










This study investigates peripersonal space (PPS) modulation in patients with anorexia nervosa (AN) versus healthy controls (HCs) and explores associations between PPS, eating-related, and general psychopathology.
MethodForty-six patients and 42 HCs completed a computer-based task observing videos of an approaching actor (male or female) displaying different facial expressions along with a non-social condition. Then, participants completed self-report questionnaires assessing eating-related and general psychopathology.
ResultsMixed-models revealed that both groups adjusted PPS based on task conditions, with a gender effect favoring closer proximity to female actor. HCs reduced PPS amplitude progressively during the task, while patients did not show this effect. In patients, wider PPS correlated with lower self-esteem and facial expression identification accuracy, while in HCs, PPS was associated to body dissatisfaction and anxiety symptoms.
ConclusionThese findings enhance understanding of bodily self-consciousness, suggesting PPS consideration in therapeutic interactions with patients with AN and as a potential target in treatments addressing social impairment.
Anorexia Nervosa (AN) is a mental disorder in which - besides the specific symptoms linked to eating and the body - other determinants related to comorbidity, personality traits, emotion regulation, and socio-relational factors have a significant role (Jérolon et al., 2022; Monteleone & Cascino, 2021). In different theoretical models, socio-relational factors are central in the development and maintenance of the disorder. Arcelus and colleagues underlined how some social interaction factors determine greater social sensitivity which in turn influences self-esteem and social anxiety (Arcelus et al., 2013). In the “cognitive interpersonal model” by Treasure and Schmidt (2013), the social components were relevant in all phases of risk and development of the disease and were divided into predisposing, precipitating, and maintenance factors (Treasure & Schmidt, 2013). Subjects suffering from AN have inabilities in social functioning and social processing (Mason et al., 2021), high levels of social shame (Panero et al., 2022), and difficulties in friendship and relationships (Datta et al., 2021); these problems often precede the onset of the disorder (Cardi et al., 2018). Two meta-analyses estimated a greater risk of social anxiety symptoms in subjects with AN compared to healthy controls (Kerr-Gaffney et al., 2018) and a correlation between physical social anxiety (i.e., fear of being observed or negatively judged basing on physical aspect) and body image disturbance (Alcaraz-ibáñez et al., 2023). Relatedly, it has been known that the co-morbidity between AN and social anxiety disorder is high, varying from 16 to 88.2 % (Swinbourne & Touyz, 2007).
In AN, the study of social components is difficult since it involves biological, psychological, and cultural levels, often tenaciously intertwined with each other. A possible way of studying social behaviors is to evaluate how individuals modulate space and mutual distances during social interactions. This area of research originated in anthropology with the pioneering studies of Hall who called the study of gestures, space, and distances within social communication “proxemics”, and identified four possible distances: intimate, personal, social, and public (Hall, 1966).
Proxemics had applications in the clinical field (Kendall et al., 1976; Mclaughlin et al., 2008). Its study has recently been resumed with the development of neuroscience and the possible clinical applications of virtual reality (McCall, 2017) and with the definition of the more restrictive and measurable concept of peripersonal space.
Peripersonal Space (PPS) is the space around the body in which we interact with other people and objects (Rizzolatti et al., 1997). The term PPS was used by Rizzolatti and colleagues who identified a group of neurons triggering when an object was present inside the PPS (Rizzolatti et al., 1981). Subsequently, neurosciences deepened the nature and the functions of PPS. Two main functions emerged: a motor one regarding the interaction with objects in the surroundings (Brozzoli et al., 2012), and a defense function to protect the body from incoming threats, regarding both human and non-human entities (de Haan et al., 2016). Overall, PPS is relevantly involved in the social environment since it represents the space in which the interactions with others occur (Rabellino et al., 2020). Concerning the nature of PPS, it was described as flexible and, under normal circumstances, the modulation of its boundaries depends on the nature of external stimuli (e.g., valence, context) and internal factors (e.g., bodily state). PPS is thus regulated by the balance between subject's affective states and implicit and explicit cognitive responses (Biggio et al., 2019).
The concept of PPS is related to bodily self-consciousness. Bodily self-consciousness refers to the subjective experience and perception of the body including physical sensation, movement, and spatial boundaries; relatedly, bodily self-consciousness is influenced by the perception of the space around the body (Rabellino et al., 2020).
A core symptom of AN is the body image disturbance: patients with AN have an altered experience of their body, especially in terms of a distorted perception of body shape and weight (Dalhoff et al., 2019; Sattler et al., 2020). This impairment is not limited to the aesthetic component of the body: studies are demonstrating that the bodily impairment is much deeper, involving implicit components of the bodily self-consciousness. Literature described alterations in patients with AN in the sense of agency (Colle et al., 2023), body schema (Meregalli et al., 2023), and the processing of tactile information (Gadsby, 2017). All these alterations contribute to an experience of the body as extraneous (Stanghellini et al., 2012) and out of control; this is often exacerbated by somatoform dissociation and body dissatisfaction (Longo et al., 2022).
The exploration of PPS is interestingly applied to the study of psychopathology. Herein, alterations of PPS were described in anxiety disorders (Iachini et al., 2015), post-traumatic stress disorder (Rabellino et al., 2020), autism spectrum disorders (Mul et al., 2019), and schizophrenia (Di Cosmo et al., 2018). Just two studies addressed PPS in AN (Nandrino et al., 2017; Cartaud et al., 2024). The first study adopted the stop-distance paradigm (i.e., a typical task to evaluate PPS) with videos recorded on human actors and found larger PPS boundaries in patients than in healthy participants. Interestingly, the larger the PPS the higher the scores on scales measuring eating-related symptoms (Nandrino et al., 2017). Cartaud et al. (2024) used virtual characters and static tasks such as the reachability judgment and the interpersonal distance judgment task. The authors reported, in contrast to the previous data by the same group, no differences in interpersonal distance between patients with AN and HCs, and showed that both groups kept at a higher distance the virtual characters with angry expressions than those with happy expressions (Cartaud et al., 2024).
