



Edited by: Óscar F. Gonçalves
More infoThe present study examined the impact of the COVID-19 pandemic on the emotional quality of dreams, the incorporation of pandemic-related themes, and the occurrence of lucid dreaming. Dream reports and lucidity ratings of psychiatric outpatients (n = 30) and healthy controls (n = 81) during two lockdowns in Germany were compared to those of healthy controls (n = 33) before the pandemic. Results confirmed previous reports that pandemic-specific themes were incorporated into dreams. Overall, however, incorporation into dreams was rare. Contrary to expectations, psychiatric outpatients did not differ from controls in the frequency of dream incorporation of pandemic-related content. Moreover, incorporation was independent of psychiatric symptoms and loneliness. Loneliness was, however, associated with threat-related content, suggesting that it represents a risk for bad dreams but not for crisis-specific dream incorporation. Regarding lucid dreaming, both groups had similar scores for its underlying core dimensions, i.e., insight, control, and dissociation, during the two lockdowns. Scores for control and dissociation but not insight were lower compared to the pre-pandemic sample. Our working hypothesis is that REM sleep during lockdowns intensified as a means of increased emotional consolidation, rendering the associated mental state less hybrid and thereby less lucid.
The question to what extent, or if at all, waking experiences are implemented in dreams has a long tradition in dream research. The continuity between waking and dreaming is often measured by how often residuals of daytime experience appear in the dream, but also by the extent to which feelings and themes of waking life are incorporated into the dream. In particular, the salience of waking life experiences has been shown to influence the emotional quality of dreams (Cartwright et al., 2006). As such, the study of dreams during crises and crisis-like events like natural catastrophes and traumatizing life events provide important insights into the functionality of dreams and its relation to waking life (Mellman et al., 1995; Wood et al., 1992).
However, despite extensive research, results of crisis-related effects on dreams are inconclusive. For example, in the context of the 9/11 terrorist attacks, some authors reported higher dream intensity, but no incorporation of the terrorists attacks themselves (Hartmann & Basile, 2003; Hartmann & Brezler, 2008), suggesting emotional arousal continuity but not concrete thematic continuity. Others present evidence that elements of the trauma are, indeed, incorporated into dreams but the incidence of incorporation is low, ranging from mere six and a half percent of 3/4 of participants (Bulkeley & Kahan, 2008) to 12% of all participants (Propper et al., 2007). These findings point to possible mediating factors hitherto not sufficiently addressed, such as sample characteristics, psychological vulnerability, or cultural differences.
Regarding vulnerability, the diathesis-stress model (Wittchen & Hoyer, 2011) proposes that the combination of personal dispositions and life stressors can promote mental illness. The more pronounced the dispositions, but also the greater the stressors, the more likely is the onset of a mental disorder. Conversely, those with a mental health disorder tend to respond with greater emotional arousal to stressful life events by attributing higher salience to these events. Theoretically, increased salience should also increase the likelihood of dream incorporation. This presumption is consistent with the finding of Mellman et al., and Nolan (1995) that Vietnam veterans with PTSD were significantly more likely to dream about combat compared to veterans without PTSD.
Regarding emotional dream content, negatively toned dreams such as nightmares and bad dreams have been found to occur more frequently in the aftermath of traumatic events such as hurricanes, earthquakes, or the terrorist attacks of 9/11 (Mellman et al., 1995; Nielsen et al., 2006; Schuster et al., 2001; Wood et al., 1992). Such effects were also reported in the absence of a direct personal involvement in the event, i.e., when witnessing the attacks of 9/11 via television or social media (Propper et al., 2007). Similarly, Valli et al. (2005) found that Kurdish refugee children in Iraq without direct war experience reported more dreams containing threatening events than non-traumatized Finnish control subjects. However, in comparison, a group of directly traumatized children had the most threat-dreams compared to the other two groups. These findings are again in line with the emotional arousal theory. While not directly challenging incorporation theory, they do suggest that incorporation is not an all-or-none phenomena.
The ongoing COVID-19 pandemic provides another unique opportunity to examine the impact of experienced crises on dreaming. The episode is unique in the sense of its temporal and territorial extension, representing a potentially life-threatening event of unknown duration for the entire global population that affects everyday life in many ways, and has been present 24/7 on all media channels. In addition to actually causing severe illness in some people, it produced significant psychological distress in the general population in the form of stress, anxiety, depressive symptoms, sleep disturbances, anger, and fear (Solomonova et al., 2021; Torales et al., 2020; S. Wang et al., 2020; C. Wang et al., 2020; Zhou et al., 2020). The imposed lockdowns in many countries around the world contributed to social isolation through the loss of everyday contacts and fostered existential worries (Encheva-Stoykova et al., 2022; Moore et al., 2022).
Several studies have already been conducted, most of which were online studies asking participants to report their most recent dream or asking explicitly for a recent dream about COVID-19. In most studies, dream reports comprised at least some explicit references to COVID-19 (e.g. Kilius et al., 2021; MacKay & DeCicco, 2020; Marogna et al., 2021; Parrello et al., 2021; Pesonen et al., 2020; Schredl & Bulkeley, 2020). However, there were also studies not reporting explicit COVID-19 references (Gupta et al., 2020; J. Wang et al., 2021), again suggesting that mediating factors likely play a role in dream incorporation.
