 | 4.6 | – | – | – | N | – | – | Villous adenoma of the hepatic flexure with mucinous adenocarcinoma |
Cl: chlorine; CO3H: bicarbonate; Cr: creatinine; HypoNa: hyponatraemia; HypoK: hypokalaemia; K: potassium; UK: urinary potassium; Na: sodium; UNa: urinary sodium; pH: potential of hydrogen.
Only with awareness of this information could it have been possible to make the diagnosis defended with due rigour and, at the same time, rule out other possibilities such as improper secretion of antidiuretic hormone, with which the patient's reduction in extracellular volume would have conflicted a priori.
Notwithstanding this, we would like to congratulate the authors on the interesting nature of the case and the contributions of their study.
Please cite this article as: Prieto de Paula JM, Rodríguez Martín C, Martín Asenjo M, Franco Hidalgo S. Puntualizaciones sobre un caso de síndrome de Mckittrick-Wheelock y coma metabólico. Gastroenterol Hepatol. 2017;40:430–431.