The cited studies, however, had limitations. The samples were not large; in the first study (Nandrino et al., 2017) only three experimental conditions were studied and the possible moderators of the PPS were investigated only with bivariate analyses; in the second study (Cartaud et al., 2024) the evaluation of the interpersonal space was conducted with virtual characters (i.e., avatar) in virtual reality and the participants were asked to choose their preferred relational distance through an experimental adjustment of the position of the avatar. The evaluation was therefore static and concerning the use of conscious cognitive functions (i.e., judgment). This study, however, has the merit of considering many aspects that could influence the choice of interpersonal distance as our study did, but it did not address the effect of approaching stimuli's gender on PPS. The gender of the approaching person is a relevant factor: studies on healthy subjects showed that the distance chosen to interact with female subjects is shorter than that preferred to interact with males (Iachini et al., 2015; Ruggiero et al., 2017); in contrast, Nandrino et al. (2017) found that patients with AN kept at higher distance the female than the male actor: the paucity of data on this variable in AN led us to deepen the topic. Moreover, facial expressions are typically relevant in determining PPS boundaries: previous studies on healthy participants tested the effect of neutral, negative (e.g., angry), and positive (e.g., happy) facial expressions on the choice of comfortable interpersonal distance, finding an increase of distance when the approaching actor displayed a negative facial expression (Cartaud et al., 2018; Ruggiero et al., 2017). Similarly, in the recent study by Cartaud et al. (2024), patients with AN chose greater relational distance when the virtual character simulated angry expressions. To our knowledge, the effect of facial expression on PPS in AN was not extensively addressed in a dynamic way with human approaching actors, and this is a relevant gap since it was showed an impairment in the recognition of others mental states in the active phase of the illness (Preti et al., 2022), especially for negative emotions (Martini, Marzola et al., 2023). Relatedly, our interest focused also on verifying the influence of correct facial expressions recognition on the choice of interpersonal distance; this relationship was not investigated so far despite the above-cited difficulty in emotion recognition typical of patients with AN. Furthermore, no studies explored the role of the gaze direction of the approaching individual in determining the choice of comfortable distance: this variable could be specifically important for patients with AN given their tendency to avoid looking at faces and eyes in social tasks (Watson et al., 2010). Moreover, although many studies addressed the change in eating-related symptoms after the pandemic (J. Devoe et al., 2023; Martini, Longo et al., 2023), no one investigated the role of wearing mask in modulating social distance in patients with AN. Lastly, it was not explored whether the experiment modifies the PPS and subjective emotional states through the task. It is also noteworthy, that in real-world social interactions, all the cited factors are entangled influencing each other, thus the interactions among these variables (e.g., gender, facial expressions) may be investigated. Relatedly, the use of dynamic tasks with human actors is essential because it has a higher ecological validity and allows to evaluate more accurately the factors linked to PPS determined by implicit rather than conscious mechanisms.
Given limited data on PPS in AN and the limits of previous research, we deepened the exploration of PPS in AN with the following aims: a) to compare patients with AN and HCs on the modulation of PPS in different conditions (i.e., interaction with an object and social interaction with male and female actors with different facial expressions, namely, neutral, with laterally directed gaze, threatening, friendly, and wearing an FFP2 mask); b) to assess whether the PPS modulation changes over time measuring the differences in mean PPS among the blocks of the task; c) to investigate the association between PPS and psychometric measures of eating-related and general symptoms (i.e., anxiety, depression, dissociation, self-esteem) and the accuracy in the recognition of actors’ facial expressions conveying emotions.
We expect a larger PPS in patients than in HCs, and different patterns of PPS modulation in the two groups. In particular, for patients with AN, given the literature cited above, we hypothesize a larger distance in the interaction with females than males, following Nandrino et al. (2017), a shorter distance in the conditions in which the actor turned the gaze laterally and wore an FFP2 mask, and a higher difficulty in recognize the emotional facial expressions of the actors compared to HCs, speculating an effect of this alteration on PPS modulation. As regards HC, we expect to replicate the findings on the non-clinical population on the higher comfort of interacting with female than male subjects, and the influence of negative and positive emotion-related facial expressions on the modulation of PPS. Moreover, we assume both subjects with AN and HCs to become familiar with the task, shortening the distance to the actors over time and reaching a greater state of comfort after the task. Lastly, we hypothesize a positive correlation between the width of PPS and the severity of psychopathology in both patients with AN and HCs.
Method and materialsParticipantsThe study included 46 patients with AN (23 with R-AN, 14 with BP-AN, and 9 with atypical AN): 95.7 % of patients were female (n = 44), while 2 patients (4.3 %) were male. We recruited 42 HCs, of which 40 were females (95.2 %) and 2 were males (4.8 %). Patients were recruited at our center. All patients met the criteria for AN diagnosis according to DSM-5, except for 9 of them who met all criteria but maintained their weight within or above the normal range. We set the following inclusion criteria: a) diagnosis of AN or atypical AN; b) age greater than 18; c) normal or corrected-to-normal eyesight. Exclusion criteria were: a) comorbid psychotic disorder; b) current alcohol or substance abuse; c) cognitive impairment and neurological disease.
HCs were recruited among university students and medicine residents. For them, inclusion criteria were age greater than 18 and normal or corrected-to-normal eyesight; exclusion criteria were: a) current or history of psychiatric disorder; b) current alcohol or substance abuse; c) cognitive impairment and neurological disease.
All participants signed the informed consent according to our Ethical Committee that approved this study under the registration number CS2/1125.
Procedure and materialsClinical assessmentAll participants were interviewed by an experienced psychiatrist who confirmed or excluded the diagnosis of AN and checked for inclusion and exclusion criteria. Both patients and HCs completed the following self-report questionnaires during the first week after the visit:
Eating Disorder Examination Questionnaire (EDE-Q; Fairburn & Beglin, 1994): is one of the most used questionnaires to evaluate eating-related psychopathology. It investigates four clusters of eating-related symptoms: dietary restraint, food concern, weight concern, shape concern. We used the Italian validation that has a Cronbach's alpha value of 0.95 (Calugi et al., 2017); Cronbach alpha for our sample had a value of 0.95.
Eating Disorder Inventory 2 (EDI-2; (Garner et al., 1983a): it assesses the core symptoms of eating disorders providing the following subscales: drive for thinness, bulimia, and body dissatisfaction; moreover, other symptoms typically reported by subjects with eating disorders are explored such as perfectionism, interoceptive awareness, and maturity fears. The tool has a good internal consistency (Cronbach's alpha = 0.95; (Garner et al., 1983b). Cronbach alpha in our sample was 0.93.
Beck Depression Inventory (BDI; (Beck et al., 1961): it describes the severity of depressive symptoms with items about affective, cognitive, and physical symptoms. The internal consistency is high (Cronbach's alpha 0.86; (Wang & Gorenstein, 2013); in our sample, Cronbach alpha measured 0.90.
State-Trait Anxiety Inventory (STAI; (C. D. Spielberger et al., 1983): it assesses anxiety differentiating between a current and context-related anxiety (i.e., state anxiety) and a stable and personality-typical anxiety (i.e., trait anxiety). The Cronbach's alpha value of 0.96 reflects a good internal consistency (C. Spielberger, 2010). In our sample, Cronbach alpha value was 0.75.
Body Shape Questionnaire (BSQ; (Cooper et al., 1987): it aims to estimate how individuals perceive their body image and to assess the level of body dissatisfaction. The Italian validation has a high internal consistency (Cronbach's alpha = 0.97; (Marzola et al., 2022), while Cronbach's alpha calculated on our sample had a value of 0.98.
Rosenberg Self-Esteem Scale (Rosenberg, 1965): it evaluates self-esteem in terms of the perception of one's own value and self-acceptance. The Cronbach's alpha of 0.81 reflects a high internal consistency (Sinclair et al., 2010), even in our sample, with a value of 0.87.
Dissociative Experience Scale (DES II; (Carlson & Putnam, 1993): it investigates the frequency of dissociative experiences perceived by individuals in daily life. The Italian version has a good internal consistency with Cronbach's alpha of 0.94 (De Pasquale et al., 2016), and the same value (0.94) was found in our sample.