Regarding such mediating factors, we have, in this study, collected dream reports not only from healthy volunteers but also from psychiatric out-patients, assuming that they were more susceptible to the psychological stress invoked by the pandemic and would , thus, incorporate COVID-19 related themes more often into their dreams compared to controls (see Campbell & Germain, 2016; Gorgoni et al., 2021 for changes in dream content as a function of mental health).
Our study aims to provide further insight into the functioning of the dream, testing whether salience determines the degree of dream incorporation not in qualitative but in quantitative terms. In that case, not the objectifiable salience (e.g., actual danger to the self) but the degree of subjectively perceived salience would be crucial for dream incorporation. Thus, we speculated that incorporation would occur only when a certain threshold of perceived emotional involvement is exceeded. As this threshold is lower in emotionally unstable psychiatric patients than in emotionally stable individuals, we hypothesized that the rate of incorporation will be higher in patients than in emotionally stable participants.
Another goal of the current study was to investigate whether the stress invoked by the pandemic affects dream lucidity, i.e., to gain information about situational and mental health-related influences on lucid dreams. A lucid dream can be defined as a dream in which “the dreamer is aware of the fact that he is dreaming while the dream continues” (Voss et al., 2013, S. 9). Lucid dreaming is considered a hybrid state of consciousness with elements of both primary and secondary consciousness, the former pertaining to the REM-dream state and the latter to the waking state (Hobson & Voss, 2011). Primary consciousness refers to a state of simple awareness which is predominant in REM-sleep dreaming, deprived of the dimension “time” or the ability to exert executive functions such as planning ahead, reflecting upon the past or contemplating the future, and decision-making capacities. Secondary consciousness is usually dominant in the waking state, introducing higher order cognitive functions such as self-reflective awareness, abstract thinking, volition, and metacognition (Hobson & Voss, 2010, 2011; Voss et al., 2013).
According to Voss et al. (2013), consciousness during lucid dreaming is mainly defined by three factors: insight into the state of dreaming (knowing one is dreaming while dreaming), control (being able to alter the dream plot), and dissociation (experiencing the dream from a third person perspective). Insight into the state of dreaming must be considered the core factor, however, as it is possible to be lucid, yet incapable of controlling the dream plot, for example. According to a meta-analysis by Saunders et al., and Clegg (2016), most people (on average: 63%) experience a lucid dream at least once in their lifetime, whereas frequent lucid dreams have been reported by an average of 24% of participants, ranging from 8% to 50% (p. 11). As the authors point out, however, these numbers must be interpreted with caution, as sampling biases in lucid dream research are likely (e.g., those who participate in such research often share an interest in lucid dreaming, and lucid dreaming is also known to occur mainly in the young, Voss et al., 2012). Furthermore, criteria for labelling a dream as lucid may vary, depending on whether they originate from the REM-sleep phase, the waking state, or sleep onset, i.e. possibly being confounded with hypnagogic or hypnopompic hallucinations. In children, it was observed that lucidity often developed out of nightmares, representing a successful coping attempt with the threat experienced in the dream (Armstrong-Hickey, 1988; Voss et al., 2012). It would, thus, be conceivable that when confronted with a global crisis, the experience of perceived helplessness, i.e., loss of control, in an uncertain waking-situation, would trigger attempts to gain control and insight into the dream, especially in those who are psychologically vulnerable.
The present studyIn Germany, the first and so far, strictest lockdown in reaction to COVID-19 took place between March 16, 2020, and the beginning of May 2020. During this lockdown, a variety of health and safety measures were imposed, such as wearing a mouth-nose protection, social distancing, closing of stores and schools, working from home office, and 14-day long quarantines for both, infected individuals, and close contact persons. After a phase of apparent relaxation during the summer, a second lockdown light (social distancing rules, but no changes in store openings) was implemented in November 2020, and again tightened shortly before Christmas.
The aim of the present study was to investigate the impact of the pandemic on dream content in an adult German sample from both lockdowns. Additionally, we were interested in the occurrence and characteristics of lucid dreaming. Furthermore, the impact of pandemic-related feelings and worries, as well as the impact of demographic variables on dream content and lucidity was assessed.
To determine the role of psychopathology in altered dreaming during COVID-19, we were interested in whether reported dreaming between healthy adults and psychiatric outpatients differs, assuming that these individuals are affected differently by the pandemic situation. To further elucidate such potential differences and see whether they could explain differences in dream incorporation, we assessed symptoms of psychopathology from all participants (among others depressiveness, anxiousness, and psychoticism). In addition, we wanted to look at individual differences in terms of psychiatric variables between individuals with and without dreams with COVID-19 content.
Further, dimensions of consciousness during dreaming were measured to determine whether higher demands of coping with an extreme situation, and thus potentially higher demands on cognitive control functions, would lead to higher involvement of secondary consciousness/lucidity during dreaming. Therefore, the expression of different dimensions of consciousness in the present lockdown groups were compared to a pre-pandemic sample from 2013 (Voss et al., 2013). To investigate whether dream lucidity differed between psychiatric patients and healthy controls, we compared the data of emotionally stable individuals with those of psychiatric outpatients. Note that Individuals were not selected based on pre-existing susceptibility to lucid dreaming. Rather, we expected that in our sample lucid dreaming should have the same probability of occurring as in any other unselected sample.
MethodRecruitment of participants and study procedures were approved by the local ethics committee of the Goethe University Frankfurt, Germany (Ref. 2020-19).
ParticipantsParticipants in both lockdowns were recruited from a patient population of the Vitos Hochtaunus gGmbH in Germany and from a student population of Goethe-University Frankfurt in two observation periods (first and second lockdown). The patients were made aware of the study through personal contacts; students were recruited through an advertisement on the homepage of the Goethe University Frankfurt. They were encouraged to pass on this invitation to friends and families.
During the first lockdown in Germany (Lockdown 1, L1), study materials were sent to 130 participants between March 26, 2020, and April 08, 2020. Seventy-three participants sent back their materials, five of whom had to be excluded because of zero dream recall, resulting in a final sample of 68 participants (for details see Table 1; controls n = 48, patients n = 20). In the group of patients, 60% reported depression as diagnosis. Other diagnoses were: bipolar disorder, anxiety, adjustment disorder, obsessive compulsive disorder, eating disorder, post-traumatic stress disorder, attention deficit hyperactivity syndrome, and personality disorder.
For the second observation period (Lockdown 2, L2), study materials were sent to 82 participants, (controls n = 33, patients n = 10) between November 11, 2020, and November 27, 2020. Forty-three sent back their materials (for details see Table 1). Again, 60% of patients reported depression as diagnosis. Other diagnoses were: bipolar disorder, anxiety, obsessive compulsive disorder, eating disorder, attention deficit hyperactivity syndrome, and personality disorder.
Sociodemographic characteristics.
| Lockdown 1 | Lockdown 2 | |||
|---|---|---|---|---|
| Patients (n=20) | Controls (n=48) | Patients (n= 10) | Controls (n= 33)ab | |
| Gender | ||||
| Female | 15 (75%) | 43 (90%) | 9 (90%) | 26 (81%) |
| Male | 5 (25%) | 5 (10%) | 1 (10%) | 6 (19%) |
| Age m(SE) | 34.20 (3.13) | 24.88 (1.51) | 25.9 (3.10) | 28.09 (1.45) |
| Education | ||||
| <= 9 years schooling | 2 (10%) | - | - | 2 (6%) |
| Secondary school | 6 (30%) | 3 (6%) | - | 1 (3%) |
| High school grad. | 9 (45%) | 38 (79%) | 5 (50%) | 11 (34%) |
| University degree | 3 (15%) | 7 (15%) | 5 (50%) | 19 (59%) |
| Psychopharmaceuticals | ||||
| No | 8 (40%) | 47 (98%) | 5 (50%) | 29 (88%) |
| Yes | 12 (60%) | 1 (2%) | 5 (50%) | 4 (12%) |
| Alcohol consumption per weekc | ||||
| No alcohol at all | 10 (50%) | 23 (48%) | 5 (50%) | 15 (46%) |
| One unit maximum | 3 (15%) | 12 (25%) | 3 (30%) | 6 (18%) |
| > one unit | 7 (35%) | 13 (27%) | 2 (20%) | 12 (36%) |
| Drug consumptiond | ||||
| No | 19 (95%) | 46 (96%) | 10 (100%) | 33 (100%) |
| Yes | 1 (5%) | 2 (4%) | - | - |
| BMI m(SE) | 21.93 (1.06) | 23.28 (0.74) | 22.45 (0.79) | 23.26 (0.80) |
All three participants reportedly consumed Marihuana only. After exclusion of their data, the overall pattern of results stayed the same (see Appendix, Tables A.10 and A.11).
Pre-pandemic group. Pre-pandemic control group participants (NPP = 33; 27 female, age range 18-36 years, M = 22.27, SD = 4.17) were recruited from a student population of the University of Bonn in 2012 (Voss, unpublished)1 .
Validation sample. The validation sample (N = 151, 80 female) was originally recruited for validation of the LuCiD scale (Voss et al., 2013) and was used here to compare lucidity data from the present study with a pre-pandemic sample.
Study materialsIn the pandemic group, each participant received a paper-pencil folder by mail. The folder contained a self-constructed questionnaire asking for demographic information, the extent of fear of infection with COVID-19, the impact of COVID-19-related limitations in daily life, existential fears, and the extent of personal contacts. Sleep quality was measured using the Pittsburgh Sleep Quality Inventory (PSQI: Buysse et al., 1989). The Beck Depression Inventory II (BDI: Beck et al., 1996), Beck Anxiety Inventory (BAI: Beck et al., 1988), and the Symptom Checklist 90 Standard (SCL-90; Franke, 2014) were used to assess psychiatric symptoms. In addition, the folder contained fourteen lined pages for dream reports, each followed by a Lucidity in Dreams Scale (LuCiD scale, Voss et al., 2013). Results for the PSQI, BDI, BAI, and SCL-90-S are reported elsewhere (Koppehele-Gossel et al., 2022). However, the BDI, BAI, and SCL-90-S were used as indicators of psychiatric characteristics of the present sample.
ProceduresParticipants of L1 were instructed to complete the questionnaires at the beginning of study participation. In addition, they were asked to report one dream per night for seven nights and to complete a LuCiD scale related to the reported dream. After the first week, they were instructed to take a break for one week and again to complete the questionnaires and to collect dreams from seven consecutive nights. The dream reports from both weeks were later combined. The instructions for data collection during L2 were modified so that participants were asked to collect dream reports from 14 consecutive nights. As in the L1 survey, participants were instructed to complete the test battery (PSQI, BDI, BAI, and SCL-90-S), at the beginning of study participation.