Experimental procedure: a task to measure PPSWe created a computer-based task to measure PPS boundaries in several social conditions. The task was an adapted version of the stop-distance paradigm typically used to measure peripersonal and interpersonal space (Iachini et al., 2014; Nandrino et al., 2017).
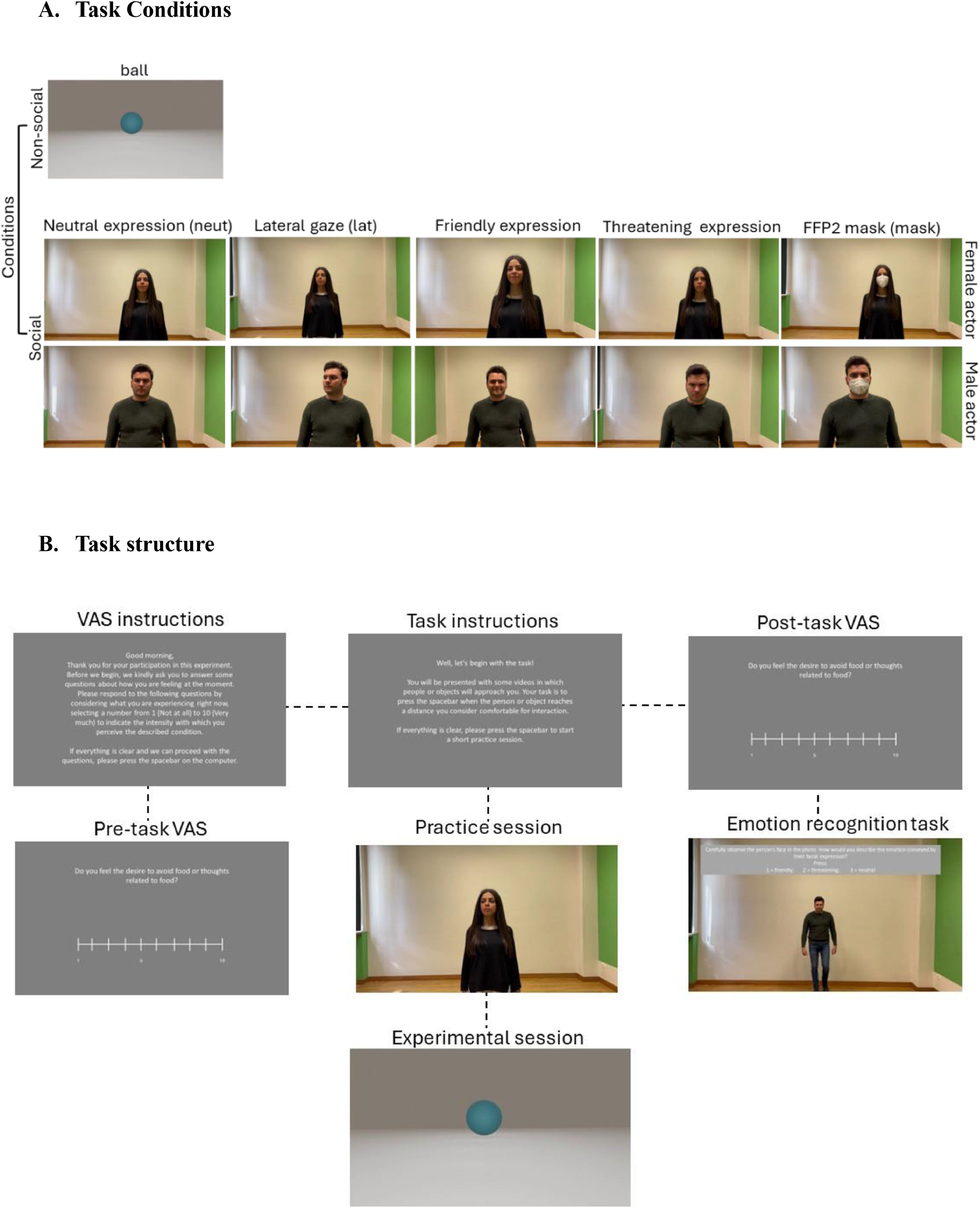
Stimuli creation. We recruited two actors (one male, one female) of 28 and 26 years old respectively. We filmed the actors approaching along a distance of 4 m at a constant speed, marked by auditory signals, of half a meter per second; each video thus lasted 8 s. We recorded for both actors 5 videos with the following different facial expressions: 1) neutral (no conveying emotions) looking straight ahead, 2) turning the gaze laterally, 3) with a friendly expression, 4) with a threatening expression; 5) wearing an FFP2 mask. We then added a non-social condition virtually creating a video in which a ball rolls toward the camera along the same distance and at the same speed adopted by the actors.
Task structure. The task consisted of 11 conditions, 10 social conditions: female actor with neutral facial expression (neut_F), gaze turned laterally (lat_F), friendly expression (friend_F), threatening expression (threat_F), and wearing a mask (mask_F); male actor with the same expressions (neut_M, lat_M, friend_M, threat_M, mask_M), and a non-social condition (ball; conditions are summarizes in Fig. 1.A). Before and after the PPS task, participants were asked to answer 10 questions about their current state on a visual analog scale (VAS) ranging from 0 to 10. The questions assessed the following topics: anxiety level, hunger level, food craving, desire to do physical activity, desire to avoid food, arousal level, physical reactions (i.e., heart rate acceleration, sweating), inner sensations, feeling the surroundings as non-realistic (e.g., like being in a dream), feeling of being a spectator of what happening. At the end of the task, we proposed an emotion recognition task: looking at the photos of the actors in the 3 social conditions related to emotions (neutral, friendly, and threatening) participants were asked to indicate what facial expression the actor was adopting choosing among 3 possibilities (neutral, friendly, threatening).