Dream codingAll dream reports were screened for words related to COVID-19, disease, and threat using a self-defined coding scheme. The scheme was based on ratings provided by participants (N = 69, 50 female, age 18 - 71, M = 43.42; SD = 15.50) in an online survey conducted via SoSci Survey (Leiner, 2019) at www.soscisurvey.de (see Appendix, Table A.1) who were asked to rate preselected COVID-19-related items and freely name additional items. After screening the dream reports, some additional items were included, resulting in a list of 25 items which were then applied to the dream reports by assigned raters who were blind to group membership und who used automatic screening of reports. In addition, dream reports were manually screened for terms that were not specific to the COVID-19 pandemic situation but were more generally related to threat, fear, and aggression (see Table 2).
Frequencies of COVID-19-related words in dreams reported prior and during the two lockdowns.
| M (SE) | N (%) with score > 0 | M (SE) | N (%) with score > 0 | M (SE) | N (%) with score > 0 | |
|---|---|---|---|---|---|---|
| Sum score of COVID-19-related dream content | 2.96 (0.45) | 45 (66) | 2.95 (0.52) | 32 (74) | 0.42 (0.21) | 6 (18) |
Dream reports from the first lockdown were rated by two independent raters, interrater reliability was r = .76, p < .001. Dream reports from the second lockdown were rated by two other trained, independent raters (interrater reliability was r = .74, p < .001). All discrepancies were discussed until a consensus was reached. Raters also manually screened dream reports for statements suggesting lucidity. Results regarding bad dreams (dream of high negative emotional quality) and nightmares (dream with threatening content resulting in awakening from the dream, Duval & Zadra, 2010) are reported elsewhere (Koppehele-Gossel et al., 2022). In line with common practice (see Antrobus, 1983; Stickgold et al., 1994), the length of the dream reports was determined by word count while filler words, non-dream explanations, interpretations and thoughts were excluded. A minimum word count of 30 words was applied to all analyzed dream reports. Ideally, we would have chosen a 40-word cut-off (Hobson et al., 2000; Rahimi et al., 2015) which has been found to increase the likelihood of representing a REM sleep dream report. However, as it has also been shown that, for example, depressed patients often report dreams with a lower word count (Barrett & Loeffler, 1992), we chose a more inclusive criterion.
LuCiD scaleAlthough participants were instructed to answer one LuCiD scale for each dream report, some participants answered LuCiD scales without reporting a dream or forgot to answer the LuCiD scale. Hence, only LuCiD scales combined with a valid dream report (with more than 30 words) were included in the analyses. One outlier value was identified for the control scale of participant #27 via boxplot inspection, this value was excluded from further analyses (Appendix, Figures A.1 to A.3).
Statistical analysesTo increase statistical power and simplify the interpretation of results, sum values were calculated for all COVID-19-related (“sum score COVID-19-related dream content”) and all threat-related words (“sum score threat-related dream content”).
As the distribution was skewed to the right, distribution-free tests were chosen. Kruskal-Wallis tests and Mann-Whitney-U Tests were computed to analyze differences between groups. Bonferroni-corrected p-values are reported.
For explorative purposes, correlations between the sum score of all COVID-19-related words and the sum score of all threat related words with demographic characteristics, the variables of the self-constructed questionnaire and the psychiatric characteristics (BDI, BAI, SCL-90-S) were computed. For dichotomous variables (gender, wearing a mask, diagnosis, self-infection with COVID-19) point-biserial correlations were computed; for the remaining variables Pearson correlations were computed and uncorrected p-values are reported. Bonferroni correction was applied to prevent overestimation of significant relationships. After Bonferroni correction, the significance level (p = .05*1/29) was adjusted to .0017. To control for the influence of the potentially confounding variables (mean number of given valid dream reports and mean word count), partial correlations were calculated.
To explore general differences between our lockdown samples and the validation sample from Voss et al. (2013), Cohen's d and the confidence intervals of the differences for the three key factors of the LuCiD scale were determined. To check for meaningful differences between the two lockdown groups as well as to contrast the data of patients and controls within each lockdown period, t-tests for independent samples were computed, and Bonferroni-corrected levels of significance are reported. Pearson correlations were again calculated to explore associations between the lucidity dimensions and the psychiatric variables. Using Bonferroni correction, the significance level was adjusted to (p = .05*1/16) .003.
ResultsDream reportsDuring L1, 725 dream reports were collected, of which 582 (80%) contained at least 30 words. During L2, 448 dream reports were collected, of which 368 (82%) contained at least 30 words (see Appendix, Table A.2).
Dream content analysisThe four most frequently named COVID-19 related words during both lockdowns were “COVID-19”, “social distancing”, “masks” and “home office” (see Table 2 and Table 3). “Skiing vacation” and even “mask” was among the ten most frequently named words in the control dreams collected years before the pandemic, albeit with quite low absolute frequencies. Eight themes were identified in all three samples (based on the top 10 namings in each sample), namely “threat”, “worries”, “fear”, “crying”, “frighten”, “accident”, “death” and “weapon”.
Co-occurring words describing the ten most frequently mentioned dream contents in at least two samples.
Note. ✓ = present. ✗ = not present.