Task procedure. Participants were comfortably seated in front of a laptop (DELL XPS 15 with a display of 15.6 inches, resolution of 1920×1080 pixels, and refresh rate of 60 Hz) placed at a distance of 50 cm. The experimenter accurately explained the task and ensured that the participant had understood the procedure. At the beginning of the task written instructions on the screen were provided, the participant answered the VAS and completed a practice section of 11 videos (i.e., one for each condition, see Fig. 1). After the pre-task VAS session, the experimental session began: each video was repeated 15 times in a block design with 15 blocks for a total of 165 trials; in each block, the conditions were presented in a randomized order. Participants were asked to pretend that the actor or the object in the video was approaching her/him and to stop the actor or the object, by pressing the space bar on the keyboard of the laptop, when the subject was at a comfortable distance for social interaction. The response time (RT) was measured in seconds with millisecond precision, ranging from 0 to 8. A value of 0 indicated that participants halted the video at the initiation when the actor was at the maximum distance (4 m), whereas a value of 8 indicates that subjects paused the video when the actor was in the nearest proximity (0 m between cameras and actor's face). Then the RT was turned in distance with the formula:
in which MD represents the maximum distance that was equal to 4 m and RT represents the reaction time for participant to press the space bar from the trial start. The resulted value ranges between 0 and 4, with 0 representing the nearest proximity and 4 the maximum distance. At the end of the trials, participant answered to the VAS and to the emotions recognition task (Fig. 1.B summarizes the task procedure). Stimuli presentation, timing, and randomization were controlled using PsychoPy software (Peirce et al., 2019).Statistical analysis
Statistical analysis was performed adopting R (version 4.3.1), using Rstudio, and SPSS (version 29.0.1.0). Linear mixed effects models (LMEM) were adopted to assess the significance of differences in PPS amplitude compared with experimental conditions and blocks across the two groups (i.e., patients with AN and healthy control subjects). LMEM analyses were executed utilizing the glmer function from the R package ‘lme4’ (version 1.1–27.1). The structure of the random effects in the model was determined by applying the Bayesian Information Criterion (BIC), a criterion that seeks to identify the model that offers a superior fit with reduced complexity. The significance of all fixed effects was evaluated by performing likelihood-ratio tests (LRTs) between mixed models that differed only in the inclusion or exclusion of a specific predictor (Model selection results are reported in Supplementary Table 2). The R package ‘emmeans’ (version 1.7.2) was used to investigate interactions, providing post-hoc estimates of interaction slopes in linear models (Montobbio et al., 2022; Scaliti et al., 2023) with Tuckey correction for multiple comparisons. We performed a power analysis following Kumle et al. (2021): using the R package “mixedpower” we used plausible sample size to estimate power (i.e. 20, 40, 60, 80, and 100) including an approximation of our sample size (i.e. 80) and an alpha level of 5 %. We included Actors’ gender, Condition, and Groups (i.e., AN vs HC) as fixed effects and participant as random variable for the simulation. This analysis showed a power greater or higher than 80 % for all the fixed effects (and their interactions) when the sample size is above 80 participants (for details, see Supplementary Table 3 and Supplementary Figure 2). To estimate effect size in LMEM we calculated the Conditional R-squared (R2c), which indicates the portion of variance explained by combined fixed and random effects in the model, using the R package ‘MuMIn’. R2c values close to 1 mean that a great portion of the variance is explained by the model.
Independent sample t-test with Cohen's D calculation was run to describe the overall sample in terms of differences between patients with AN and HCs.
Paired sample t-test was used to investigate differences between pre and post-task VAS scores.
An accuracy index for the emotion recognition task was calculated for all participants. Subjects scored 1 if the answer was correct and 0 in case it was wrong: the accuracy index consisted of the mean of accuracy scores gained in the six questions on actor's facial expression and it ranged from 0 to 1, with higher scores corresponding to higher number of expressions correctly recognized. The difference in accuracy between patients with AN and HCs was calculated with independent sample t-test.
Finally, linear regression models were performed to investigate the association between the mean PPS amplitude and eating-related and general psychopathology symptoms and to explore the association between the accuracy index for the emotion recognition task and the PPS amplitude. In particular, for each group we created a regression model with mean PPS as dependent variable and clinical variables (e.g., years of illness, BMI, age) as independent variables, a second model with mean PPS as dependent variable and eating-related symptoms (e.g., restriction, weight concern) as independent variables, a third model with mean PPS as dependent variable and general psychopathology symptoms (e.g., depression, anxiety) as independent variables, and a last model had mean PPS as dependent variable and accuracy in emotion recognition as independent variable; in this last case, we considered the mean PPS calculated on the six emotion-related conditions (i.e., neutral, friendly, threatening, each one for both male and female actor). When the associations were significant, we adjusted the regression models controlling for the role of possible covariates (e.g., BMI, anxiety).
ResultsSample characteristicsThe sample consisted of 46 inpatients with AN, 24 with R-AN, 14 with BP-AN, 9 with atypical AN, and 42 HCs for a total of 88 participants. The two samples were comparable regarding the age, whereas patients had a significantly lower BMI and higher eating-related and general psychopathology (See Supplementary Table 1).
Mixed models analyses on PPS modulationThe mean PPS amplitudes for the two groups are reported in Table 1. Mixed models analyses showed a main significant effect of the groups (i.e., patients with AN vs HCs), namely patients with AN chose a significantly higher distance to interact with actors in all conditions. A significant main effect of actors’ gender (i.e., female vs male) emerged, revealing that all subjects kept the male actor at a higher distance than the female actress, and of agent (i.e., human vs not human) with participants choosing a higher distance from actors than from the object (Table 2). Two-way significant interactions were found between groups and actors' gender, groups and conditions, and actors' gender and conditions, reflecting that the response was modulated by these combinations of factors (Table 2). The three-way interaction among groups, actors' gender, and conditions significantly affected the response (Table 2). Crossing conditions and actors’ gender within the groups, it emerges significant higher distances in male interactions compared to female ones independently of the condition for the majority of the contrasts; however, in the patients group, the condition mask_M did not differ from Friend_F and Lat_F, and in HCs Neut_M did not differ from Threat_F. Lastly, Friend_M and Lat_M were not significantly different from Threat_F and Mask_F. Concerning the three-way interaction, patients with AN and HCs modulated the distance from the different conditions in a similar way, namely keeping further away the Threatening conditions than the others, and nearer the neutral conditions or the ball. For contrasts details see Supplementary Table 3 and Fig. 2. Conditional R-squared, assessing effect size for fixed and random effects combined in the model had a value of 0.724, suggesting good effect size of our model.
Mean PPS values.
| Patients with AN (N = 46) | Healthy controls (N = 42) | |
|---|---|---|
| Mean (SE) | Mean (SE) | |
| Total_PPS | 2.1 (0.09) | 1.5 (0.07) |
| PPS_F | 2 (0.09) | 1.4 (0.08) |
| PPS_M | 2.3 (0.09) | 1.6 (0.08) |
| Social_PPS | 2.1 (0.9) | 1.5 (0.08) |
| Neut_F | 1.8 (0.09) | 1.2 (0.07) |
| Neut_M | 2.3 (0.11) | 1.6 (0.09) |
| Happy_F | 1.9 (0.09) | 1.4 (0.06) |
| Happy_M | 2.2 (0.10) | 1.6 (0.08) |
| Lat_F | 2 (0.09) | 1.4 (0.08) |
| Lat_M | 2.2 (0.09) | 1.6 (0.08) |
| Angry_F | 2.3 (0.13) | 1.6 (0.10) |
| Angry_M | 2.5 (0.11) | 1.8 (0.10) |
| Mask_F | 2.1 (0.09) | 1.5 (0.08) |
| Mask_M | 2 (0.11) | 1.3 (0.09) |
| Ball | 1.9 (0.09) | 1.3 (0.08) |
Total PPS = mean PPS amplitude for all conditions; PPS_F = mean distance from female actress; PPS_M = mean distance from male actor; Social PPS= mean PPS amplitude for all conditions except “Ball”.