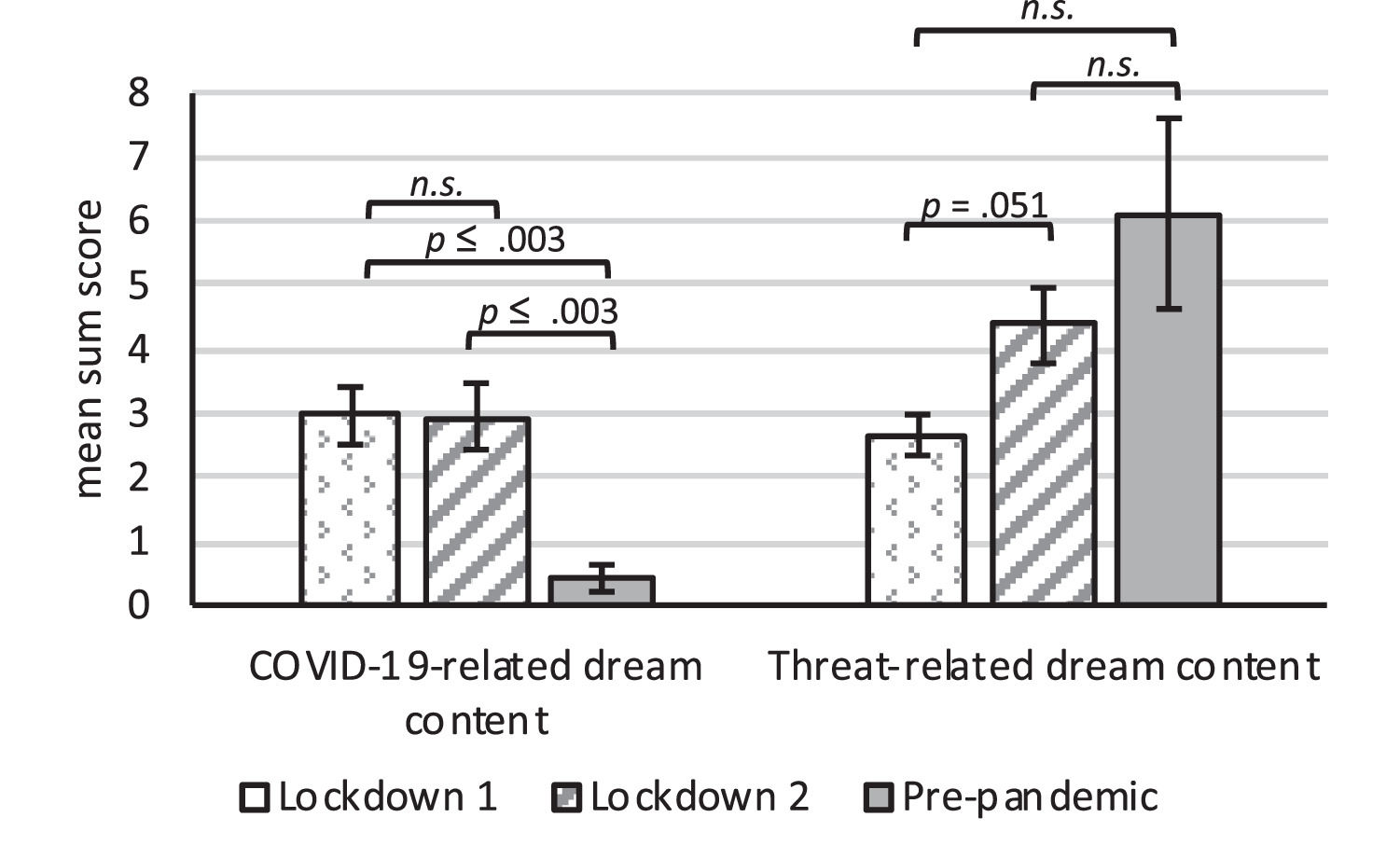
A sum score of all COVID-19-related and all threat-related dream content was calculated and compared between groups (Table 2 and Figure 1). Overall, the pandemic groups differed from the pre-pandemic group significantly in the frequency of COVID-19 related words; Kruskall Wallis H(2) = 26.32, p < .001 with significantly less mentions of COVID-19 words for the pre-pandemic group compared with both lockdown groups; Mann-Whitney U(NL1 = 68, NPP= 33) = 528, Z = -4.60, p ≤ .003; Mann-Whitney U(NL2 = 43; NPP = 33) = 275, Z = -4.87, p ≤ .003. Regarding the summation score of COVID-19 related dream content, no significant differences between Lockdown 1 and Lockdown 2 were found; Mann-Whitney U(NL1 = 68; NL2 = 43) = 1375, Z = -0.536, p > .999. Nonetheless, threat-related dream content differed significantly for the three groups (Kruskal Wallis H(2) = 6.09, p= .048). Pairwise post-hoc analyses revealed a marginally significant difference between the two lockdown groups, Mann-Whitney U(NL1 = 68; NL2 = 43) = 1072, Z = -2.39, p = .051, suggesting less threat-related dream content during the first lockdown. Regarding threat-related dream content, neither of the two lockdown groups differed significantly from the pre-pandemic group; Mann-Whitney U(NL1 = 68; NPP = 33) = 908.50, Z = -1.56, p = .354; Mann-Whitney U(NL2 = 43; NPP = 33) = 690, Z = -0.21, p > .999).