Summary of likelihood ratio test for significance of main effects and product terms in mixed effect statistics related to Fig. 2.
| χ2 | df | P | |
|---|---|---|---|
| Intercept | 212.71 | 1 | <0.001 |
| Agent | 26.53 | 1 | <0.001 |
| Groups (AN vs HC) | 26.62 | 1 | <0.001 |
| Actors’ gender | 273.24 | 1 | <0.001 |
| Condition | 236.94 | 4 | <0.001 |
| Groups*Actors’ gender | 20.99 | 2 | <0.001 |
| Groups*Condition | 50.91 | 4 | <0.001 |
| Actors’ Gender*Condition | 479.09 | 4 | <0.001 |
| Groups*Actors’ Gender*Condition | 26.95 | 4 | <0.001 |
Patients with AN (n = 46) and HCs (n = 42).
Response_mt ∼ Agent + Groups * Actors’ gender * Condition + (1|participant).
 Bars represent standard error.")
Main and interaction LMEM effects on PPS modulation.
a. Main effects of Agent, Groups, Actors’ gender, and Conditions. ***: p < .001
b. Groups*Actors*Conditions interaction effect.
c1 and c2. Significant post-hoc contrasts in the two groups (Healthy controls on top and patients with AN on bottom)
Bars represent standard error.
As described above, 4 males (2 HCs and 2 patients with AN) took part in the task; Supplementary Figure 2 (Supplementary Materials) shows a single-subject trend in PPS mean scores for these 4 participants.
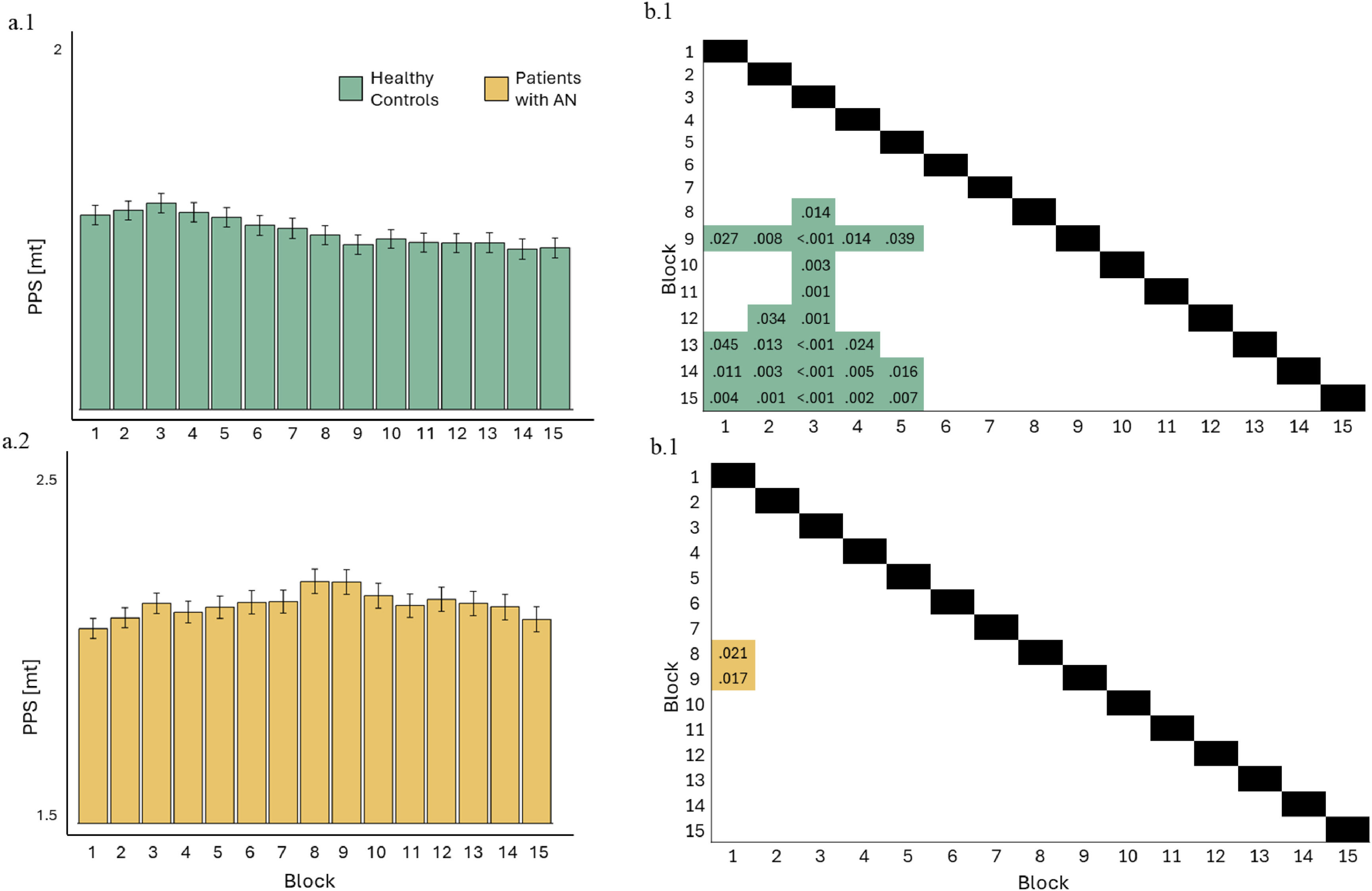
Effect of time on PPS modulation on the two groupsMixed models showed a significant effect of blocks in HCs (Table 3): post-hoc comparisons showed a significantly reduced mean distance in the last block compared to the first, and this effect is progressively present among the blocks (see Fig. 3) with a lower distance in the final part of the task than in initial one. Considering patients, the effect of the block was significant (Table 3) but we did not find a progressive decrease in the chosen distance (i.e., post-hoc did not show a significant difference between the first and the last blocks) but a significant increase of PPS between the first and the two middle blocks (Fig. 3).
Summary of likelihood ratio test for significance of main effects and product terms in mixed effect statistics related to Fig. 3.
| χ2 | df | p | |
|---|---|---|---|
| Intercept | 678.44 | 1 | <0.001 |
| Blocks | 28.38 | 14 | .013 |
| Healthy control subjects (n = 42) | |||
| Response_mt ∼ Blocks + (1|participant) | |||
| χ2 | df | p | |
| Intercept | 407.16 | 1 | <0.001 |
| Blocks | 103.68 | 14 | <0.001 |
Patients with AN (n = 46).
Response_mt ∼ Blocks + (1|participant).
. b.1 and b.2. Significant post-hoc contrasts in the two groups (Healthy controls on top and patients with AN on bottom) Bars represent standard error.")
Main LMEM effect of blocks on PPS modulation.
a.1 and a.2. Main effects of Blocks in the two groups (Healthy controls on top and patients with AN on bottom).
b.1 and b.2. Significant post-hoc contrasts in the two groups (Healthy controls on top and patients with AN on bottom)
Bars represent standard error.
In patients with AN no differences emerged between pre and post-task VAS (Table 4). In the group of HCs, the post-task scores of inner sensations and desire to do physical activity were significantly lower than the pre-task scores (Table 4).
Differences between pre and post-task VAS scores.
| Pre-task | Post-task | Statistical analysis | |||
|---|---|---|---|---|---|
| Patients with AN (n = 46) | Mean (SD) | Mean (SD) | t | p | Cohen's D |
| VAS inner state | 6.7 (2.9) | 6.4 (3.1) | .833 | .409 | .126 |
| VAS arousal | 4.9 (2.9) | 5.1 (3) | −0.629 | .533 | −0.094 |
| VAS reactions | 4.8 (3) | 4.6 (3.1) | .560 | .578 | .083 |
| VAS non-realistic | 3.3 (2.5) | 3.2 (2.4) | .502 | .618 | .075 |
| VAS spectator | 3.9 (2.9) | 3.4 (2.8) | 1.551 | .128 | .234 |
| VAS anxiety | 6.2 (3.1) | 6.2 (3.4) | .219 | .827 | .033 |
| VAS hunger | 2.7 (2.3) | 2.3 (2.2) | 1.868 | .068 | .278 |
| VAS craving | 3 (2.6) | 2.6 (2.5) | 1.373 | .167 | .207 |
| VAS food avoidance | 7.2 (2.9) | 7.3 (2.9) | −0.715 | .478 | −0.108 |
| VAS physical activity | 7.1 (2.9) | 9.4 (2.9) | −1.118 | .269 | −0.167 |
| HCs (n = 42) | |||||
| Pre-task | Post-task | Statistical analysis | |||
| Mean (SD) | Mean (SD) | t | p | Cohen's D | |
| VAS inner state | 2.4 (1.7) | 2 (1.6) | 2.520 | .016 | .389 |
| VAS arousal | 1.8 (1.2) | 1.8 (1.3) | −0.411 | .683 | −0.063 |
| VAS reactions | 1.8 (1.1) | 1.6 (1.1) | 1.603 | .117 | .247 |
| VAS non-realistic | 1.2 (0.4) | 1.4 (0.9) | −1.303 | .200 | −0.202 |
| VAS spectator | 1.5 (0.8) | 1.4 (0.8) | .500 | .620 | .067 |
| VAS anxiety | 2.2 (1.3) | 2.1 (1.5) | .289 | .774 | .045 |
| VAS hunger | 2.5 (1.8) | 2.5 (2.1) | −0.342 | .734 | −0.053 |
| VAS craving | 2.8 (2.3) | 2.7 (2) | .751 | .457 | .116 |
| VAS food avoidance | 1.6 (0.9) | 1.5 (0.9) | 1.409 | .167 | .217 |
| VAS physical activity | 2.9 (2.3) | 2.4 (2.1) | 3.090 | .004 | .467 |
The accuracy of facial expressions recognition was high and above chance level for both groups (patients with AN: mean = 0.86, SD = 0.19; HCs: mean = 0.92, SD =0.11); however, the mean accuracy of HCs was significantly higher than patients’(t = 2.01; p = .047).
Association between PPS and eating-related and general psychopathologyNo significant associations emerged between PPS amplitude and clinical variables and eating-related psychopathology in patients with AN (Table 5); a negative significant association was found between mean PPS and self-esteem, namely the lower the self-esteem, the larger the chosen distance (Table 5). Moreover, the accuracy index for the emotion recognition task was significantly and negatively associated with mean PPS for the conditions characterized by emotion-related facial expressions; this result was independent of BMI, years of illness, anxiety, depression, and self-esteem.
Associations between social PPS and psychometric data in patients with AN.
| B | SE | β | p | IC 95 % | p*/p**/p*** | |
|---|---|---|---|---|---|---|
| Model 1: dependent variable: mean PPS - independent variables: clinical variables | ||||||
| Age (years) | .015 | .027 | .189 | .526 | −0.041–0.070 | |
| BMI | .016 | .023 | .110 | .487 | −0.031–0.060 | |
| Years of illness | −0.027 | .027 | −0.351 | .334 | −0.082–0.029 | |
| Model 2: dependent variable: mean PPS - independent variables eating-related psychopathology | ||||||
| EDI-2 drive for thinness | −0.016 | .039 | −0.169 | .677 | −0.096–0.063 | |
| EDI-2 Bulimia | .000 | .018 | −0.002 | .991 | −0.037–0.037 | |
| EDI-2 Body dissatisfaction | .009 | .026 | .105 | .745 | −0.045–0.062 | |
| EDE-Q dietary restrain | .071 | .123 | .235 | .571 | −0.182–0.323 | |
| EDE-Q food concern | .057 | .126 | .152 | .655 | −0.201–0.314 | |
| EDE-Q weight concern | .029 | .175 | .083 | .869 | −0.330–0.338 | |
| EDE-Q shape concern | −0.108 | .239 | −0.259 | .657 | −0.599–0.384 | |
| BSQ | .001 | .006 | .087 | .849 | −0.012–0.014 | |
| Model 3: dependent variable: mean PPS - independent variables general psychopathology | ||||||
| BDI | −0.019 | .027 | −0.178 | .492 | −0.076–0.038 | |
| STAI-Trait | .010 | .015 | .172 | .523 | −0.021–0.041 | |
| STAI-State | −0.009 | .011 | −0.168 | .437 | −0.032–0.015 | |
| DES | .014 | .007 | .376 | .058 | −0.001–0.029 | |
| Rosenberg Self-esteem scale | −0.057 | .013 | −0.788 | <0.001 | −0.084–0.030 | .003 |
| Model 4: dependent variable: mean PPS** - independent variable: emotion recognition accuracy | ||||||
| Emotion recognition accuracy | −1.805 | .452 | −0.583 | <0.001 | −2.728–0.883 | .026/0.001/0.003 |
**regression analyses between emotion recognition accuracy and mean PPS amplitude in the conditions related to facial expressions (i.e., neutral, friendly, threatening).
p*=model adjusted for BMI and years of illness.
p**= model adjusted for depression and anxiety.
p***= model adjusted for self-esteem.
In HCs, mean PPS was significantly associated with body dissatisfaction, eating restraint, and weight concerns, and these data survived the statistical adjustment for anxiety and depression. A significant negative association emerged between trait anxiety and PPS (Table 6).