Correlations of dream content frequencies with demographic characteristics, loneliness, pandemic-related fears, and psychiatric characteristics
The sum score of COVID-19-related items and the sum score of threat-related items were correlated with demographics (age, gender, psychiatric diagnosis), the items from our self-constructed questionnaire, fear of becoming infected, impact of COVID-19-related limitations in daily life, anxiety, loneliness, and number and characteristics of personal social contacts (see Appendix, Table A.3). This yielded significant correlations for gender and COVID-19-related items, r(109) = .19, p = .045, with women reporting a higher proportion of COVID-19-related items. Further, threat-related items were positively associated with loneliness; r(109) = .22, p = .021. However, after Bonferroni-Correction (p ≤ 0.0017), both correlations did not remain significant. Both summation scores (COVID-19-related and threat-related) were strongly associated with the number of valid dream reports, i.e. word count ≥ 30 (COVID-19 related dream content: r(109) = .48, p ≤ .001, threat-related dream content: r(109) = .48, p ≤ .001), as well as the mean word count per dream report (COVID-19 related dream content: r(109) = .46, p ≤ .001; threat-related dream content: r(109) = .40, p ≤ .001). The significant association between gender and the number of COVID-19-related items remained even after controlling for the influence of the number of valid dream reports using a partial correlation coefficient: r(108) = .20, p = .041. This also applied to the association between the number of threat-related items and loneliness: r(108) = .23, p = .015. Further, the correlation between loneliness and threat-related items remained significant after controlling for mean word count using partial correlation: r(108) = .25, p = .008. No further correlations between dream content and COVID-19 associated fears, personal contact or any other item of the self-constructed questionnaire reached significance.
There was no significant association between reported psychiatric diagnosis and the sum scores of COVID-19-related and threat-related items. Further, there were no significant correlations between COVID-19-related items and the BDI score, BAI score or the SL-90-S’ GSI and its subscales (see Appendix, Table A.4). Interestingly, however, threat-related items were significantly correlated with depression as measured by the BDI, r(108) = .25, p = .008, as well as the subscales “paranoid ideation”, r(108) = .20, p = .042, and “psychoticism”, r(108) = .19, p = .045. Here, after Bonferroni correction, none of the correlations remained significant.
A qualitative examination of the correlational patterns between the psychiatric variables shows several significant intercorrelations (see Appendix, Table A.5). Notably, the variables “existential anxieties”, “loneliness”, and “number of personal contacts” were highly correlated with indicators of psychological distress. In particular, existential anxieties and loneliness were related to almost all psychiatric variables. Conversely, the number of reported social contacts was related to less psychological distress.
Further, we explored whether psychiatric characteristics could differentiate between the group of participants with versus without COVID-19-related content in their dreams and participants without any COVID-19-reference. This was also explored for the group of participants with any threat-related content and participants without any threat-related content. However, no differences were found (see Appendix, Table A.6 and A.7).
Lucidity and LuCiD scaleOverall, five lucid dreams were reported from four participants, four of which fulfilled the criterion of at least 30 words (see Appendix, Table A.2). Thus, only 0.4% of the dream reports can be considered lucid dreams. For the three key factors of the LuCiD scale (Insight, Control and Dissociation), participants from both lockdowns did not show any significant differences (see Appendix, Table A.8). The scores from each subscale were compared to the scores of the validation sample collected for questionnaire development (Voss et al., 2013). During Lockdown 1 and Lockdown 2, differences between the pandemic samples and the validation sample were found for the subscales Control and Dissociation with lower means for the two lockdown groups compared to the validation sample (see Table 4). Within each lockdown group, the data of patients and controls yielded no significant differences (see Appendix, Table A.8). However, during Lockdown 2, patients showed slightly higher levels of dissociation (M = 1.11, SE = 0.30) compared to healthy controls (M = 0.48, SE = 0.09).
Descriptive statistics and Cohen's d for the LuCID scale differences between the two lockdown groups and the validation sample by Voss et al. (2013).
| Lockdown 1 N = 68a | Voss et al., 2013N = 151 | Confidence interval | |||||
|---|---|---|---|---|---|---|---|
| Subscale | M | SE | M | SE | Cohen's d | lower bound | upper bound |
| Insight | 0.83 | 0.09 | 0.96 | 0.11 | 0.11 | −0.18 | 0.39 |
| Control | 0.38 | 0.05 | 0.78 | 0.09 | 0.42 | 0.12 | 0.71 |
| Dissociation | 0.83 | 0.10 | 1.55 | 0.11 | 0.60 | 0.31 | 0.90 |
| Lockdown 2 N = 43 | Voss et al., 2013N = 151 | Confidence Interval | |||||
|---|---|---|---|---|---|---|---|
| Subscale | M | SE | M | SE | Cohen's d | lower bound | upper bound |
| Insight | 0.92 | 0.14 | 0.96 | 0.11 | 0.03 | −0.31 | 0.37 |
| Control | 0.38 | 0.07 | 0.78 | 0.09 | 0.40 | 0.06 | 0.74 |
| Dissociation | 0.63 | 0.10 | 1.55 | 0.11 | 0.76 | 0.41 | 1.10 |
Note. Outlier value of one participant on the Control scale was excluded.