Associations between PPS and psychometric data in HCs.
| B | SE | β | p | IC 95 % | p* | |
|---|---|---|---|---|---|---|
| Model 1: dependent variable: mean PPS - independent variables: clinical variables | ||||||
| Age (years) | −0.016 | .035 | −0.077 | .654 | −0.086–0.055 | |
| BMI | .021 | .035 | .103 | .550 | −0.050–0.093 | |
| Model 2: dependent variable: mean PPS - independent variables eating-related psychopathology | ||||||
| EDI-2 drive for thinness | .009 | .050 | .056 | .861 | −0.094–0.111 | |
| EDI-2 Bulimia | .135 | .116 | .256 | .257 | −0.105–0.375 | |
| EDI-2 Body dissatisfaction | −0.084 | .028 | −0.994 | .006 | −0.141- −0.026 | .028 |
| EDE-Q dietary restrain | .315 | .147 | .541 | .042 | .012–0.618 | .029 |
| EDE-Q food concern | −0.230 | .283 | −0.293 | .425 | −0.812–0.353 | |
| EDE-Q weight concern | .470 | .174 | .949 | .012 | .112-..829 | .004 |
| EDE-Q shape concern | .049 | .143 | .146 | .737 | −0.247–0.344 | |
| BSQ | −0.005 | .010 | −0.274 | .583 | −0.026–0.015 | |
| Model 3: dependent variable: mean PPS - independent variables general psychopathology | ||||||
| BDI | .052 | .031 | .412 | .104 | −0.012–0.116 | |
| STAI-Trait | −0.038 | .018 | −0.713 | .048 | −0.076–0.000 | |
| STAI-State | .031 | .018 | .576 | .089 | −0.005–0.067 | |
| DES | −0.014 | .009 | −0.295 | .135 | −0.033–0.005 | |
| Rosenberg Self-esteem scale | .001 | .010 | .013 | .944 | −0.020–0.022 | |
| Model 4: dependent variable: mean PPS** - independent variable: emotion recognition accuracy | ||||||
| Emotion recognition accuracy** | −0.074 | .764 | −0.015 | .923 | −1.618–1.469 | |
**regression analyses between emotion recognition accuracy and mean PPS amplitude in the conditions related to facial expressions (i.e., neutral, friendly, threatening).
The present study aimed to explore PPS in AN, comparing patients to healthy subjects (HCs). The following findings emerged: 1) the PPS of the patients was significantly larger than the PPS of HCs and both patients with AN and HCs modulated the comfortable chosen distance basing on the gender and the expression of the actors, and the nature of the agent (i.e., human or not human); 2) while HCs gradually decreased PPS through the task, patients with AN maintained a constant distance from the stimuli; 3) the scales evaluating “inner sensations” and “desire of doing physical activity” decreased after the task in HCs, while no changes in the state of individuals after the task emerged in patients with AN; 4) patients with AN were significantly less accurate in identifying the actors’ facial expression; 5) negative significant correlation between PPS amplitude and self-esteem emerged in patients with AN; examining the group of HCs we found significant correlations between PPS and eating-related symptoms and trait anxiety; moreover, in the group of patients, the mean emotion recognition accuracy negatively and significantly correlated with the mean PPS in the conditions in which actors conveyed emotions; this correlation did not emerge in HCs.
Although the two groups similarly modulated PPS, patients with AN needed an overall larger distance to interact with actors in all conditions of the task, in line with our hypothesis and Nandrino et al. (2017). This result could be related both to the perceptive alterations typical of AN (Magrini et al., 2022; Zitron-Emanuel et al., 2022) and the lived negative bodily experience: the overestimation of the body size could have such a deep influence to impact an implicit construct as PPS, similar to what was described for other components of bodily self-consciousness (Colle et al., 2023; Meregalli et al., 2023). Moreover, the enlargement of PPS could have a role in the social anxiety often associated with AN (Swinbourne & Touyz, 2007), especially regarding Social Physical Anxiety, an anxiety strongly related to the fear of being observed or negatively judged basing on the physical aspect (Alcaraz-ibáñez et al., 2023): Social Physical Anxiety is commonly reported in AN, also because of the common substrate regarding the negative relationship with the body. Furthermore, the alteration of PPS was observed also in other psychiatric conditions such as schizophrenia and anxiety disorders (de Vignemont & Iannetti, 2015). PPS impairment thus could be considered both as a transdiagnostic factor and as an index of mental suffering, but further studies are needed to test this hypothesis.
Mixed models analyses revealed a significant effect of actors’ gender and condition (i.e., facial expressions), and the interaction between these factors on PPS emerged in both patients with AN and HCs. Both groups chose a lower distance to interact with the female subject than with the male, in line with the literature on non-clinical samples suggesting higher security of female individuals in interacting with a same-gender individual (Iachini et al., 2014); however, our data contrast with Nandrino et al. (2017), and our a-priori hypothesis, who described a higher distance to the female actor than to the male one (Nandrino et al., 2017). Of note, the previous study differs from ours in several aspects: the composition of the clinical group (i.e., Nandrino et al. recruited patients with R-AN, while we included both AN diagnostic subtypes), the amplitude of the sample and the structure of the PPS task. This could be relevant since subjects with R-AN are more inclined to social comparison than subjects with the binge purging variant of AN (Arcelus et al., 2013): this could explain the greater hostility towards female figures that emerged in the previous study. Noteworthy, the post-hoc comparisons within groups in our study suggest that while HCs are driven more by the facial expression of the actor than by the gender to choose the comfortable distance, patients are more influenced by the gender, keeping the male actor more distant than the female regardless of their facial expression. Surprisingly, the most recent study on PPS in AN (Cartaud et al., 2024) did not explore the role of gender. Since our study showed the same trend toward gender in patients and HCs, in line with the literature on PPS in HCs, but Nandrino et al. (2017) reported the opposite trend, the debate is still open.
This is the first study to investigate the influence of facial expression on PPS in patients with AN in a dynamic way with human actors: according to our hypothesis, data suggest a similar modulation of PPS basing on facial expression in AN and HCs, showing the largest distance in the threatening conditions. These data are in line with previous studies on healthy subjects showing an increase in the comfort distance when the approaching subject had an angry expression, thus eliciting avoidant and defensive behaviors (Cartaud et al., 2018; Ruggiero et al., 2017). The only recent study that analyzed interpersonal distance in AN in relation to emotional expressions is in line with our findings, reporting greater need for distance when subjects with AN are confronted with angry facial expressions. However, the comparison between the two studies is difficult because Cartaud et al. (2024) adopted a different method. Specifically, the use of avatars and static tasks makes the study less ecological and less similar to real-world interactions. Moreover, in our opinion, the tasks adopted by Cartaud et al. evaluate mainly the knowledge about one's own PPS: the participants are indeed asked to give a judgment on the interpersonal distance, removing thus the threat component inherent to dynamic approaching stimuli. This is also confirmed by the lack of electrodermal activity increase in response to angry virtual characters reported by the authors in patients with AN. Differently, the stop-distance paradigm allows to capture a more ecological PPS adjustment reflecting the implicit and automatic mechanisms underlying the modulation of interpersonal distance in the real world.
In contrast to our assumptions, we did not find a strong effect of the “lateral gaze” conditions in shortening the distance from the actors: it could be speculated that although the tendency of patients with AN to avoid other's gaze (Watson et al., 2010) - also considering the social functioning-related autistic traits described in AN (Boltri & Sapuppo, 2021) - the same behavior adopted by an approaching actor does not influence the choice of the comfortable social distance. Similarly, wearing an FFP2 mask did not influence significantly the overall distance, with PPS in Mask conditions smaller than Threatening conditions but not than other conditions in both patients with AN and HCs. This is in contrast with Kühne et al. (2022) who reported that face masks reduced interpersonal space in non-clinical subjects during the COVID-19 pandemic (Kühne et al., 2022). The two studies, however, differ not only in the sample composition and task setting but also because Kühne et al. tested participants during the peak and the end of pandemic waves, while we did not recruit participants during the COVID-19 peaks but after each wave and at the end of the pandemic.