The exploration of associations between the key factors of lucidity and psychiatric variables revealed no correlations between insight and any of the psychiatric variables (see Appendix, Table A.9). However, significant correlations of control and the SCL-90-S subscales anxiety (r(106) = .22, p = .021) as well as psychoticism (r(106) = .30, p = .001) emerged. Dissociation was related to BDI-depression (r(108) = .29, p = .002), the Global Severity Index of the SCL-90-S (r(107) = .27, p = .005), and its subscales Obsessive-Compulsive (r(107) = .27, p = .005), Depression (r(107) = .26, p = .006), Anxiety (r(107) = .21, p = .033), Anger-Hostility (r(107) = .23, p = .014), Paranoid Ideation (r(107) = .24, p = .012), and Psychoticism (r(107) = .32, p ≤ .001). After Bonferroni-correction, only the correlation of Control and Psychoticism, Dissociation and BDI as well as Dissociation and Psychoticism remained significant.
DiscussionDream contentThe present data suggest that concerns related to the pandemic situation found their way into the dreams of our participants, although only in rather small proportions and not for all participants. Explicit references to COVID-19 were found in 11% of dreams in Lockdown 1 and 8% in Lockdown 2. Overall, these references were observed in 41% of participants in Lockdown 1 and 40% of participants in Lockdown 2. Thus, more than half of both samples did not report having dreamt explicitly about COVID-19. These findings are grossly in line with previous studies which reported COVID-19 incorporations into dreams for 8% to 40% of their participants (Kilius et al., 2021; Musse et al., 2020; Schredl & Bulkeley, 2020) and between 11% to 20% incorporation dreams during the pandemic (Iorio et al., 2020; Parrello et al., 2021) or during other times of crisis, like 9/11 (Bulkeley & Kahan, 2008; Propper et al., 2007).
As the proportion of individuals who included COVID-19 in their dreams was similar in both lockdowns, our findings suggest that the impact of the pandemic on dreams was roughly the same at both time points. Alternatively, the finding could indicate stable individual differences in the propensity to incorporate experienced crises into dreams. As we studied different samples in both lockdowns, we can only speculate about the latter.
A high degree of agreement between the two lockdown groups and the control group regarding dream content was also found for threat-related dream content. Here, the 10 most frequently mentioned terms were the same in all three groups. This indicates a high concordance of threatening dream content across time and context, i.e., not necessarily linked to specific external circumstances such as a pandemic. This is consistent with threat simulation theory (Revonsuo, 2000) in that threats are regular and constant themes in our dreams. Specifically, we found no evidence for a pandemic-induced increase of generic threat themes. Because psychiatric patients, whom we assume to be more susceptible to emotional stressors, did not report more threat-related dream content than controls, our results do not support emotional arousal continuity as proposed by Hartmann and colleagues (Hartmann & Basile, 2003; Hartmann & Brezler, 2008).
Regarding incorporation of COVID-19-related content into dreaming, we found some evidence for incorporation, i.e., explicit references to COVID-19 in the dream reports in our lockdown groups, but not in the control sample collected prior to the pandemic. Thus, our results contrast with previous studies that found no differences between pandemic and control samples (MacKay & DeCicco, 2020; J. Wang et al., 2021). Interestingly, the data from these studies were collected at a fairly early stage of the global pandemic (February 24 to March 12, 2020; MacKay & DeCicco, 2020; February 7 to 27, 2020; J. Wang et al., 2021). Other studies with positive incorporation results were conducted between April and August 2020 (Iorio et al., 2020; Kilius et al., 2021; Parrello et al., 2021; Schredl & Bulkeley, 2020), suggesting that the pandemic took some time to enter dreaming. This pattern seems to be consistent with the so-called “dream-lag” hypothesis, assuming that daytime experiences are either incorporated into the dream immediately or with a certain time lag (Nielsen et al., 2004). While Nielsen et al. (2004) report relatively short time lags for daily events, it is conceivable that more salient events take longer to be incorporated into the dream. With respect to the function of such incorporation, it remains an open question whether the dream facilitates adaptation to a salient life event or whether such an event is only dreamed about once adaptation has been successfully completed. Thus, on the one hand, incorporation of pandemic-related themes could indicate active processing of the pandemic during sleep and support adaptation in the waking state. On the other hand, dream incorporation of pandemic-related themes could reflect completed emotional processing, presenting itself to the dreaming brain to be permanently stored or filed away.
Dream content and demographic characteristics, loneliness, fears related to the pandemic, and psychiatric characteristicsOur explorative investigation of the relation between dream content and sociodemographic variables, loneliness, pandemic-related fears, and measures of mental health yielded only a single significant correlation, namely the one between gender and the frequency of COVID-19-related words. Similar to other studies (e.g., Schredl & Bulkeley, 2020), women reported COVID-19 items more frequently than men. However, in our study, when controlling for the influence of average word count, the correlation between COVID-19-related dream content and gender was no longer significant. Assuming that COVID-19-related words have a higher likelihood of inclusion in longer dream reports, this finding suggests that, at least in our sample, the gender differences regarding the number of COVID-19-related words were based on the longer dream reports of women.
As for threat-related dream content, we found a significant association with the degree of loneliness experienced by our participants, even after controlling for the number of dream reports and mean word count. This result has face validity in that it seems plausible that the pandemic promotes loneliness, which increases stress and negatively impacts mental health, which in turn leads to more negatively toned dreams (e.g. Barrett, 2020; Mota et al., 2020; Rescott et al., 2021; J. Wang et al., 2021). Our data provide twofold evidence for the relationship between loneliness and psychological distress: First, reported loneliness was positively correlated with existential anxieties and most of the collected psychiatric variables, and second, it was negatively correlated with the number of social contacts. Although the results appear consistent in terms of the overall pattern of results, they must be considered exploratory and hypothesis-generating, as they do not withstand a Bonferroni correction given the large number of correlations. Besides loneliness, the amount of threat-related dream content was related to psychiatric variables like depressiveness, paranoid ideation and psychoticism. This again supports the tendency to experience more threatful dreams when participants are under psychological stress.
Dream incorporation, mental health, and the vulnerability hypothesisOverall, we found no association between the presence of a psychiatric diagnosis and incorporation. Also, there were no differences in mental health variables between individuals with and without incorporation (neither for COVID-19-related nor threat-related content). This does not provide evidence for our initially proposed vulnerability hypothesis. Thus, poor mental health status does not automatically lead to an increase in dream incorporation of daily stressors. However, further studies with larger samples with consistent psychiatric diagnoses would be desirable here, as effects may have been masked in our rather small and heterogeneous sample of psychiatric patients.
Lucid dreaming during the pandemicIn our two lockdown samples, only four participants reported a lucid dream (4%) and overall, less than 1% of the collected dreams were lucid ones (see Appendix, Table A.2). These relatively low frequencies are comparable to those of the post-lockdown group of Scarpelli and colleagues (Scarpelli et al., 2021) and our own observations prior to the pandemic (Voss et al., 2009, 2014). However, in contrast to our data, Scarpelli et al. reported an increase in lucid dreaming during the lockdown, suggesting that increased trauma lucidity during lockdown is a coping strategy (Scarpelli et al., 2021). Our own data provide no further support for this interpretation. It is possible that these different results were due to different procedures. Whereas Scarpelli et al. (2021) assessed lucidity with a single question that was not verified by the dream report, our data are based on the statement that the dream was lucid plus a verification through evidence of lucidity in the dream report. Future studies could specifically address possible discrepancies between questionnaire data and dream reports.
Regarding the three key factors of lucidity, namely Insight, Control and Dissociation, no differences were found between the two lockdown groups in the present study. Further, the core criterion of lucidity in dreams during both lockdowns, i.e. Insight, was similar to pre-pandemic levels. However, both lockdown groups differed significantly from the validation with regard to Control and Dissociation, both exhibiting lower values during the pandemic, at least in healthy controls. As lucid dreams must be considered hybrid states with elements of waking and sleeping, this finding suggests that dreams during the pandemic may have been slightly less fragile and more robust. Assuming that dreaming facilitates adaptation (Revonsuo et al., 2015) and emotional consolidation (Voss & Klimke, 2018), we must assume that prolonged periods of crisis, such as the pandemic, require higher levels of processing and may deepen dream sleep, at least in psychologically healthy individuals and in the absence of nightmares. This is in line with a study by Pépin et al. (2021) who observed more REM sleep, less slow wave sleep and more light sleep during the pandemic. Prolonged REM sleep could intensify bizarre dream experience and foster the emotional consolidation process. Further, the reduction of slow wave sleep reported by Pépin et al. (2021) is also in agreement with our finding of reduced lucidity, as our lucid dreamers from previous studies indicated that adequate sleep is a highly favorable, if not necessary, condition for lucidity while dreaming (unpublished). However, differences between pre-pandemic and pandemic levels of lucidity were very slight. Moreover, lucidity in general was very low, similar to previous studies (Gott et al., 2021; Voss et al., 2009). As spontaneous lucidity in dreams mainly occurs in children (Saunders et al., 2016; Voss et al., 2012) and in adults usually requires training, this result seems plausible. Interestingly, patients reported higher levels of dissociation in dreams compared to controls suggesting that adult psychiatric patients may be more susceptible to full lucidity in dreams if trained in such way.
ConclusionWith respect to dream content, our study supports the incorporation approach to dreaming, which assumes that salient events in waking life find their way into dreams, at least to a moderate degree, at least in some individuals. Assuming that dreaming serves the function of emotional processing and consolidation, we interpret this finding as evidence of adaptation or at least an adaptation attempt. While women seem to be more inclined to incorporate, this effect was confounded with the more elaborate dream reports of female participants. Loneliness, a phenomenon fostered by the social restrictions during the pandemic, seems to be associated with threat-related dream content, independent of mental health, gender, and age. While overall dream lucidity is similar to pre-pandemic levels, the dimensions “dissociation” and “control” were reduced in our samples. As other authors have reported an increase in REM sleep during lockdowns, we are inclined to interpret our findings in line with our hybrid idea suggesting that lucid dreaming represents a fragile state of REM sleep. During times of crises, the need to engage in robust and non-lucid dreaming may be heightened and with such, dream lucidity may be lessened.
U.V. and J.K.-G. designed the study. L.-M.W., U.V. and J.K.-G. collected the data. U.V. and J.K.-G. analyzed the data. U.V., A.K., S.W. and J.K.-G. wrote the manuscript. All of the authors discussed the results and commented on the manuscript.
No external funding.
The authors thank Alina Erb and Noah Mba for help in dream coding as well as Maria Ruse for assistance in data entry.