Moreover, the nature of the agent (i.e., human or not human) significantly affected the choice of the distance with an overall larger PPS for humans than ball.
An interesting result regards the change in the PPS boundaries during the task: while HCs progressively decreased the mean distance from the stimuli through the task, suggesting a familiarization with the approaching subjects, patients did not change the preferred distance across the blocks. It could be hypothesized that the repeated exposition to a stimulus does not induce habituation or familiarization in patients with AN. To our knowledge, this is the first study to consider this variable that deserves a deeper exploration since it could have important implications in the treatment of social anxiety and phobias in AN. Given this, the need for a larger distance to interact with others, and the lack of familiarization during the task could prompt social anxiety, especially in contexts in which the required distance cannot be granted.
It is known that individuals with AN show high levels of cognitive rigidity (Buzzichelli et al., 2018) and tend to maintain behaviors rigidly; it is of interest that the rigidity does not emerge only in cognitive tasks, but involves other different aspects such as the modulation of PPS.
Participants completed a set of questions about their current state before and after the PPS task. Patients with AN did not show differences between pre and post-task assessment, while HCs decreased the confusion about their inner states and the desire to do physical activity after the task. These data are novel and difficult to comment on, but they suggest a different effect of sociality in patients and HCs, to be further investigated, and corroborate the fact that - while healthy subjects change their emotional state during the task, - AN sufferers remain rigid in this case too.
In patients with AN, lower self-esteem correlated with a larger distance chosen to interact with actors. Given the acknowledged negative self-perception and the social physical anxiety typical of subjects with AN (Alcaraz-ibáñez et al., 2023; Brockmeyer et al., 2013), this correlation could reflect an attempt to protect the body from negative feelings and other's judgment by keeping them at distance. Unexpectedly, no correlations with eating-related symptoms emerged, in contrast with Nandrino et al. (Nandrino et al., 2017), but, again, the two studies are scarcely comparable, and, surprisingly, Cartaud et al. (2024) did not explore the link between eating-related symptoms and interpersonal space. The role of self-esteem in PPS modulation is however intriguing. Low self-esteem is a core driver of the eating disorder (Fairburn et al., 2003); moreover, according to the Arcelus model (2013), the link between relationship difficulties and eating symptoms is mediated by low self-esteem (Arcelus et al., 2013). Finally, the feeling of inadequacy and the related difficulties of the self are therapeutically more relevant than the cognitive symptoms (Skårderud, 2009). Differently, the PPS of HCs significantly correlated with body dissatisfaction, weight concern, and dietary restraint. These data are novel and suggest that the subjective experience of the body and the subclinical concern about weight and diet lead to a different modulation of PPS having an impact on the quality of social interaction; these data highlight the importance of eating-related dimension in daily life and in general population.
In HCs trait anxiety was negatively and significantly associated with PPS showing that higher levels of anxiety were related to a lower chosen distance. These data are in contrast with studies showing the need for higher social distance in people with trait anxiety (Iachini et al., 2015; Sambo et al., 2012); however, our result is in line with von Mohr et al. (2023) who showed that healthy people with high attachment anxiety preferred closer interpersonal distance. It could be speculated that healthy individuals with stable anxiety could tend to search for social proximity to adaptively cope with anxiety. Following the attachment theory (Bowlby, 1979), the way of managing anxiety has at least two styles: an anxious worried one requiring greater closeness to the other and an anxious evasive one, distancing the other. The different emotions of the children regarding attachment styles may correlate with the opposite difference in the modulation of the PPS. The literature on the topic reflects a debate still open.
Finally, although both groups were accurate in identifying actors' facial expressions, patients were significantly less accurate than HCs. This result is in line with previous literature detecting poorer emotion recognition abilities in AN than in HCs (Blomberg et al., 2021; Martini, Marzola et al., 2023). In our study, the mean accuracy in emotion recognition was negatively correlated with the amplitude of PPS, namely the lower the accuracy the larger the PPS; this correlation was not significant in the group of HCs. We speculated that, since facial expressions influence the choice of comfortable distance (Bogdanova et al., 2021), minor difficulties in recognizing facial expressions could cause uncertainty about the other's intention, leading the patients to maintain a larger distance. Anyway, as described above, we observed in patients a pattern of PPS modulation based on facial expression similar to the one showed by HCs: we can thus speculate that the less accuracy in emotion recognition influences the mean general distance from others but does not prevent defensive implicit mechanisms such as distancing approaching other with hostile or threatening expression. A consequent hypothesis is that the defensive function of PPS in AN is preserved or intensified, while the social function is impaired and influenced by some factors such as self-esteem and explicit emotion recognition; future studies are needed to deepen this topic.
Data on regressions lead us to suppose different mechanisms underlying PPS modulation in patients with AN and HCs. Patients’ choice of comfortable distance could be driven by psychopathological cores such as deeply impaired self-esteem and inabilities in others’ emotion recognition; differently, in HCs PPS modulation is influenced by the subclinical and culturally spread phenomenon of body dissatisfaction, and by a restrictive-like pattern of symptoms (i.e., restriction and weight concern) related to a higher distance. Future studies will ascertain whether psychological problems are the cause or consequence of the disease state or both. However, it is interesting to notice that PPS in AN is not associated with specific eating-related symptoms. These findings led to asking about the above-mentioned transdiagnostic nature of PPS alteration, given the lack of significant relations between PPS amplitude and severity of eating-related symptoms in patients; on the other hand, the present study showed correlations between PPS and self-esteem and difficulties in emotion recognition, both typically present in patients with AN, suggesting that PPS could be an important non-specific factor entangled with other typical symptoms of AN.
This study has some limits: firstly, we used self-report measures to assess eating-related and general psychopathology, thus recall bias could be present; secondly, the sample size was relatively small for the regression analysis within the groups, while this limit was overcome in the exploration of PPS with the adoption of mixed models; thirdly, the number of males participants was small so results cannot be generalized to male patients with AN; lastly, the study did not include a control group of patients with other psychiatric diagnosis.
To summarize, the present study deepened the investigation of PPS in AN with an ecological task and a design that considered both external (e.g., actors’ gender and facial expression) and internal (e.g., current subjective state, self-esteem) variables potentially impacting the choice of the distance to interact with others. PPS in AN is not only larger than in HCs, but also probably more rigid: it indeed does not change with the repeated exposition to the stimuli of the task, and it is not related to the levels of psychopathology of the subjects. Moreover, in patients with AN, the choice of the interacting distance is negatively correlated with the ability to correctly recognize the facial expression of the other.
The results shed light on an implicit and important bodily-related constructs such as PPS in AN, and could have relevant clinical implications. PPS alteration should be borne in mind when treating with patients with AN, reminding that they could need a higher distance to interact. Moreover, the PPS width could be a proxy of social anxiety level, and a treatment target in AN. Lastly, the growing applications of virtual reality to treatments could help to develop rehabilitation techniques and increase the ability to modulate the PPS of those suffering from AN.
FundingNone.
None.
